
Abstract
This study presents a case of Extraosseous Ewing sarcoma arising in the cervical esophagus of a 36-year-old woman who presented with cervical mass and dysphagia. Imaging studies demonstrated a well-defined, cystic-solid mass in the neck extending into the upper mediastinum, which results in deviation of the trachea and esophagus. The relationship between the tumor and the cervical esophagus was found in the operation. The patient underwent localized tumor resection without radical esophagectomy. The accurate diagnosis was obtained by the immunohistochemistry and molecular genetic assay. Although this is a rare site for this type of tumor to occur, extraosseous Ewing sarcoma should be considered in the differential diagnosis of small round cell tumors of the cervical esophagus. The postoperative chemotherapy and radiotherapy are of great value in improving the prognosis of cervical esophageal Ewing sarcoma.
Introduction
The esophagus is not a common site for rare tumors. 1 Small round cell tumors of the esophagus are particularly prevalent occurrences that encompass differential diagnosis with small-cell carcinoma and undifferentiated carcinoma being the most common. 1 Recent advances in pathological diagnosis, including immunohistochemistry and molecular genetics, have considerably improved the accuracy of the diagnosis of small round cell tumors. The Ewing family of tumors includes classical Ewing sarcoma and peripheral primitive neuroectodermal tumors, which show various degrees of neuronal differentiation. Ewing sarcomas are a group of small round cell tumors that occur predominantly in the long bones as well as in extraosseous locations such as the extremities, trunk, and retroperitoneum. 