
Abstract
Extramedullary plasmacytoma (EMP) is a tumor characterized by plasma cell proliferation in organs or tissues outside the bone marrow. It originates from B lymphocytes and can occur in all extramedullary tissues and organs of the body. Primary EMPs of the nasal cavity are relatively rare and mostly presented as case reports. Nasal EMP usually manifests as nasal obstruction, epistaxis, and progressive dyspnea. A 64-year-old man was admitted to our hospital because of rhinorrhagia with nasal obstruction. Computed tomography (CT) revealed a mass in the right nasal passage, which we resected under nasal endoscopy. At the 2-year follow-up, positron emission tomography/CT showed osteolytic bone destruction in the third cervical vertebra and its accessories, accompanied by increased metabolism. We considered the possibility of progression to myeloma, but the patient refused another puncture biopsy. We reviewed the literature for the clinical characteristics and CT findings of 14 patients pathologically confirmed with EMPs of the nasal cavity. All patients had nonspecific clinical manifestations, such as nasal obstruction and epistaxis. Computed tomography mostly showed a uniform-density polypoid mass in the nasal cavity. Therefore, nasal EMP should be included in the differential diagnosis of nasal polyps and other nasal tumors.
Introduction
Extramedullary plasmacytoma (EMP) is a type of isolated plasma cell tumor characterized by plasma cell proliferation in organs or tissues outside the bone marrow. It originates from B lymphocytes and can occur in all extramedullary tissues and organs of the body. Approximately 60% of cases arise in the nasal cavity, paranasal sinus, and nasopharynx, while other sites include the larynx, oropharynx, skull base, gastrointestinal tract, and pelvic cavity. 1 Nasal or nasopharyngeal EMP is mostly a highly differentiated malignant tumor. It shows a predilection for men aged over 50 years, and its most common clinical features are nasal congestion, epistaxis, dyspnea, and local pain. Due to the rarity of this disease, the clinical diagnosis and treatment are challenging. Here, we report a case of EMP confirmed by pathology after surgical resection under nasal endoscopy. The purpose of this report is to share a clinical experience of the diagnosis and treatment of EMP and describe its computed tomography (CT) features for differentiation from other nasal space-occupying lesions. In addition, we provide a literature review and summarize the information in Table 1.
