
Abstract

A 60-year-old woman presented with recurrent episodes of epistaxis of 5 months duration. Each episode started as dull frontal headache followed by severe bilateral nasal bleeding, with blood loss up to 200 mL, which resolved spontaneously. Epistaxis occurred 2 to 3 times a month, and the most recent event had occurred prior to her presentation to the emergency department. Following a similar incident 4 months ago, she developed weakness of the left upper limb for which she was hospitalized and treated for elevated blood pressure. She made an uneventful recovery and had minimal residual deficits of the left arm. She had been on regular treatment for diabetes mellitus and systemic hypertension. There was no recent or remote history of trauma or nasal surgeries.
A complete otorhinolaryngological examination including rigid endoscopy did not reveal any abnormality. Apart from subnormal tone and power in the left arm, neurologic and ophthalmologic examinations were normal. The patient’s hemoglobin level on admission was 5.4 g/dL, and coagulation studies were normal.
A contrast-enhanced computed tomography of the paranasal sinuses demonstrated a small left sphenoid mucosal polyp along with hyperintense mucosal thickening involving the right sphenoid sinus and no obvious bony dehiscence.
Patient was taken up for an endoscopic examination under general anesthesia wherein a pulsatile blood clot was visualized in the lateral wall of the right sphenoid sinus at the opticocarotid recess (Figure 1). Subsequently done cerebral angiogram confirmed the presence of a pseudoaneurysm which measured 1.9 mm at the neck, 1.7 mm at the dome, and 4.6 mm in length, arising from the distal cavernous segment of the right internal carotid artery (ICA) eroding the sphenoid sinus. Following a successful balloon occlusion test with hypotensive challenge, right ICA occlusion was performed using Progreat microcatheter and polyvinyl alcohol particles. Postprocedure, the patient recovered well without any neurological deficit and had no further episodes of epistaxis.
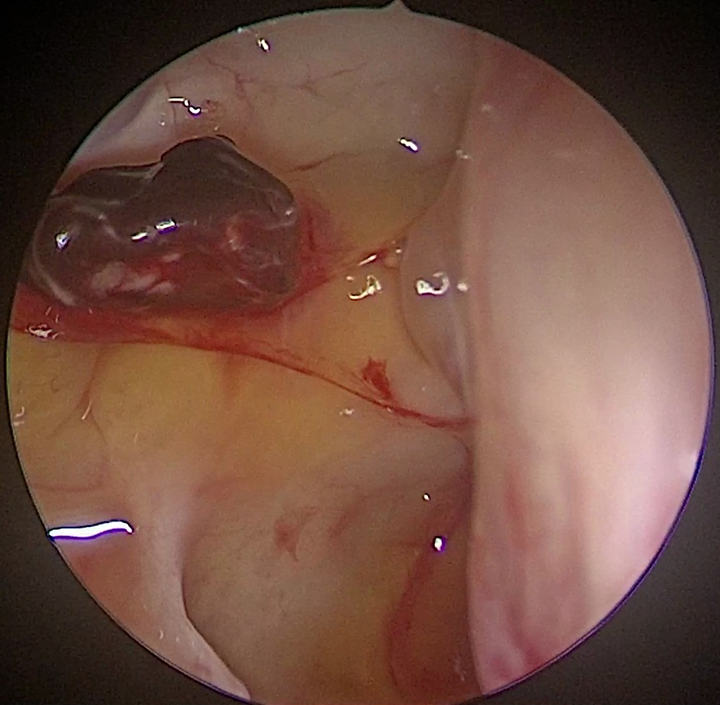
Pulsatile blood clot on the lateral wall of the right sphenoid sinus.
Cavernous carotid aneurysms (CCAs) account for 2% to 8% of all intracranial aneurysms and 14% of aneurysms arising from the ICA.1,2 They can be true aneurysms or pseudoaneurysms. Trauma is the most common etiology for CCAs apart from infectious, iatrogenic, and idiopathic factors.3-5 Reported predisposing factors for the condition include smoking, hypertension, female sex, and patient age more than 50. 2
Mycotic aneurysms could be sequelae of localized arteritis due to intravascular hematogenous spread of septic emboli from bacterial endocarditis or extravascular conditions such as meningitis, sinusitis, and cavernous sinus thrombophlebitis. 5
Traumatic aneurysms follow accidental or iatrogenic trauma to the vessel. These are usually pseudoaneurysms consisting of a hematoma surrounded by a fibrous layer rather than a true arterial wall and is prone to rupture. 6
Nontraumatic CCAs are usually benign asymptomatic lesions, incidentally detected on imaging. 7 Symptoms caused by these aneurysms can be broadly divided into 2 types: compressive and vascular.
Common symptoms due to compression by mass effect of the expanding CCA are headache and diplopia (secondary to third, fourth, or sixth nerve paresis).2,8 It can also cause pain or sensory loss over the distribution of ophthalmic and maxillary divisions of trigeminal nerve and Horner syndrome.
Unlike other intracranial aneurysms, since the cavernous portion of the carotid artery is extradural, CCAs typically do not present with a subarachnoid hemorrhage. Vascular symptoms encountered in CCAs are caroticocavernous fistula, epistaxis, and hematoma formation.
Recurrent, profuse, life-threatening epistaxis can occur in 3% of patients with CCAs owing to the proximity of the cavernous segment of the ICA to the sphenoid sinus. 2 The bony covering is dehiscent in 4% individuals, and in 66%, it is less than 1 mm thick. Nontraumatic CCAs presenting with epistaxis are exceedingly rare. Risk factors for rupture include female sex, symptomatic or multilobed aneurysms, and size larger than 1 cm2. However, posttraumatic pseudoaneurysms of the internal carotid arteries can rupture and cause massive epistaxis with a mortality rate of around 30% to 50%. 1 This generally occurs within 3 weeks of the traumatic event but is sometimes delayed for even years.
Digital subtraction angiography is the gold standard investigation. It helps to determine the origin, configuration, and course of the aneurysm which is critical to plan its management.1,9 On computed tomography, these lesions are mildly hyperintense and sometimes show peripheral curvilinear calcifications. 9 However, small CCAs can be missed by both computed tomography and magnetic resonance imaging scans.
Cavernous carotid aneurysms are managed by endovascular treatment options like primary embolization of the aneurysm using detachable balloons and platinum coils or complete occlusion of the ICA distal and proximal to the aneurysm. 2 Our case highlights that in any patient presenting with spontaneous, large-volume epistaxis, ICA aneurysm is a possible differential that needs prompt evaluation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.