2 Extraosseous Ewing sarcoma (EES) is a type of small round cell tumor that occurs in soft tissues. In rare cases, EES occurs in the esophagus.1,3 Here, we present the first report of a cervical esophageal EES confirmed by immunohistochemical and molecular genetic techniques.
Case Report
A 36-year-old female patient presented with a 1-month history of painless left neck mass and dysphagia. She was an otherwise healthy woman with no prior surgeries or chronic medications. There was no family history of obvious abnormalities. Physical examination revealed a smooth, soft, nontender mass on the left side of the neck without any palpable lymphadenopathy. Laboratory investigations were unremarkable. An ultrasound of the neck revealed a huge, cystic-solid, heterogeneous echostructure mass within the left side of the neck posterior to the trachea. Flexible esophagogastroscopy showed esophageal narrowing with an intact mucosal surface at 17 to 22 cm from the incisor teeth (Figure 1). Contrast-enhanced computed-tomography (CT) of the neck and thorax demonstrated a 9.0 × 6.7 × 4.7 cm well-defined, cystic-solid, heterogeneous cervical mass extending into the upper mediastinum with enhancement of the solid part of the tumor, which caused deviation of the trachea and esophagus. There were no pathologized lymph nodes in the neck and mediastinum (Figure 2).
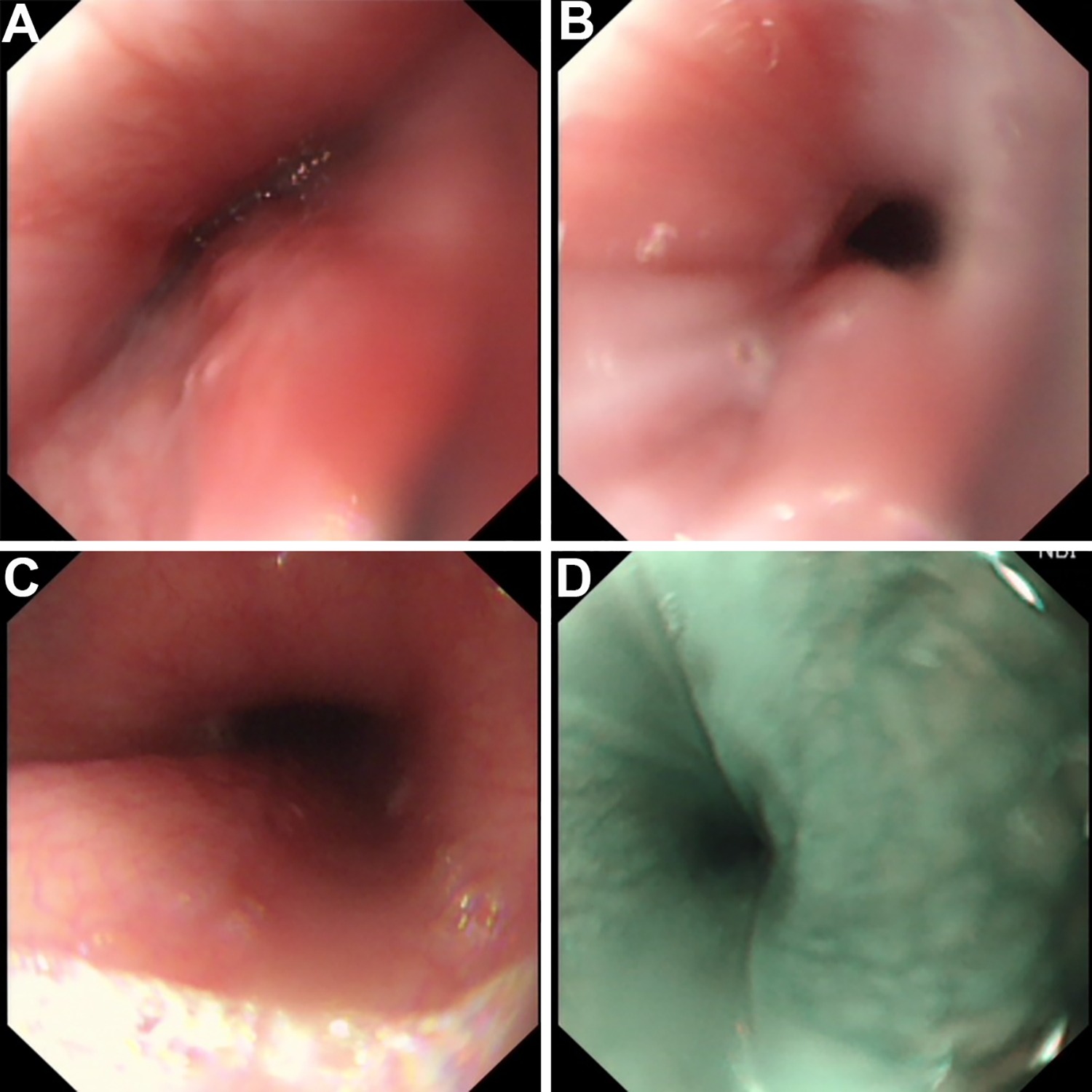
The esophagus in the esophagogastroscopy examination before operation. A and B, The esophageal narrowing with an intact mucosal surface. C, The normal esophagus after narrow section. D, the normal mucosal surface of narrow esophagus in narrow band imaging (NBI) endoscopy.