Clinical Features of the Cases of Extramedullary Plasma Cell Tumor of Nasal Cavity From the Literature.
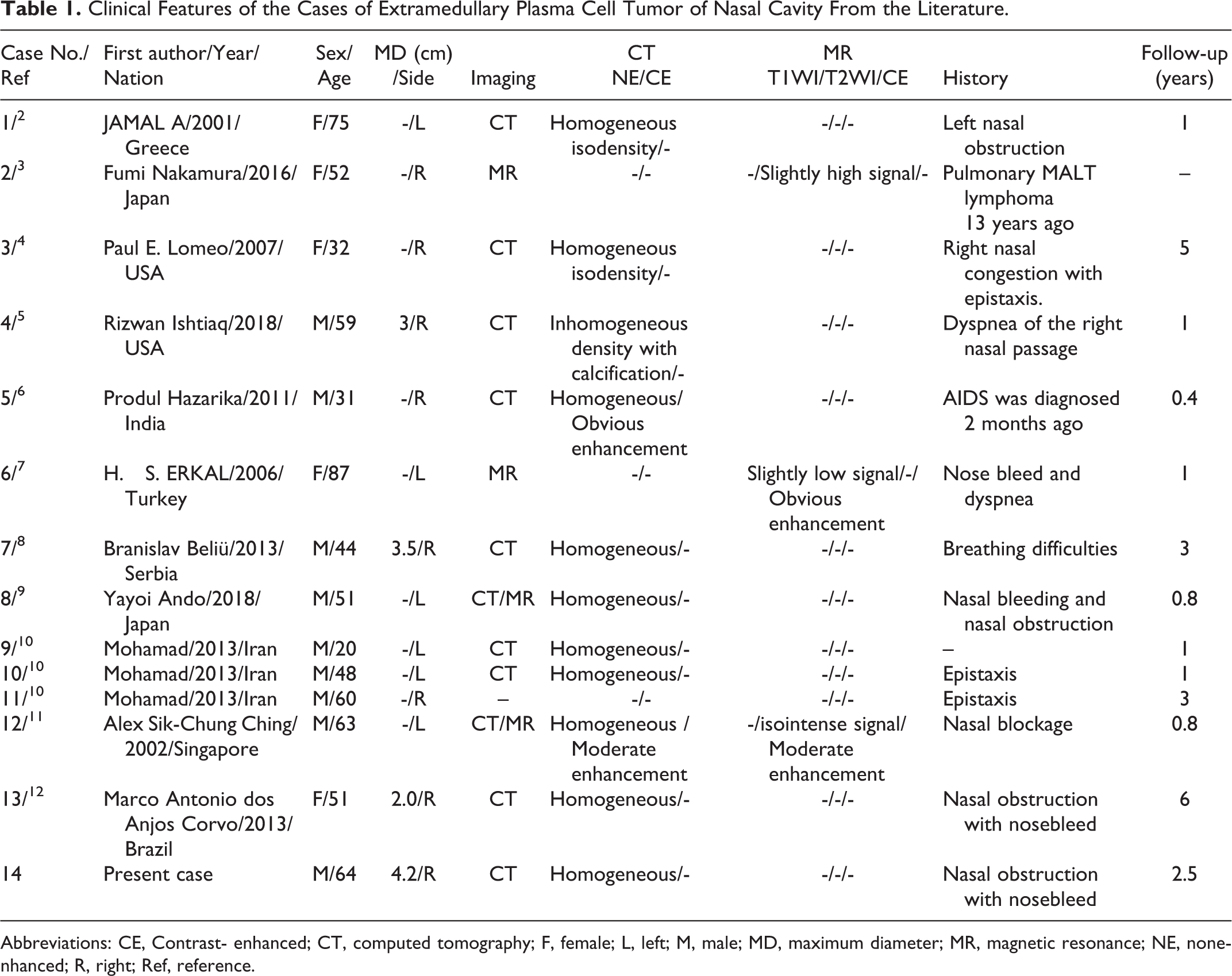
Abbreviations: CE, Contrast- enhanced; CT, computed tomography; F, female; L, left; M, male; MD, maximum diameter; MR, magnetic resonance; NE, nonenhanced; R, right; Ref, reference.
Case Report
Patient Information
A 64-year-old man was admitted to the hospital because of epistaxis for 2 months, which had become aggravated and accompanied by nasal congestion for 15 days. Over 2 months, the patient had developed epistaxis, cough, sputum (occasionally bloody sputum), dizziness, headache, and a decreased sense of smell without obvious inducement. Ten days before presentation, the aforementioned symptoms had aggravated significantly, accompanied by nasal congestion and nasal odor, without discomforts, such as dry nose, nasal itching, or nasal pain. The patient had taken no symptomatic treatment during the disease course. He was admitted to our otolaryngology outpatient department for further diagnosis and treatment.
Physical Examination
Physical examination revealed no external nasal collapse, no nasal stenosis, chronic congestion of the bilateral nasal mucosa, red purulent secretion outflow in the right nasal cavity, new biological stuffing, with the biological source unknown, and bleeding on touch. Furthermore, we found left nasal cavity inferior turbinate hypertrophy, without new organisms, purulent secretion, or deviation in the nasal septum.
Computed Tomography Examination
Computed tomography revealed bilateral maxillary sinus mucosal thickenings, uneven densities of the right maxillary sinus and nasal passages, and suspected space-occupying lesions accompanied by epistaxis. Bone resorption was observed in the medial wall of the right maxillary sinus. The left middle and lower turbinates showed hypertrophy (Figure 1).
