
Abstract
Coins are among the most common foreign bodies ingested by children, especially those below 5 years of age. Early endoscopic retrieval of esophageal coins minimizes the risk of serious complications. However, significant morbidity and mortality are reported when coins are retained in the gastrointestinal tract for prolonged periods of time. We report a case in which a coin was retained in the upper esophagus for 4 years and presented a distinctive clinical course. An esophageal coin retained for a prolonged period may place the patient at a risk of complications such as tracheoesophageal fistulas. The management of patients with complicated aerodigestive tract foreign bodies is challenging. To avoid a delayed diagnosis and to improve the patients’ safety, the quality of medical care in rural areas should be monitored by implementing continuous educational programs for primary physicians.
Introduction
Ingested foreign bodies are commonly observed in the upper esophagus of children. 1 Although airway aspiration of foreign bodies is dangerous by itself, a delayed diagnosis of foreign bodies in the esophagus can lead to life-threatening complications. 2 Coins are some of the most frequent foreign bodies ingested by children, and most coins remain lodged in the upper esophagus. 1 Children with foreign bodies in the upper esophagus can present with various airway and gastrointestinal symptoms, and the most common symptoms are pain, odynophagia, dysphagia, and drooling. 3 Most cases of esophageal coin impaction are reported in children between 2 and 5 years of age and children older than 5 years of age have been reported to ingest significantly larger coins. 4
Case presentation
An 11-year-old girl with sickle cell disease and thalassemia was taken to the emergency department by her father after the incidental finding of a foreign body in the upper esophagus by her primary physician who reviewed her routine chest radiograph 3 weeks previously and advised the patient to visit a tertiary hospital. The child revealed that she ingested the coin several years ago while playing with a peer, which was followed by an episode of vomiting. However, she