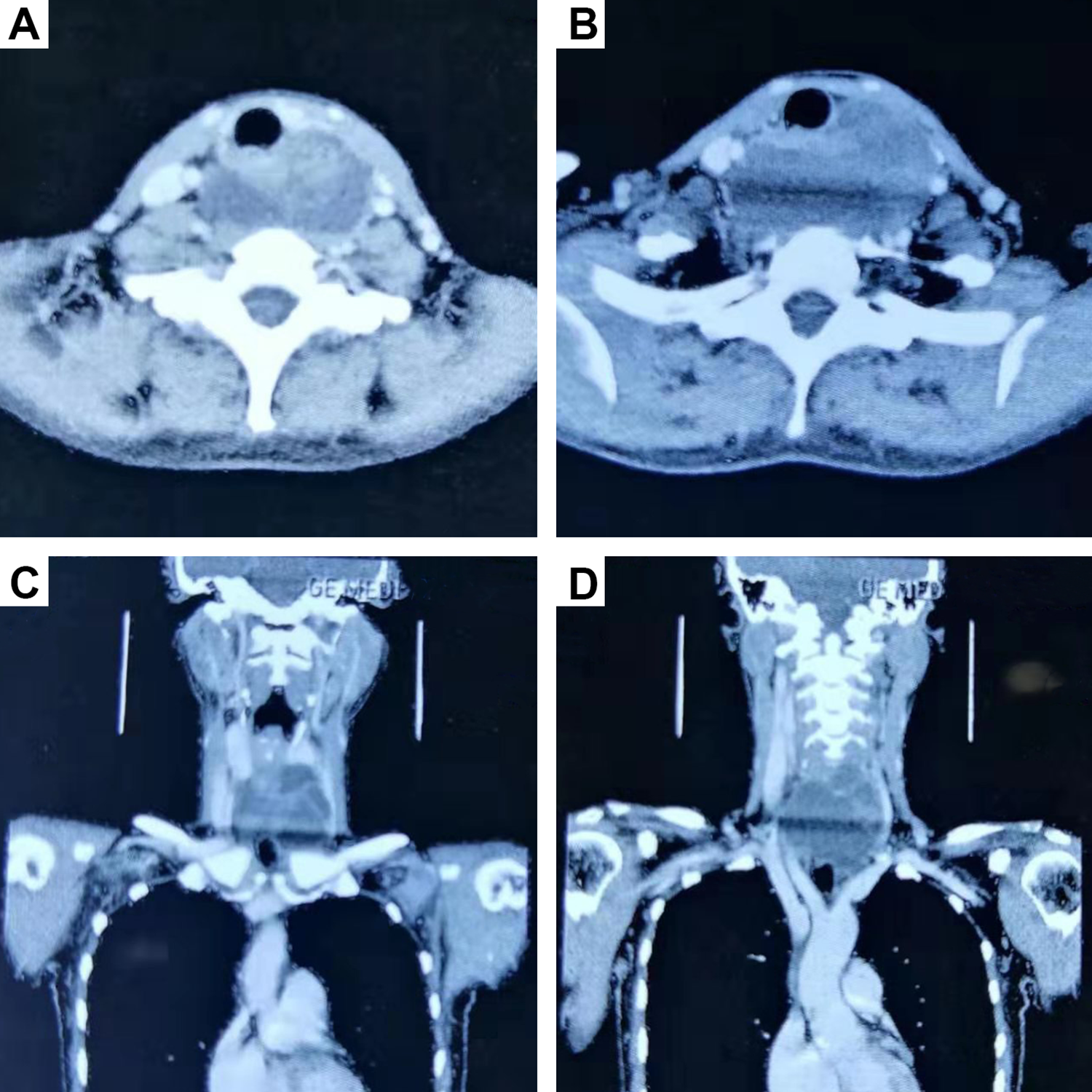
Axial (A, B) and coronal (C, D) computed-tomography (CT) showed a well-defined, cystic-solid, heterogeneous cervical mass extending into the upper mediastinum, which caused trachea and esophagus deviation.
The patient underwent cervical discectomy surgery. During the operation, a cystic mass was found between the sternocleidomastoid muscle and strap muscle. The trachea and esophagus were displaced to the right. There was no sign of infiltration of any of the surrounding tissues (eg, trachea, thyroid gland, carotid sheath) except the esophagus. There was a close relationship between the tumor and the thickened wall of the cervical esophagus (at the level of rings 3-6 of the trachea). The intraoperative frozen section showed a small round cell tumor. The tumor was subsequently excised from the outer membrane of the cervical esophagus. Gross findings showed a mass measuring 9 × 8 × 6 cm in size with a thinned cyst wall full of fluid hematoma. The patient appeared well after the operation with no esophageal fistula.
Final pathology of the mass confirmed that it was a round cell malignant tumor with a specific immunophenotype: strongly positive for cluster of differentiation 99 (CD99), friend leukemia virus integration 1 (FLI-1), neuron-specific endolase (NSE), and ERG; weakly positive for S100 and Ki-67; and negative for leukocyte common antigen (LCA), synaptophsin, chromogranin A, human melanoma black-45 (HMB45), and other hematopoietic markers, which suggested EES (Figure 3). Testing for the EWSR1 gene rearrangement on chromosome t (11; 22) (q24; q12) via fluorescence in situ hybridization was positive and confirmed the diagnosis of EES (Figure 4).