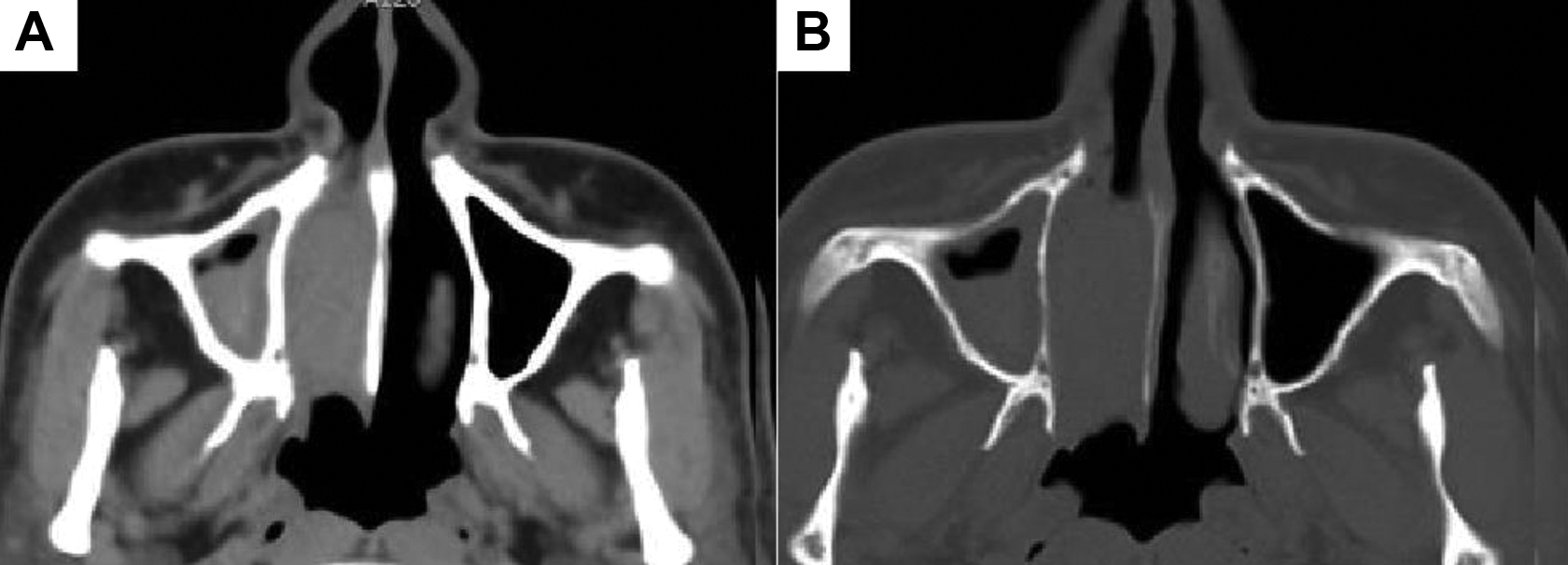
A, CT soft tissue window of the sinus showed thickening of the mucosa of the right maxillary sinus, and polypoid soft tissue density shadow was seen in the right nasal cavity, about 4.2 cm × 2.5 cm × 2.0 cm in size (anteroposterior diameter × transverse diameter × upper and lower diameter). B, CT bone window of the sinus showed partial bone absorption in the medial wall of the right maxillary sinus. CT indicates computed tomography.
Surgical Findings
Endoscopic examination revealed a dark-red neoplasm in the right nasal cavity, protruding into the posterior nostril, partially necrotic, originating from the natural mouth of the maxillary sinus in the middle nasal passage. The uncinate process was resected, and an enlarged maxillary sinus orifice and sinus cavity effusion were seen. In addition, polypoid masses were observed in the mucosa of the sinus cavity. In the process of tumor removal, the polypoid tissue in the sinus cavity was removed with a disposable knife head, and maxillary sinus orifice was further enlarged. Subsequently, the cavity was irrigated with Teshu, and collagen and gelatin sponges were stuffed. Thus, the operation was completed.
Histopathological Examination
Light microscopy revealed ciliated columnar epithelium on the tumor surface and diffusely arranged plasmacytoid tumor cells in the stroma. The nuclei were enlarged and partial on 1 side. Local bleeding and necrosis were seen. Immunohistochemical staining showed positive expressions of CD79a, CD138, CD56, 30% Ki-67, and vimentin in tumor cells, while negative expressions of other tumor markers. Based on these characteristics, the pathologist diagnosed the patient with EMP of the right nasal cavity (Figure 2).
