
Abstract
Warthin tumor with ulceration of the surrounding skin is extremely rare, making it difficult to differentiate from parotid cancer in the clinical setting. We report a 65-year-old man with a Warthin tumor in the right parotid gland that had ulceration of the overlying skin. The patient presented with right upper neck mass 2 years ago. Ultrasound and fine needle aspiration were done, and Warthin tumor was suspected. One year later, the mass was enlarged with ulceration of the skin. Superficial parotidectomy with fusiform excision of the skin was performed, and histopathological diagnosis revealed a Warthin tumor with inflammatory change. We proposed that this unique manifestation may have been induced by fine needle aspiration, enlargement of the tumor, and ischemic changes secondary to pulmonary arteriovenous malformations.
Introduction
Warthin tumor is the second most common benign tumor of the salivary glands. It is slightly male predominant, mainly occurring in the sixth to seventh decades and commonly manifests as an asymptomatic and slow-growing 2 to 4 cm mass of the parotid gland. 1 Adenolymphoma, cystadenolymphoma, and papillary cystadenoma lymphomatosum are synonyms of Warthin tumor. Although Warthin tumor is usually considered as a benign lesion, malignant transformation had been occurred in about 0.3% of cases. 2 The gross finding of the parotid tumor in our case showed some of the features of malignancy, including skin ulceration, sternocleidomastoid muscle (SCM) invasion, and tumor bleeding. However, histopathological diagnosis revealed a Warthin tumor with inflammatory change without malignant transformation. Benign Warthin tumor with skin ulceration is extremely rare. To our knowledge, only 7 cases of Warthin tumor with skin ulceration have been reported in the literature. In this article, we report a clinical course of ulcerative Warthin tumor in a 65-year-old man and propose the possible etiologies of skin ulceration. In addition, we make a brief review of the literature.
Case Report
A 65-year-old man presented to our outpatient department with a painless mass in the right upper neck for 6 months. He had a medical history of hypertension for 20 years and pulmonary arteriovenous malformations (PAVMs) in the right middle lobe for 7 years. He used to smoke 2 packs of cigarettes per day for 40 years. An elastic, movable, and nontender mass in the right neck level II was noted on physical examination. Ultrasound showed a hypoechoic lesion, 3.6 × 2.3 × 3.4 cm3 in size, in the right parotid gland, suspected to be a Warthin tumor. Fine needle aspiration (FNA) cytology indicated a benign salivary gland tumor. The patient was kept under observation as he was asymptomatic. The mass became ulcerated 1 year later.
However, this patient did not come back for evaluation until 2 years after the initial OPD visit, when the mass showed significant enlargement with a 3.7 × 3.3 cm2 skin ulceration and intermittent bleeding (Figure 1). Computed tomography demonstrated a tumor in the lower pole of the right parotid gland with an invasion of the skin and SCM and 2 bulky right parotid lymph nodes (Figure 2). The chest X-ray showed one right perihilar nodule, 2.8 cm in size, corresponding to his medical history of PAVMs. Biopsy of the ulcerative mass revealed a Warthin tumor with inflammatory changes. Although parotid cancer with lymph nodal metastases was suggested by the radiologist, Warthin tumor with skin ulceration was impressed. Superficial parotidectomy and fusiform excision of the skin were performed. Gross pathology indicated a tumor, 5.6 × 4.3 × 3.0 cm3 in size, appeared vaguely polypoid, mottled, and light-tan in color. Histopathological sections revealed typical features of Warthin tumor, with foci of squamous metaplasia. The stroma contained dense lymphoid cells, with abundant mature plasma cells and numerous Russell bodies, indicating the presence of chronic inflammation (Figure 3). There was no evidence of malignancy. Warthin tumor with Russell body plasmacytosis and skin ulceration was diagnosed. After the operation, the patient was free of any complaints related to the surgery at 2 years follow-up.

Mass of the right infra-auricular area appeared red and protruding from the ulcerated skin.