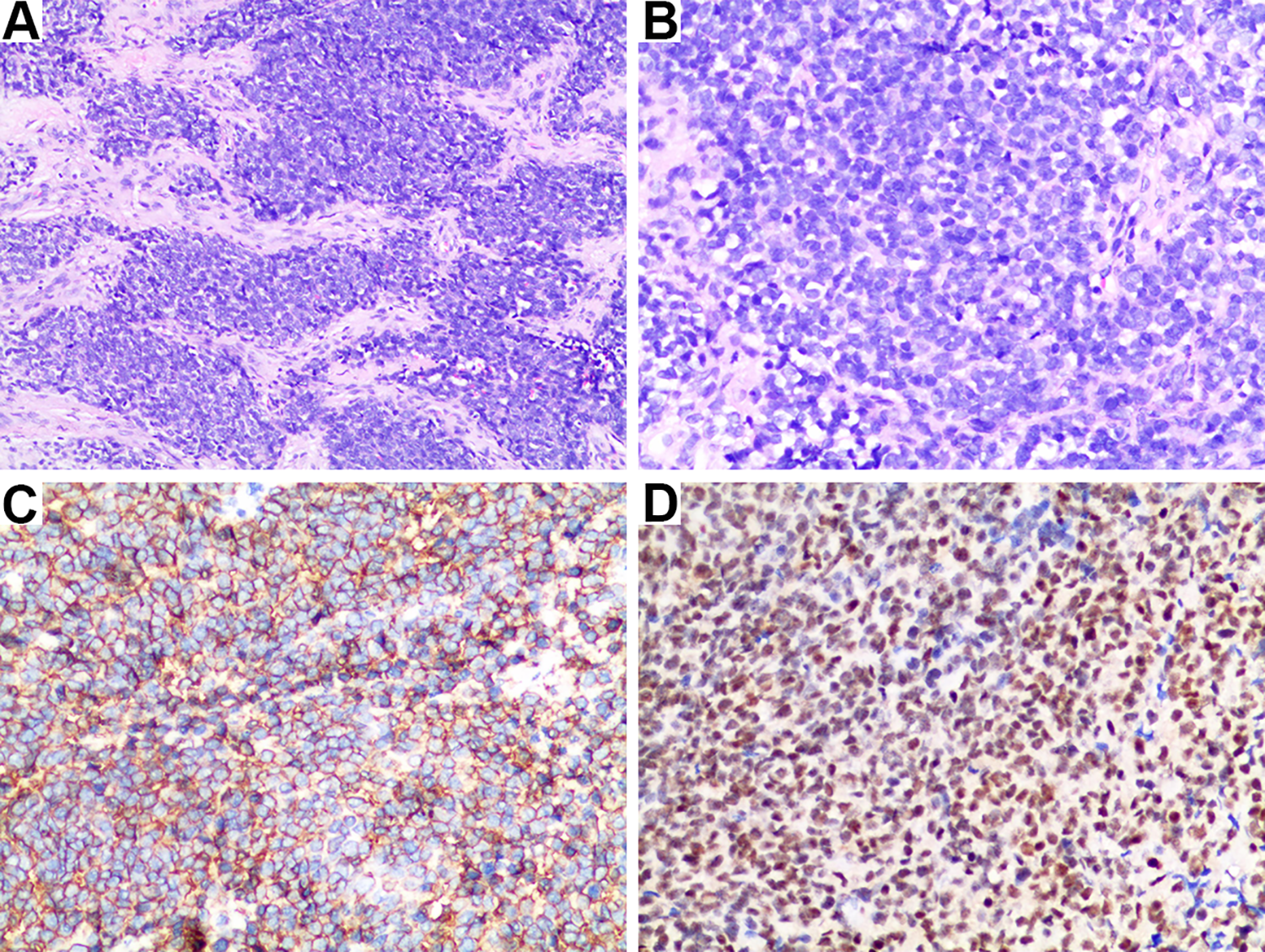
The pathological results of extraosseous Ewing sarcoma of cervical esophagus. A and B, Hematoxylin and eosin stain showed a uniform population of small round blue cells. C, Immunohistochemistry of CD99 showed diffuse strong membrane staining. D, Immunohistochemistry of FLI-1 showed diffuse strong cytoplasm staining. (Original magnification a ×10, B-D ×20).