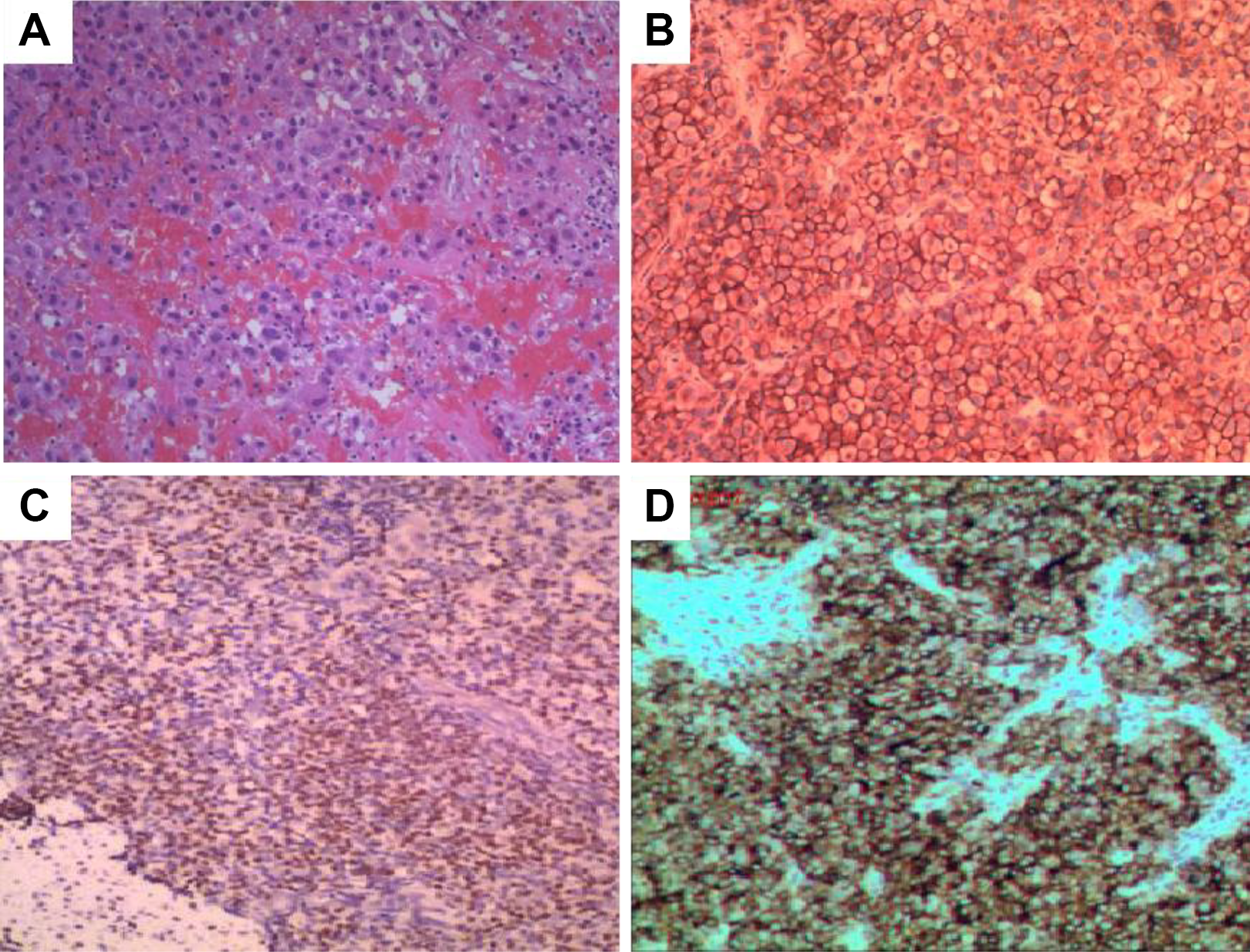
A, (HE ×100), The tumor cells are diffused and arranged, and the tumor cells are round, uniform in size, abundant in cytoplasm, and interspersed with small lymphocytes. B, Immunohistochemical staining showed positive CD138. C, Immunohistochemistry showed that the tumor cell CD56 was positive. D, Immunohistochemistry showed positive Vimentin in tumor cells.