Computed tomography (CT) demonstrated one heterogeneously enhancing tumor (5.5 cm × 4.3 cm × 5.0 cm) in the lower pole of the right parotid gland with an invasion of skin and sternocleidomastoid muscle (SCM). Two large lymph nodes were found in the right parotid gland, and the biggest one is 2.5 cm in diameter.
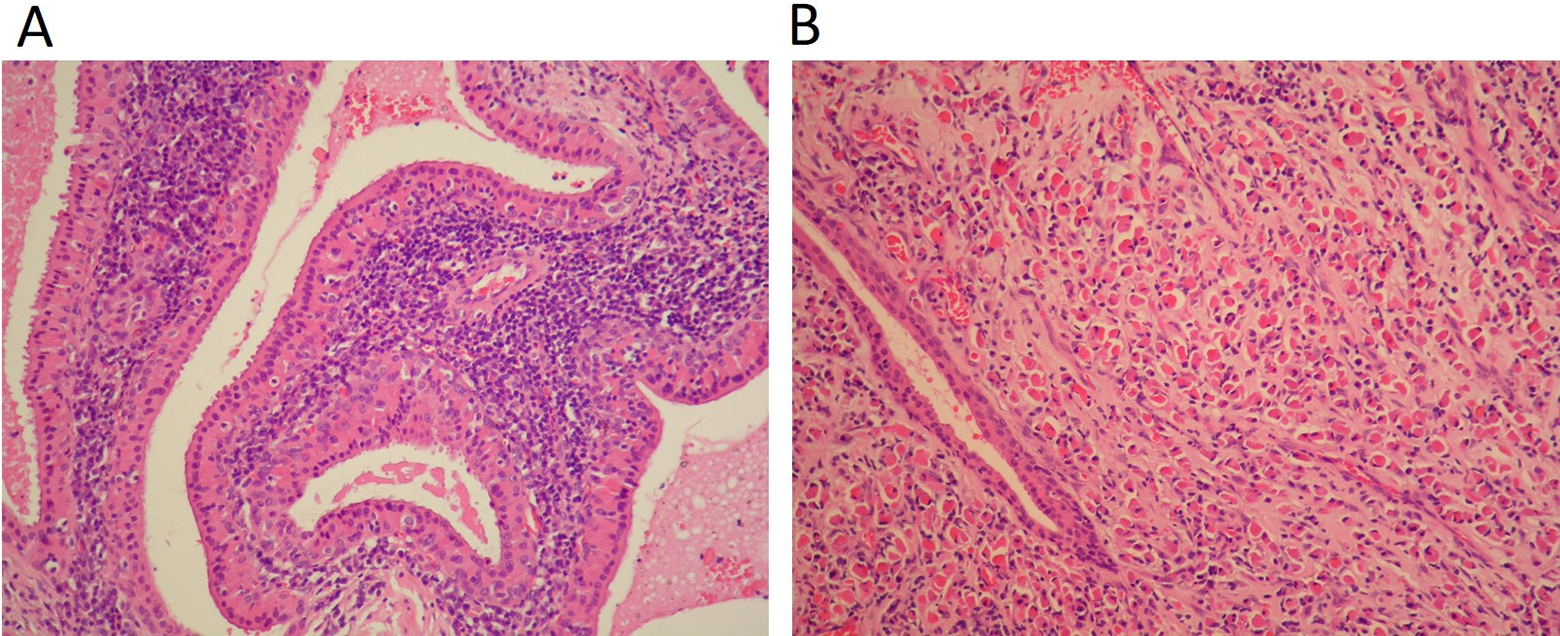
Histopathological section showed papillary-cystic structures lined by oncocytic epithelial cells composed of inner columnar and outer cuboidal cells within lymphoid tissue (hematoxylin-eosin stain; original magnification ×20) (A) and Russell body with plasmacytosis (hematoxylin-eosin stain; original magnification ×20) (B).