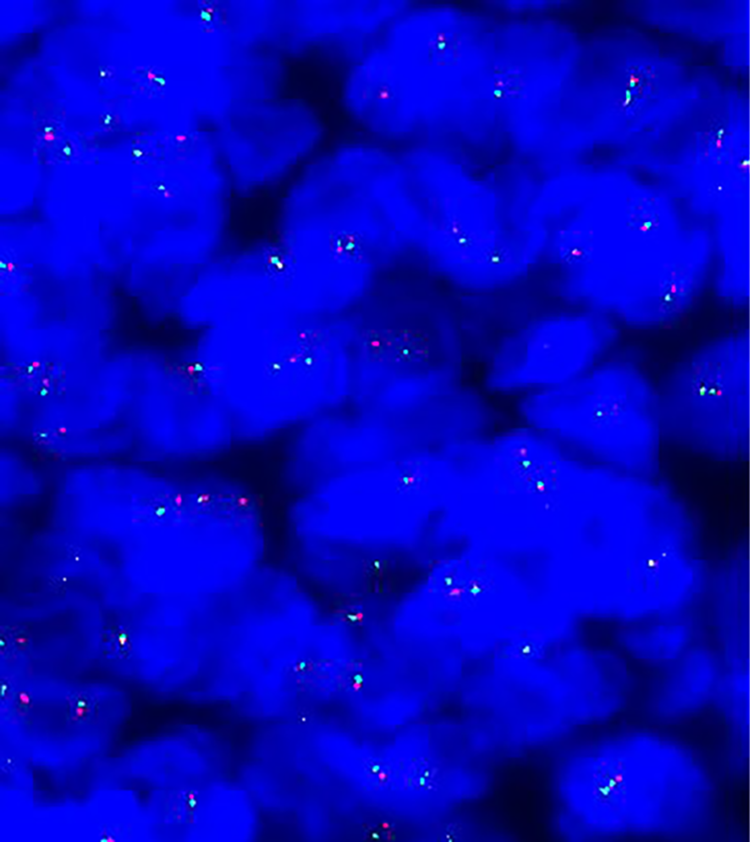
Fluorescence in situ hybridization by dual-color break apart probe 22q12 illustrating the EWSR1 gene rearrangement. The targeted area showed 28.2% of the cells with the translocation pattern.
One month after surgery, positron emission tomography-CT examination was performed, and showed intense hypermetabolic activity (SUVmax 9.0) in the cervical esophagus, with no evidence of cervical lymphadenopathy or distant metastasis (Figure 5). Subsequently, the patient was administered chemotherapy with vincristine, doxorubicin, cyclophosphamide, alternated with ifosfamide and etoposide (3-week intervals between cycles). Local radiation therapy of the neck was performed after 7 cycles of chemotherapy. As of the writing of this manuscript, it has been 19 months since the surgery, and recent follow-up magnetic resonance imaging of the neck did not reveal any evidence of tumor recurrence or metastasis.
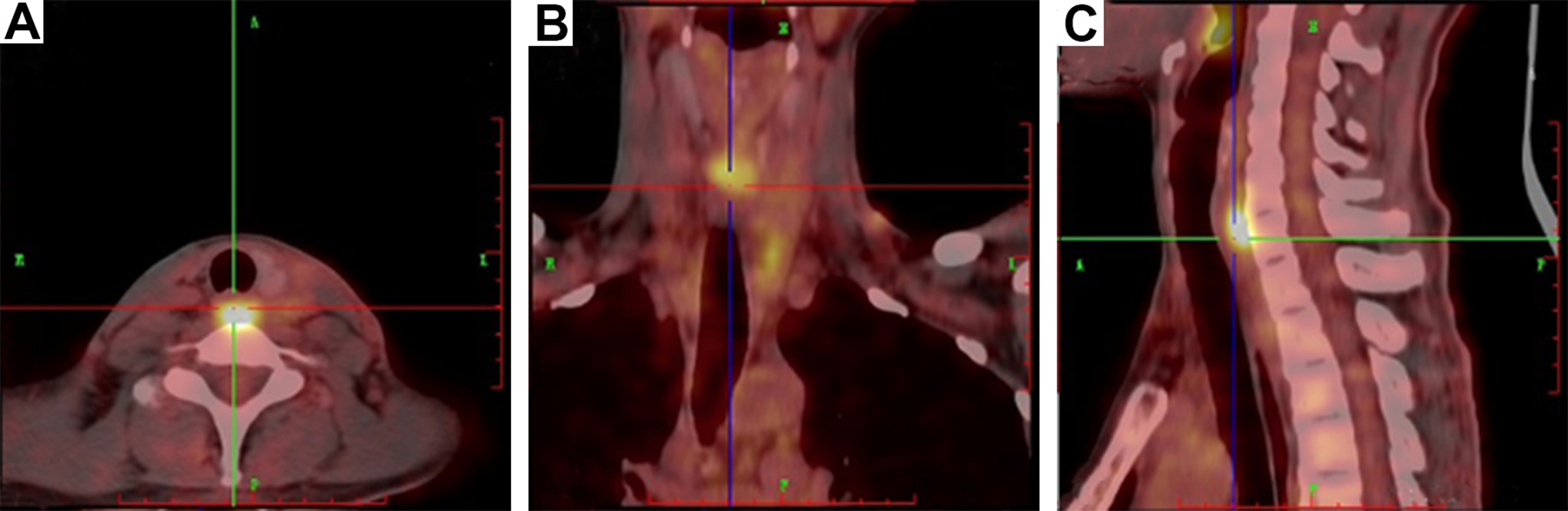
The postoperative PET-CT revealed intense hypermetabolic activity in the cervical esophagus. (A) axial view (B) coronal view (C) sagittal view. CT indicates computed-tomography; PET, positron emission tomography.
