
Abstract
Objective:
To report a case of a recurrent intramuscular hemangioma (IMH) of the lower lip of a 68-year-old female and review the published literature to provide an overview of the presentation, diagnostic strategy, pathological classification, and management of these lesions within the oral cavity.
Methods:
A case report was conducted by reviewing the documentation at a single institution. A systematic literature review on OVID MEDLINE and PubMed was performed using the MESH terms “intramuscular hemangioma” and “oral cavity,” “tongue,” “cheek,” “buccal,” “gingiva,” and “lip.”
Results:
A 62-year-old female presented to our institution with a 2 × 2 × 1 cm IMH of the lower lip involving the surrounding orbicularis oris muscle. She underwent a submucosal resection and did well postoperatively. Six and a half years later, she represented to our institution with a new lower lip lesion in the area of her previous resection. Preoperative magnetic resonance imaging showed a new 10 × 11 mm lesion with a well circumscribed central component surrounded by ill-defined tissue. Preoperative angiography showed that the lesion was supplied by vessels branching off the left facial artery, which were embolized. She underwent wide-local excision (WLE) with bilateral advancement flaps and at her 2-month postoperative visit has not had recurrence.
Conclusion:
Only 39 cases of IMH in the oral cavity have been reported, with only 3 others occurring in the lower lip. Here we add the first case of an IMH of the oral cavity that recurred after primary WLE. The patient was successfully retreated with WLE. At a 3-month follow-up visit, she noted some incompetence with oral secretions and occasional tingling along the incision site but no evidence of recurrence.
Introduction
Intramuscular hemangioma is a rare, benign, soft tissue tumor that constitutes roughly 1% of all cases of hemangiomas. These lesions predominantly arise in the extremities or trunk; however, 15 to 20% occur in the head and neck. Within this region, the masseter muscle is the most commonly affected site, followed by the trapezius.1,2 Enzinger and Weiss subclassified these lesions based on the predominant vessel size—capillary (small-vessel type), cavernous (med-large vessel type), and “mixed,” with capillary being the predominant type. Occurrence of these lesions in the oral cavity is extremely rare. 3 These lesions are also frequently referred to as infiltrating angiolipomas (IALs) because of their similar pathological appearance.4,5
In the published literature, a total of 39 cases of IMH in the oral cavity have been reported. There has been no report of an IMH of the oral cavity that recurred after complete wide-local excision (WLE). The purpose of the present report is to document the first know instance of recurrence of IMH in the oral cavity after complete WLE as well as provide an overview of the clinical presentation, diagnosis, and management of these lesions.
Case Report
A 62-year-old woman with a history of goiter and hyperthyroidism presented to our clinic with a firm, fixed, slowly enlarging lower lip which she noticed 3 months prior. She had previously seen an oral surgeon who had attempted an excision but aborted the procedure due to excessive bleeding. A biopsy of the lesion showed a vascular lesion.
She underwent an ultrasound which revealed a poorly defined, nonencapsulated, 2 × 2 cm × 1 cm homogenous echogenic structure. There was no evidence of a pseudocapsule. She underwent successful WLE of the mass which was fibrosed, deep to the dermis, and incorporated into the surrounding orbicularis oris musculature. The area was reconstructed with acellular dermis to provide bulk tissue to the defect area. Final pathological diagnosis was IAL. At her 1-month follow-up appointment, a subcutaneous nodule was noted at the surgical site with persistent numbness of the area.