Literature Review
English case reports and case series of nasal EMP published in PubMed, Web of Science, and Science Direct databases before June 30, 2020, were searched. The search items were (Nasal Cavity OR Nose) AND (Extramedullary Plasmacytoma OR Extramedullary Plasma Cell Tumor). The literature was gradually screened, and a total of 11 full-text articles, including 13 patients, were extracted. The first author, year of publication, country, patient age and sex, mass size, side of onset, imaging features, clinical history, and follow-up duration were recorded (Table 1). Figure 3 shows the scatterplot of the sex, affected side, and age of 14 patients (including our case) with nasal extramedullary cell tumor. There were 9 men and 5 women, showing a significant difference. The onset age in men was 20 to 64 years, and median onset age was approximately 48.9 years. The onset age in women was 32 to 87 years, and median onset age was 59.4 years. There was no significant difference in the incidence on either side of the nasal cavity. Clinical symptoms of the 14 patients with EMP of the nasal cavity mostly included nasal obstruction, epistaxis, and dyspnea. Some patients had a history of malignant tumor chemoradiotherapy. Imaging manifestations of EMP in the nasal cavity are mostly soft tissue masses with a uniform density or signal, but less calcification or cystic necrosis, contrary to the imaging manifestations of most malignant tumors.
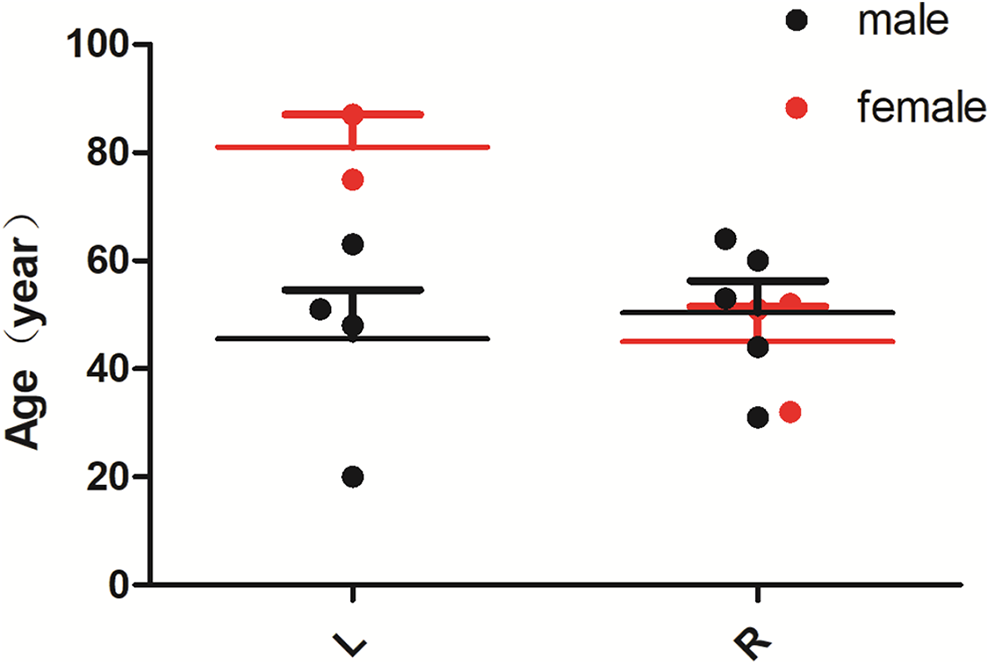
The scattered distribution of gender, diseased side, and age of EMP in 14 cases.