This case report was approved by the Research Ethics Committee of Central South University, Changsha, China. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Discussion
Extraosseous Ewing sarcoma belongs to the Ewing family of tumors, which was first described by Tefft et al in 1969. 4 Extraosseous Ewing sarcoma shows aggressive clinical features with a high rate of recurrence and a high mortality rate. Until now, only 2 cases of EES involving the thoracic esophagus have been reported.1,3 However, to the best of our knowledge, there is no report about EES in the cervical esophagus. Here, we report a new type of cervical esophageal small round cell tumors.
Extraosseous Ewing sarcoma usually has no specific clinical manifestation. The most common presenting symptom is a rapidly growing mass with or without local pain. 5 With regard to the esophageal EES, all patients have dysphagia.1,3 In our case, the examinations showed that the neoplasm had exophytic growth without involvement of the mucosal layers of the cervical esophagus. Hence, our patient had slight dysphagia with a cervical mass as the main symptom, making her case differ from thoracic esophageal EES. The imaging characteristics of soft tissue EES are nonspecific as well. It often presents as a well-defined mass that may be mistaken for a benign lesion. 6 According to the adjuvant examinations, we did not consider esophageal EES for the differential diagnosis before the operation, and thought that it might be a cystic mass such as lymphangioma or a branchial cyst. As shown in our patient, intratumor necrosis and hematoma of EES usually appear as hypodense foci in the CT scan. However, the relationship between the cervical esophagus and tumor was confirmed through surgery rather than the ultrasound or CT in our case.
The diagnosis of Ewing sarcoma is based on immunohistochemistry and molecular genetic assays. 7 It is necessary to conduct examinations by using multiple immunohistochemical markers when small round cell tumors of the esophagus are found. CD99 is a reliable marker of Ewing sarcoma during the differential diagnosis of small round cell tumors. 8 It is generally believed that CD99 and FLI-1 markers have high sensitivity but lack specificity for EES diagnosis. 9 For this reason, molecular genetic characterization of chromosomal translocations is necessary to establish a definitive diagnosis of EES. The presence of a t (11; 22) (q24; q12) translocation is found in 88% to 95% of Ewing sarcoma cases.10,11 When the presence of the t (11; 22) (q24; q12) is combined with positive staining for CD99, the diagnostic accuracy of EES can approach 100%.12,13 We reviewed the literature on esophageal EES, the immunohistochemistry results and molecular genetic analysis are shown in Table 1.
Immunohistochemistry and Molecular Markers for Esophageal Extraosseous Ewing Sarcoma.