Over 6 years later, she represented to the clinic with a recurrent central lower lip mass in the area of her previous excision (Figure 1A). She reported the mass became most notable approximately 1 year after her excision and gradually enlarged causing interference with speech and eating. Magnetic resonance imaging (MRI) following this visit showed a new 10 × 11 mm lesion with a well circumscribed central component surrounded by ill-defined tissue (Figure 2). Five months later, she returned to the clinic and was scheduled for re-excision of the mass. Preoperative angiography showed that the lesion was supplied by vessels branching off the left facial artery, and embolization of the vascular component was performed before her procedure (Figure 2B and C). Blunt dissection revealed a 3.5 × 2.0 × 1.5 cm, incompletely encapsulated mass that was removed with good hemostatic control. The defect was reconstructed with acellular dermis and bilateral advancement flaps. Final pathologic diagnosis of the specimen was read as “intramuscular angiolipoma.” At her 6-month follow-up, she noted some issues with oral incompetence in the immediate postoperative period but that had resolved and had no signs or symptoms of recurrence (Figure 1B).
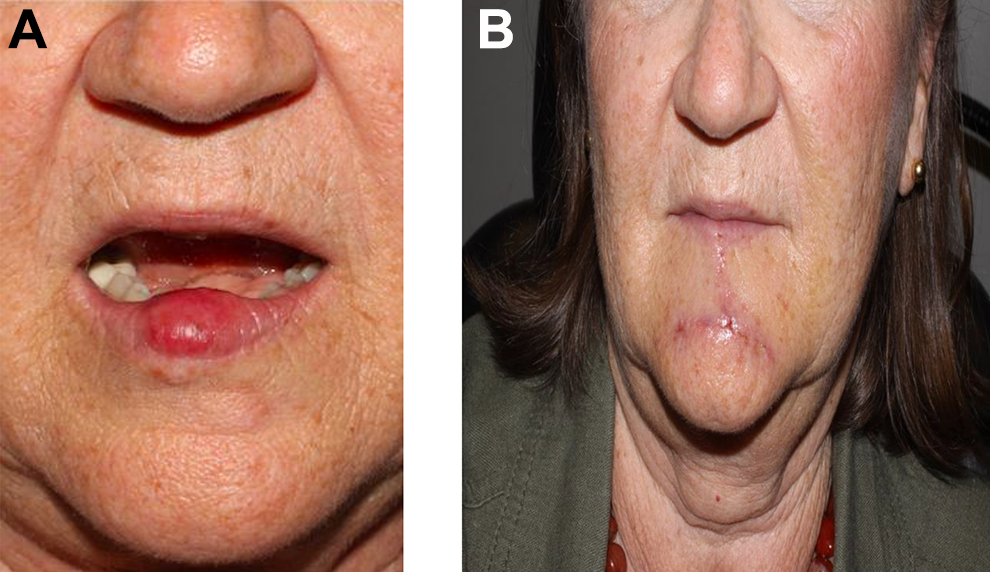
Our 68-year-old female preoperatively (A) and 1 week postoperatively after her second WLE (B). WLE indicates wide-local excision.
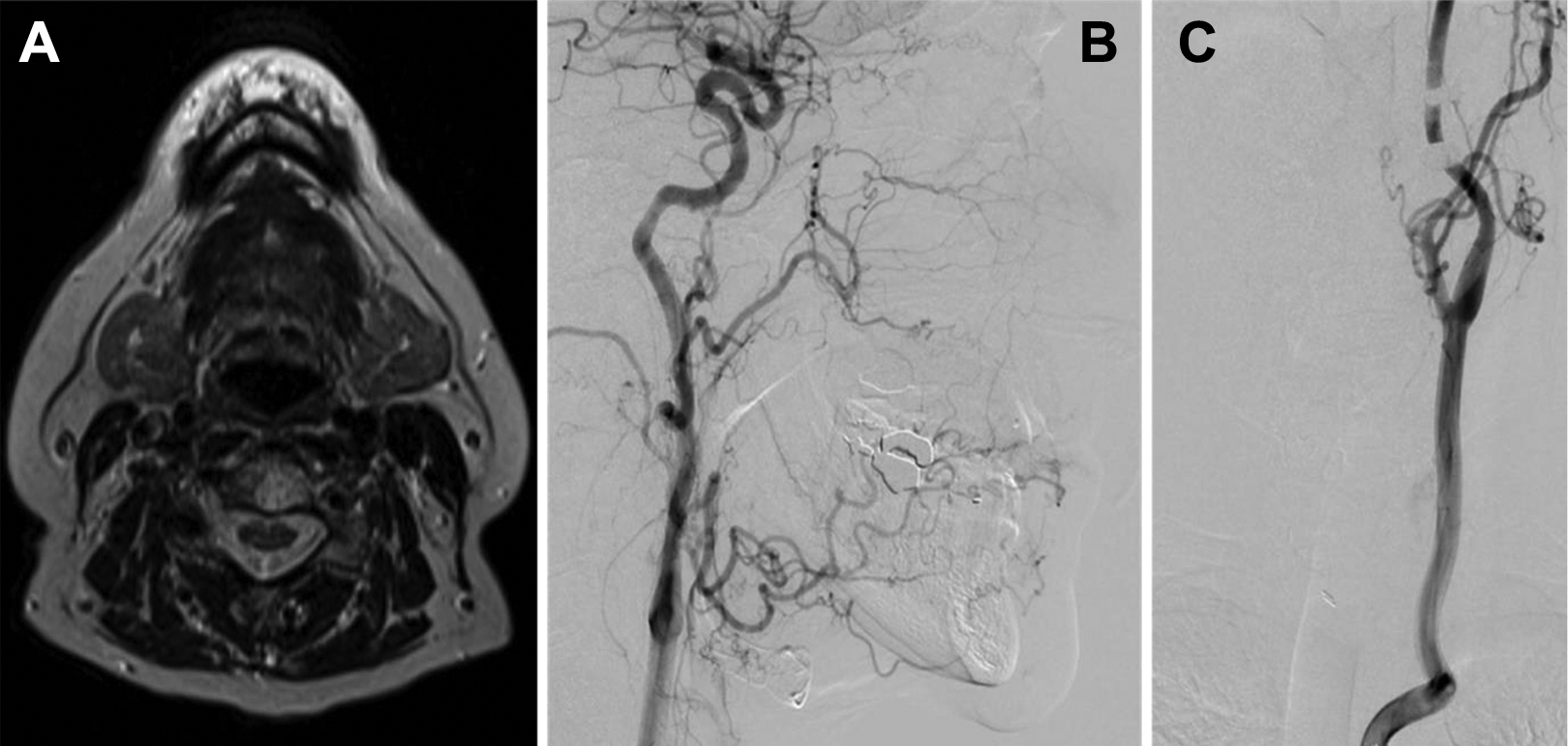
Preoperative magnetic resonance imaging of lesion (A) and magnetic resonance angiography of vessel supplying it (B and C). A, Axial T2 MRI showing a hyperintense lesion of the lower lip. B, Sagittal and (C) coronal planes of the patient’s preoperative angiography that show the lesion being supplied by a branch of the left facial artery. MRI indicates magnetic resonance imaging.
The tumor in this case consisted of a mixture of mature adipose cells and small blood vessels. It was nonencapsulated and demonstrated an infiltrative growth pattern, surrounding and permeating between skeletal muscle fibers. The blood vessels range in size from capillaries to small venules, with focal dilatation. No fibrin thrombi were noted. No cytologic atypia or significant mitotic activity was identified (Figure 3A and B). The findings are consistent with a capillary type IMH.