Discussion
Clinical Features, Diagnosis, and Treatment of Nasal EMP
The present patient was routinely followed-up with CT for nasal meatus hemorrhage. Since the CT scan showed a soft tissue mass shadow with a uniform density in the right nasal cavity, we first considered the possibility of benign lesions, such as nasal polyps or inverted papilloma. However, the postoperative pathology confirmed EMP of the nasal cavity, highlighting our lack of the clinical knowledge of this disease. Plasmacytoma is a malignant plasma cell tumor that grows in the soft tissue or axial skeleton. EMP is a subtype of plasmacytoma that arises mostly in the upper respiratory tract but can arise in any other body part. 1 The diagnosis of this disease mainly depends on histopathological examination. Under microscopy, it mainly manifests as an isolated lesion composed of the proliferation of monoclonal tumor plasma cells with different degrees of differentiation. Immunohistochemistry can exclude multiple myeloma or other nonneoplastic plasma cell hyperplasia. On CT, most lesions show uniform isodensity with a clear boundary and uniform contrast enhancement after contrast media administration. Only a few lesions show significant uneven enhancement, while the surrounding bone usually shows expansion, deformation, and absorption, with minor local damage. 13 Computed tomography findings of the present patient were roughly consistent with those previously reported. However, the patient refused to undergo contrast-enhanced CT, so more imaging evidence for this disease was not obtained. Extramedullary plasmacytoma is generally diagnosed based on the following criteria 14 : First, the lesion should be located in an organ or soft tissue other than bone tissue and pathologically confirmed as an isolated extramedullary lesion consisting of neoplastic plasma cells; second, plasma cell tumors of the bone marrow should be excluded, or the percentage of plasma cells in the normal bone marrow should be less than 5%; finally, systemic examinations, such as bone marrow biopsy and imaging, should be performed to exclude multiple myeloma and isolated bone plasma cell tumors. Due to the rarity of EMP, there is no uniform clinical treatment principle, although EMP is known to be sensitive to radiotherapy. 15 Therefore, combined radiotherapy can be performed after complete surgical resection to achieve a better prognosis. Figure 4 shows the survival rate of the enrolled patients (13/14). The mean survival rate was 3 years, and survival rates were not significantly different between men and women. All 12 of the 14 patients underwent surgery plus radiation therapy, except for 2 patients who could not undergo surgery because of old age. The patient outcomes were relatively satisfactory, with 2 patients still alive and healthy over more than 5 years of follow-up. Approximately half of the cases of EMP eventually progress to multiple myeloma. 1 After 2 years of follow-up, our patient underwent positron emission tomography/CT, which showed that the C3 vertebral body and its accessories had low-density bone destruction, and vertebral body metabolism had significantly increased. This suggested the possibility of conversion to myeloma. However, the patient refused to undergo further biopsy, so the final pathology result could not be obtained.
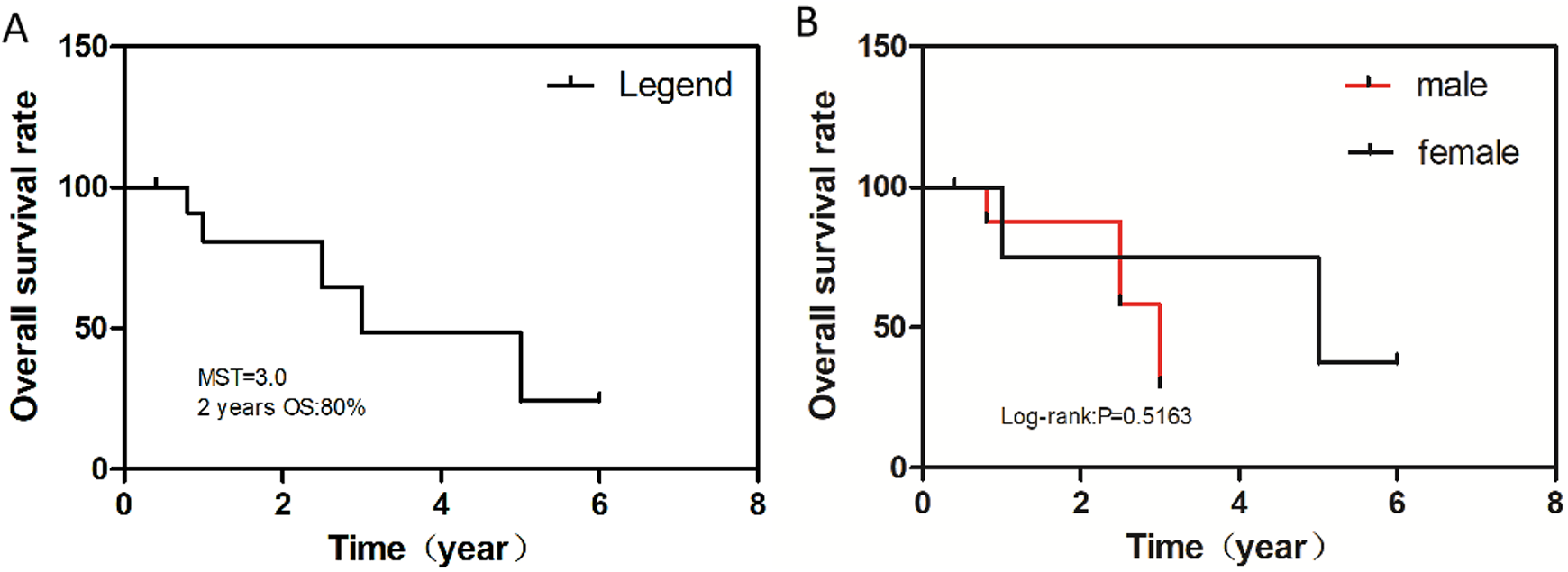
Kaplan-Meier OS. A, OS in all cases. B, OS by gender. MST indicates median survival time; OS, overall survival.