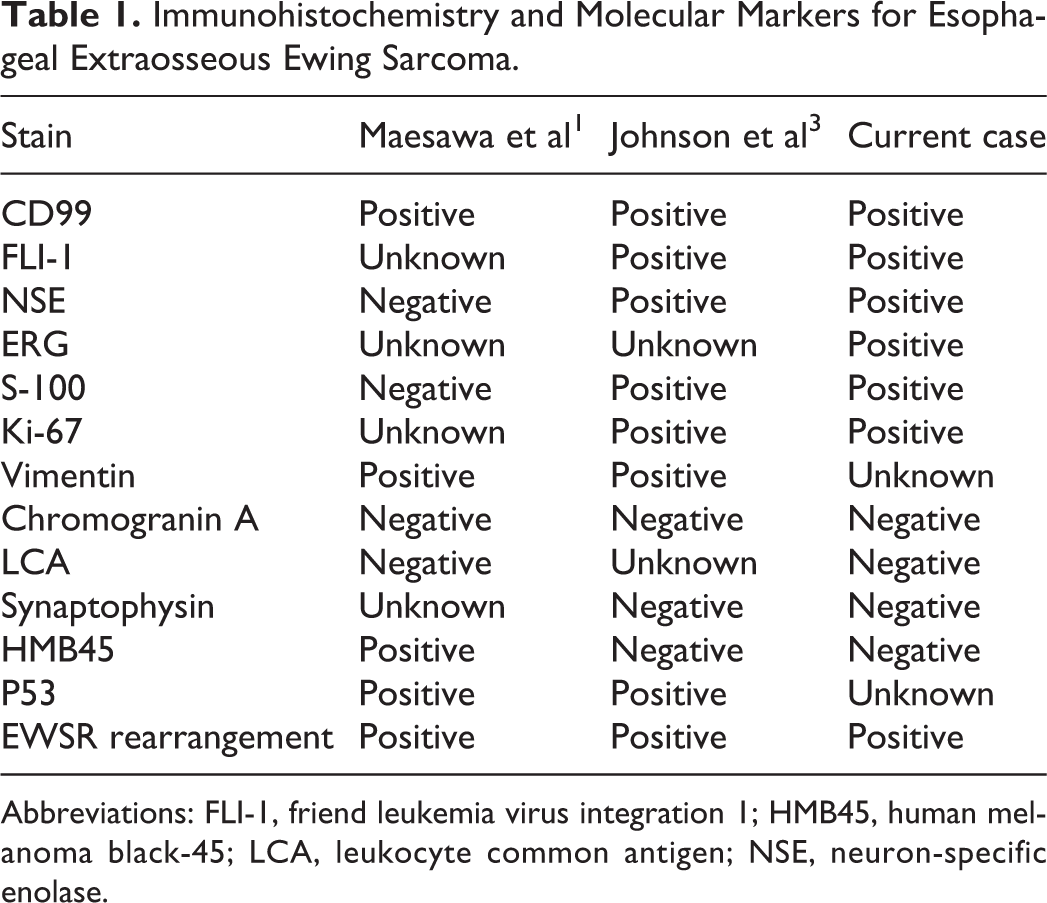
Abbreviations: FLI-1, friend leukemia virus integration 1; HMB45, human melanoma black-45; LCA, leukocyte common antigen; NSE, neuron-specific enolase.
With regard to treatment of esophageal EES, 2 prerequisites are needed: it must be an Ewing sarcoma, and the esophagus must be the site of the primary lesion and not a metastatic focus. Positron emission tomography-CT is a valuable method of excluding metastases. 14 Notably, the recommendations put forward by the National Comprehensive Cancer Network make no stipulation for the treatment of EES and skeletal Ewing sarcoma. 15 A local surgical therapy in combination with radiotherapy and chemotherapy (vincristine, doxorubicin, cyclophosphamide, ifosfamide, and etoposide) has been considered to be a superior regimen for localized EES at any site. 16 Among the 2 patients with thoracic esophageal EES, 1 patient, reported by Maesawa et al 1 , was treated with esophagectomy and postoperative immunochemotherapy, but died of disease relapse 18 months after surgery; and the other patient, reported by Johnson et al 3 , only received chemotherapy because of her colon adenocarcinoma. It is generally accepted that the surgical approach to cervical esophageal tumors is completely different from that suitable for thoracic esophageal tumors. Tumors of the cervical esophagus usually require extensive en bloc resection that includes the hypopharynx, esophagus, cervical lymph nodes, and larynx, as well as a permanent tracheostomy in many cases. 17 In our case, the accurate diagnosis could not be derived from the intraoperative frozen section evaluation. Hence, we did not perform extended esophagectomy considering the depth of tumor infiltration and prospects for a better future quality of life. As of the writing of this manuscript, the patient has been doing well after chemotherapy and radiotherapy with no evidence of tumor recurrence or metastasis.
In conclusion, we describe our experience regarding the clinical characteristics, diagnosis, treatment method, and prognosis of cervical esophageal Ewing sarcoma. The case increases the differential diagnosis of small round cell tumors in cervical esophagus. In addition, we do not recommend radical esophagectomy for localized EES of the cervical esophagus. Postoperative chemotherapy and radiotherapy are of great value in improving the prognosis of EES.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.