Discussion
The malignant transformation of Warthin tumors is extremely rare, with an incidence of about 0.3%. 2 Malignant lymphoma, evolving from the lymphoid components of the tumor, appears to occur more frequently than malignancies arising from the epithelial components. Transformation of epithelial components into adenocarcinoma, mucoepidermoid carcinoma, squamous cell carcinoma, and oncocytic carcinoma had been reported.2-5 In the reported case, the mass appeared to involve the skin, causing ulceration, to invade SCM, and had intermittent bleeding. All these clinical features resembled those of a malignant parotid tumor. However, office-based biopsy, intraoperative frozen sections, and final pathology all showed no evidence of malignancy.
Benign Warthin tumor with skin ulceration is extremely rare. To date, to the best of our knowledge, only 7 cases were reported (Table 1).6-12 Four cases were published in English, 2 in Japanese and 1 in German, respectively. Of the 8 patients, including ours, there were 6 (75%) men and 2 (25%) women with a median age of 75.9 years (range, 63-98 years). The diameter of the tumors ranged from 3.5 to 12.0 cm (mean, 7.2 cm), which is larger than the average size of Warthin tumor. The average diameter of the skin defect was 4.5 cm. The most common clinical presentation was a painless mass (6/8, 75.0%), and 3 cases had tumor bleeding. The exposed tumors were all red. The average time between awareness of the parotid mass and skin ulceration was 9.1 years. Fine needle aspiration was performed in 5 cases for diagnosis.
Overview of Published Cases of Warthin Tumor With Skin Ulceration.
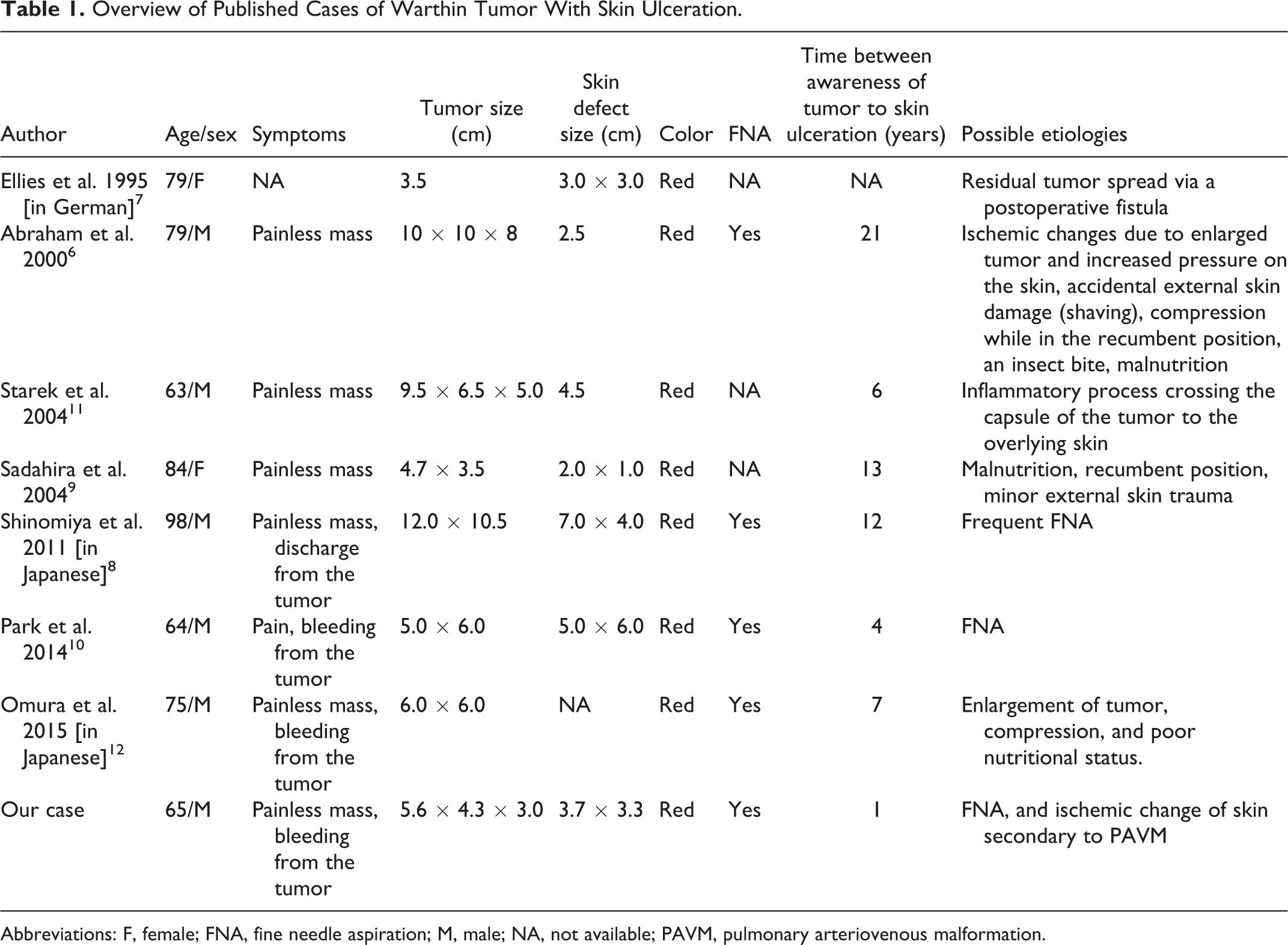
Abbreviations: F, female; FNA, fine needle aspiration; M, male; NA, not available; PAVM, pulmonary arteriovenous malformation.
Several causes of skin ulceration in the Warthin tumor have been proposed. Ellies and his colleagues reported adenolymphoma, a synonym of Warthin tumor, that was not completely removed initially spread via a postoperative fistula to the skin leading to ulceration. 7 Abraham et al speculated that ischemic change due to increased pressure on the skin, accidental external skin damage, compression of the overlying skin while in the recumbent position, insect bites causing minor trauma, and malnutrition might arise the possibility of skin ulcer formation. 