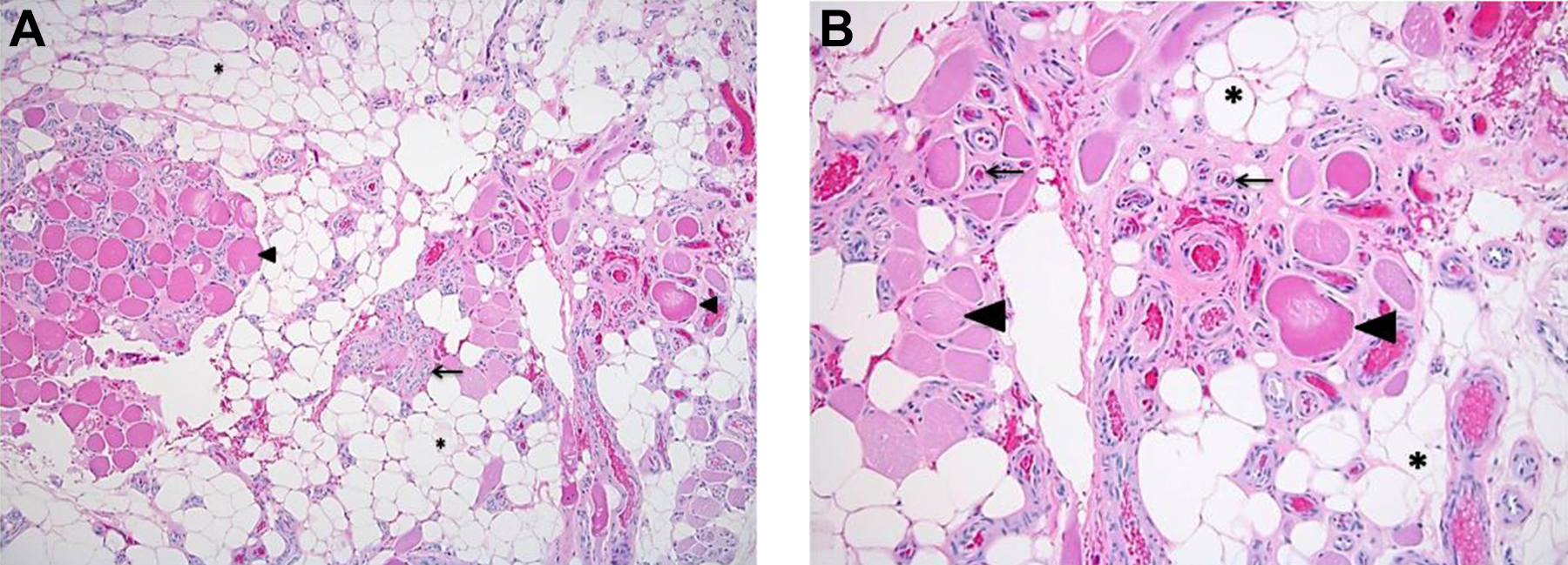
Low-power (left) and high-power (right) magnifications of pathology slides (A) Low-power magnification of H&E stained sample from initially excised lesion. The lesion has a distinct lobular appearance at lower power and consists of a proliferation of thick-walled capillaries (←) among entrapped skeletal muscle fibers (▸), accompanied by mature adipose tissue (*). B, High-power magnification of the same sample revealing similar tissue elements allowing better appreciation of the entrapped and intervening skeletal muscle fibers (←). H&E indicates hematoxylin and eosin.
Discussion
Presentation
Most patients with IMH of the oral cavity present with painless swelling that produces a functional or aesthetic concern. Lesions occurring in the cheek were more often associated with pain but nearly a quarter of the cases did not mention pain in their clinical descriptions. The upper lip was the other subsite where patients presented with pain but the majority of lesions in this subsite were painless.