Differential Diagnosis of Nasal EMP
According to the clinical characteristics and imaging manifestations of isolated EMP in the nasal cavity, it should be differentiated from nasal polyps, inverted papilloma, lymphoma, adenocarcinoma, and so on. Nasal polyps are more likely to occur in the common areas of the oral and nasal passages of the sinuses. They are mostly bilateral, with a pale or reddish appearance. Pathologically, nasal polyps are granulomatous lesions caused by edema and mucosal accumulation of hyperplasia, when they occur unilaterally. Computed tomography shows a soft tissue mass with a slightly low density or an equal density relative to the nasal cavity. This mass can easily lead to narrowing or complete obstruction of the nasal cavity and cause sinusitis. The ethmoid bone and nasal septum in the adjacent sinus wall are compressed toward the healthy side. Some patients may manifest with similar malignant tumor signs, such as bone absorption or destruction. It is difficult to differentiate EMP from other polypoid masses. Most cases of inverting papilloma arise in the area near the middle nasal passage of the lateral wall of the nasal cavity. The typical CT features are mainly soft tissue lesions in the nasal cavity and paranasal sinus. The mass density is relatively uniform, and early lesions are relatively small. Most cases arise unilaterally. Lesions can grow toward the maxillary sinus, ethmoid sinus, or in other directions and the turbinate and nasal septum shift under pressure, causing the expansion of the natural orifice of the nasal canal.13,16 Simultaneously, the involved sinus wall can show hyperosteogeny, invasion, and destruction. Most cases of nasal lymphomas are non-Hodgkin’s lymphoma. Nasal lymphomas can be divided into 3 types according to the immunohistochemistry: B, T, and NK/T cells (most common). It is difficult to differentiate nasal lymphomas from other nasal polypoid lesions in the early stage without infiltrating nasal soft tissue or causing tissue necrosis because of the destruction of the nasal midline structures. 15 Most cases of nasal adenocarcinoma occur in patients aged over 50 years. Computed tomography often shows a soft tissue mass in the nasal cavity that can spread to adjacent sinuses. As the disease progresses, the mass density may become uneven because of hemorrhage and necrosis. The surrounding bone structure is often invaded, resulting in osteolytic bone destruction. Additionally, some malignant tumors of the nasal cavity, such as melanoma and peribulbar cell tumor, may show a polypoid soft tissue mass in the early stage. Therefore, fully understanding the clinical characteristics and imaging features of various tumors of the nasal cavity is helpful for differentiating these rare tumors in clinical practice.
Conclusions
Computed tomography findings of EMP include a homogeneous soft tissue mass in the nasal cavity, with less calcification or cystic necrosis, similar to benign tumors, so it should be included in the differential diagnosis of nasal polyps and inverted papilloma. Clinical features and imaging findings of nasal EMP are nonspecific, but CT is of great significance in determining the location, scope of involvement, and other accompanying lesions of the tumor. In particular, due to nasal obstruction caused by the tumor, nasal endoscopy is usually difficult to perform, and CT can provide clinicians with the diagnosis and treatment plan. The final diagnosis of nasal EMP depends on the pathology and immunohistochemistry, and postoperative radiotherapy can improve the prognosis.
Supplemental Material
Supplemental Material, sj-doc-1-ear-10.1177_0145561320960005 - Extramedullary Plasmacytoma of Nasal Cavity: A Case Report and Literature Review
Supplemental Material, sj-doc-1-ear-10.1177_0145561320960005.doc for Extramedullary Plasmacytoma of Nasal Cavity: A Case Report and Literature Review by Xianwen Hu, Chaoyan Peng, Pan Wang and Jiong Cai in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
All procedures carried out in the study met the ethical standards of the National Research Council as well as the Declaration of Helsinki and its subsequent amendments or similar ethical standards. The patient’s oral and written informed consent was obtained for this case report and related pictures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.