6 Sadahira et al considered that malnutrition, the recumbent position, or minor trauma could all have been causative factors for ulcer formation. 9 Fine needle aspiration can cause metaplastic change, necrosis, fibrosis, and inflammatory change in Warthin tumor which has been documented by Di Palma and his colleagues. 13 Hirotaka Shinomiya et al and Park et al suggested that FNA may cause skin trauma and inflammation, resulting in skin ulceration when the tumor enlarges.8,10 In our patient, FNA was done, and the histological examination showed stromal fibrosis, granulomatous inflammation with focal necrosis, and numerous Russell bodies, which indicated chronic inflammation. 14 The findings in our patients supported the notion that FNA may be a causative factor for skin ulceration seen in the Warthin tumor.
Since not all the reported cases have received FNA before, other factors may contribute to skin ulceration in the Warthin tumor. Our reported case had a medical history of PAVMs, which are abnormal communications between pulmonary arteries and veins. Pulmonary arteriovenous malformations cause an intrapulmonary right-to-left shunt, resulting in complications including stroke, brain abscess, and hypoxemia. 15 In fact, our patient suffered an ischemic stroke secondary to embolism from the PAVMs one and a half years after the operation. The peripheral embolic occlusion may be a factor, leading to ischemic skin change and ulceration in our reported case. Interestingly, in our case, the time for the tumor to form skin ulceration was significantly shorter than the average time of other reported cases. We speculated that peripheral vascular insult secondary to PAVMs might accelerate the formation of ulcers.
In conclusion, we reported a case of Warthin tumor with skin ulceration, which is extremely rare. Of the many proposed etiologies, previous FNA, progressive enlargement of the tumor, and possible ischemic insult secondary to PAVMs may serve as contributing factors in our patient. Although Warthin tumor is usually benign, malignant transformation had been reported. To exclude the possibility of malignancy, biopsy of the ulcerative mass preoperatively and frozen section intraoperatively may help the diagnosis and treatment planning. Otorhinolaryngologists also should consider the possibility of a Warthin tumor with inflammatory changes in the differential diagnosis of parotid gland tumors with skin ulceration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.