The mean and median age of presentation was 41.65 and 48 years, respectively. The age at presentation ranged from 9 months to 78 years. Males accounted for the majority of cases in our cohort (65.7%), which is consistent with the previously reported male predilection of these lesions. Furthermore, the mean and median time period of enlargement (defined as the time between when patient’s first reported noticing their lesion to when they first presented) were 56.6 and 24 months, respectively. However, a large range in this time period was noted between 1 and 312 months.4-38 Three patients did not have data on the time period of enlargement, however, one of these individuals was a young adult who noted a lesion in her lip since childhood. 15
There was no relationship between subsites of the oral cavity and histologic subtype. The most commonly affected subsites of the oral cavity were the upper lip (33.3%) and tongue (25.6%). These subsites were followed by the cheek (23.1%), lower lip (12.8%), and upper gingiva (5.1%). Pathologically, the majority of these lesions are categorized as the capillary subtype but nearly a third of them are noted to have mixed vessel sizes. There is no relationship between subsites of the oral cavity and histologic subtype.4-38
Intramuscular hemangioma is typically soft or semifirm to firm masses but their consistencies have a discernable relationship between underlying histologic subtype. These lesions range from being easily mobile to fixed but 60% of reports did not comment on this attribute. Features typically observed in vascular malformations or vascular growths such as palpable pulsations, thrills, or bruits are not a reliable indicator of underlying vascularity for IMH of the oral cavity.
Pathogenesis
The etiology of IMH has not been elucidated. The most commonly referenced mechanism is rooted in the hormone theory which postulates they arise from congenital cutaneous lipomas, which remain dormant until the hormonal influences of adolescence initiate proliferation and differentiation. The appearance of the vascular component has been hypothesized to result from minor trauma and the ensuing fat necrosis with hemorrhagic conversion, all occurring in the context of these hormonal influences.3,39-41 In our review, it was noted that a significant number of patients had lesions present since childhood; however, many of these patients were older and varied with regard to the onset and overall duration of their clinical symptoms. These variations and lack of consistency make it difficult to provide any further insight into the pathogenesis of these lesions.
Diagnostic evaluation
The variability of presentation in terms of history of symptoms and presence or absence of certain physical tumor characteristics makes physical examination an unreliable tool in the diagnosis of these lesions. Tissue samples obtained through excisional procedures are the only means for a definitive diagnosis. Despite the frequent use of fine needle aspiration (FNA), this diagnostic tool has proven largely useless and potentially harmful during workup, especially in patients with lesions who have a prominent arterial component.7,11,12,15,16,33 There was only 1 reported case where FNA correctly led to the diagnosis. 27 While incisional biopsies have yielded correct diagnoses in several cases, these are ultimately futile since the lesions will need to be excised eventually. Additionally, like FNAs, incisional biopsies carry the risk of unnecessary bleeding.
Since it is impossible to have a diagnosis without tissue and in light of the fact that surgical diagnostic can lead to unnecessary bleeding events, imaging studies can be an important tool to help visualize surrounding neurovascular structures at risk for injury before manipulating the lesion.
Magnetic resonance imaging is the gold standard preoperative diagnostic test for these lesions. The T2-weighted images are more useful than T1 and demonstrate a characteristic heterogeneously increased signal within the lesion, reflecting the various tissue components (Figure 2A). Compared with computed tomography, MRI allows better delineation of tumor margins, degree of local extension, and differentiation of tumor components. Use of angiography can be useful for identifying lesions with a prominent arterial supply that are thus better candidates for preoperative embolization.42,43 The differences in utilization of different diagnostic studies are reflective of this difficulty. Care should be taken to fully evaluate the surrounding anatomy with MRI but given the cost of this test, it is not unreasonable to pursue other imaging first.
Preoperative diagnosis of IMH is impossible without tissue specimens. The IMH is a nonencapsulated proliferation of benign vascular channels involving skeletal muscle and deep peripheral soft tissue, accompanied by variable amounts of mature adipose tissue.1,2,40,44,45 Classification of these tumors both by vessel size and by vessel type has been attempted on 2 separate occasions, however on both occasions no clear relationship between vessel size or type and prognosis was identified.3,40 Ninety percent of IMHs include a variably prominent adipocytic component which may dominate the histological pattern, explaining why IMH was sometimes called intramuscular or IAL in the past.2,19,26
The interchangeable use of these 2 different pathological entities, angiolipoma (AL) and IMH, has generated considerable confusion, and the initial diagnosis of “infiltrating angiolipoma” and subsequent diagnosis of “intramuscular angiolipoma” in the present case are illustrative of this. Pathologically, the main distinguishing feature of IMH from AL is that they are not, or are incompletely, encapsulated.26,45 Some case reports describe IMHs within the oral cavity but in some instances the authors note an encapsulated structure or are ambiguous in their pathologic description. 27 Similarly, reports frequently classify AL as either infiltrating or noninfiltrating variants without realizing the former is actually IMH.11,32,34,35 In a recent study, the authors cited just 4 cases of this pathological entity due to this miscategorization. 30 Thus, it is important to recognize that an IAL is actually an IMH and non-IALs are what are recognized as AL.
Management
The mainstay of treatment for these lesions is WLE that includes adequate margins of healthy tissue. An exact margin has not been established but it is clear that incomplete or partial resections have a greater likelihood of recurring.5,46 Preoperative embolization can be considered in instances where there is a prominent vascular component. Given the propensity of these lesions to bleed, excision should be performed in the operating room.
While WLE is the mainstay in treatment, concern for potential cosmetic and/or functional deficits has led some to use laser-based therapies such as sclerotherapy. Some authors have used this technique to shrink larger lesions to make them more easily resectable. Avila and colleagues treated a 4-year-old boy with 3 separate applications of sclerotherapy in 4-month intervals, after which an excision of the remnant tissue was performed. No recurrence was noted at a 2-year follow-up. 6 Similarly, Silva et al employed the same strategy in a 48-year-old woman; however, definitive excision was delayed 3 years after her final sclerotherapy application because symptoms had resolved. The authors did not report recurrence at a specified time period. 36 Lastly, Kucuk et al described the case of a 32-year-old woman who was treated with sclerotherapy for a lesion deep within her tongue. During the first year of her treatment, she received applications of sclerotherapy, and radiofrequency ablation but persistence of the lesion was noted after 2 years. She ultimately underwent WLE 10 months after an attempted partial resection and was not noted to have any recurrence after 6 months. 24 Taken together, sclerotherapy can be considered as a strategy for shrinking lesions in areas that make definitive resection more risky. Nonetheless, given that many of these patients initially present with functional and/or aesthetic complaints as a result of their lesion coupled with the fact that sclerotherapy is not definitive treatment makes sclerotherapy less useful.
Apart from the case reported by Kucuk et al, 2 other cases of recurrence have been reported after initial treatment with partial resection only. Sund and Bang describe a 16-year-old boy who presented with a persistent lesion involving the musculature of his check, lip, and tongue. Prior to the presentation in the report, the boy had undergone 2 prior partial resections at the ages 4 and 15. An additional partial resection was performed at the case report encounter but persistent tissue was noted. No information on follow-up was included. 38
Lastly, Rossiter et al reported a 12-year-old individual who presented with a progressively enlarging upper lip lesion, first noted at the age of 2 years. A partial excision was performed and recurrence occurred 2.5 years later at which point a complete resection was performed. No recurrence was noted 2 years after definitive treatment. 5
The present case has similarities as well as some important differences from previous reports of IMH recurrence in the oral cavity. Most importantly, the recurrence in this instance occurred following WLE with verified adequate healthy tissue margins. While recurrence of IMH has been reported in other areas of the head and neck following WLE, this case represents the first case of recurrence within the oral cavity.5,24,38
Intramuscular hemangioma of the oral cavity presents a diagnostic challenge, and adequate imaging is important for identifying structures and anatomy that are useful for determining operative approach and/or need for preoperative interventions such as embolization. To a lesser extent, diagnosis can be suspected in an individual with a history of a painless, slow, or sometimes quickly enlarging mass. However, given the variability in clinical presentation and the lack of any ostensible correlations between histological type, subsite within the oral cavity, age, or period of enlargement, it is near impossible to diagnose without pathological specimens.
Footnotes
Authors’ Note
This study was presented at the AAO-HNS Conference Meeting; Atlanta, GA; October 7 and 10, 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.