had not informed her parents about this incident. She denied having any subsequent history of drooling of saliva, stridor, or dysphagia and was completely asymptomatic. Her father reported that in the two years prior to our hospital visit, she had multiple local hospital visits because of vaso-occlusive crises. During these visits, she had undergone multiple chest radiography tests, which revealed a round radio-opaque object that was considered to be an artifact from a necklace or clothes by the physicians. The father also presented the oldest chest radiograph, which was acquired more than 4 years ago (Figure 1). The oldest chest radiograph of the patient was acquired 4 years ago by the local hospital prior to our hospital visit.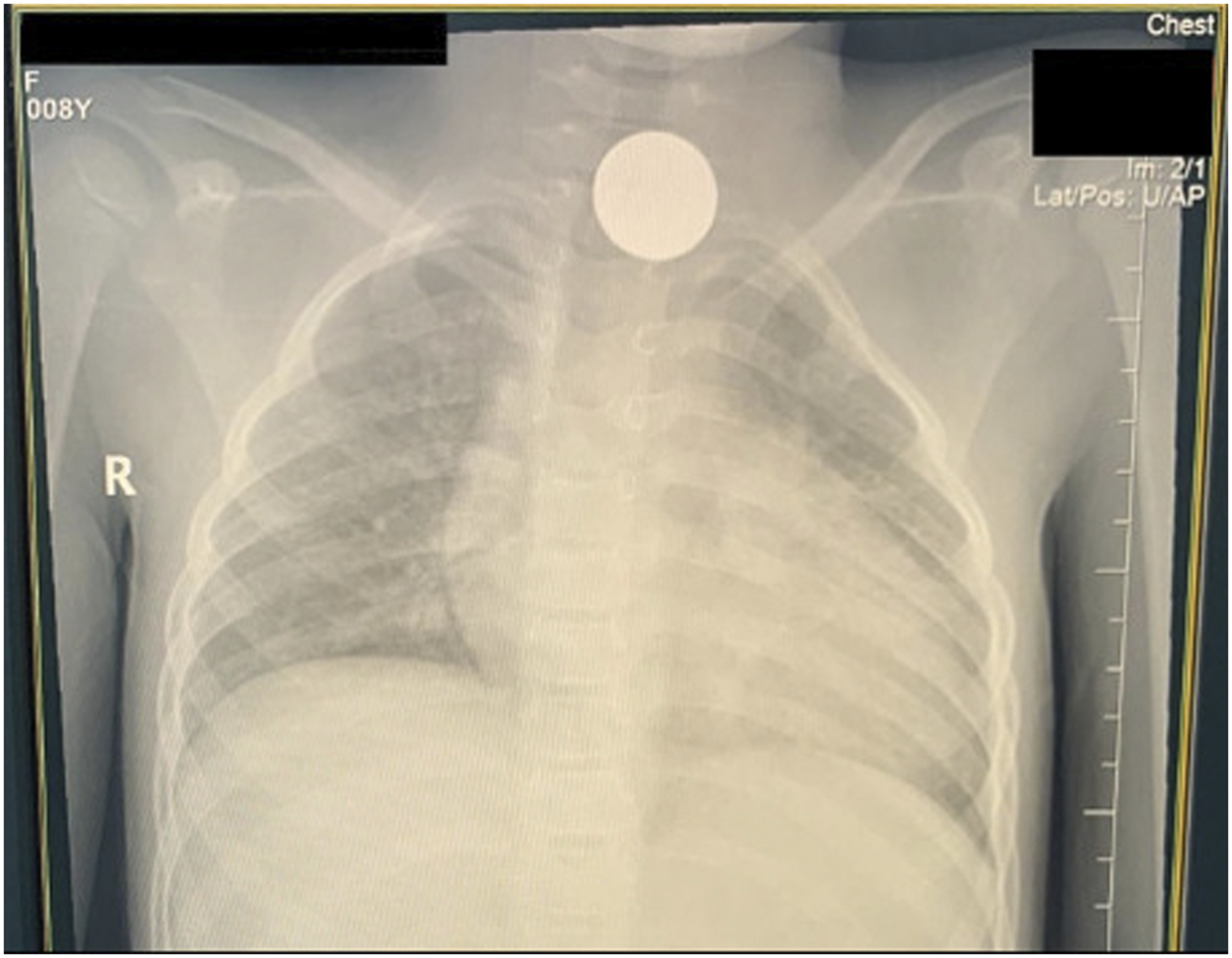
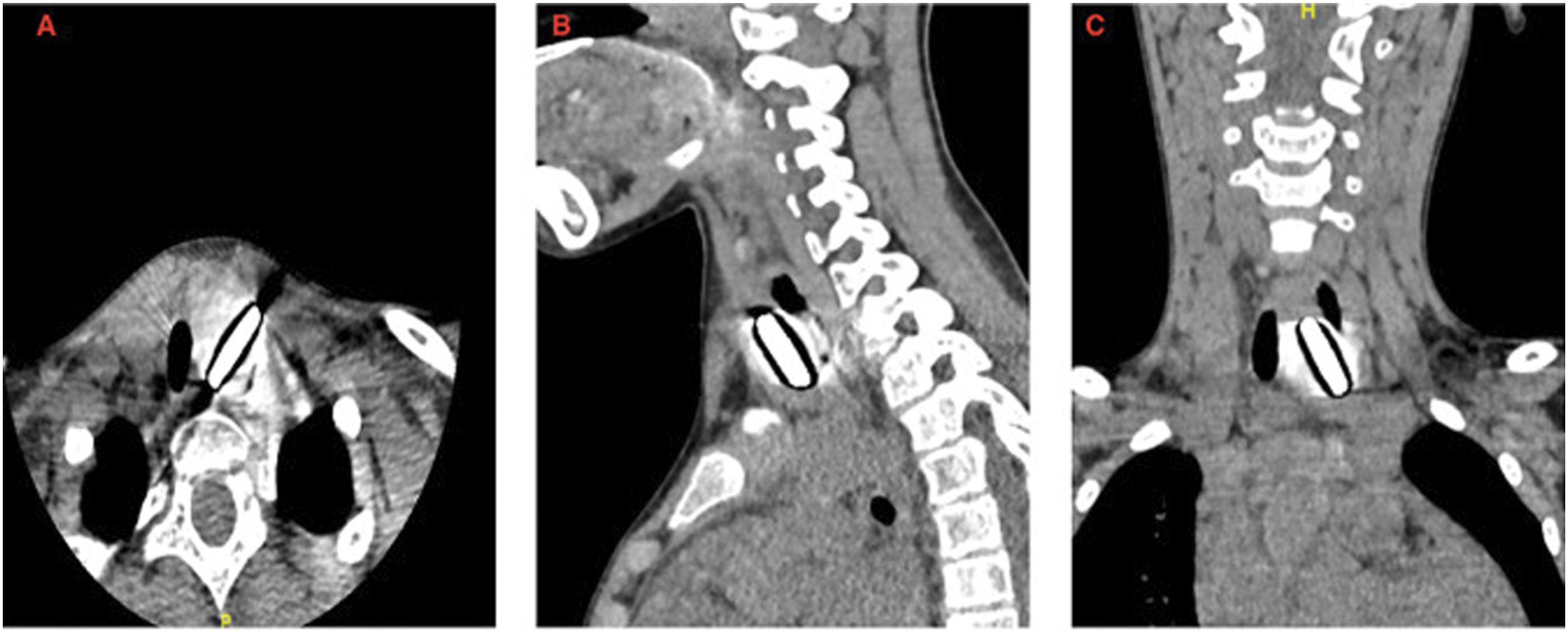
On physical examination, the patient was vitally stable and without distress; her body weight was 21 kg less than the 3rd percentile of the growth chart. Additionally, she showed a tracheal shift to the right without a tracheal tug or chest retraction, and her throat was clear. Transnasal flexible laryngoscopy revealed adenoid hypertrophy (grade 2), normal-looking larynx with bilaterally mobile vocal cords and no foreign bodies. Another chest radiography was performed, which revealed a radio-opaque foreign body in the left supraclavicular area as well as displacement of the trachea to the right (Figure 2). Owing to the chronicity of her condition, a vague history, and tracheal deviation on the radiograph, we decided to perform computed tomography (CT). CT revealed a round radio-opaque foreign body in the superior mediastinum, extraluminal of the esophagus with intact major vessels (Figure 3). A water-soluble contrast swallow was then performed revealing that the foreign body likely migrated through the wall of the esophagus as the contrast passed through smoothly with no filling defects or evidence of a diverticulum. Plain chest radiographs of the patient were acquired upon arrival at the emergency department. Computed tomography reveals a radio-opaque foreign body at the C6 vertebral level; (A) axial view; (B) sagittal view; (C) coronal view.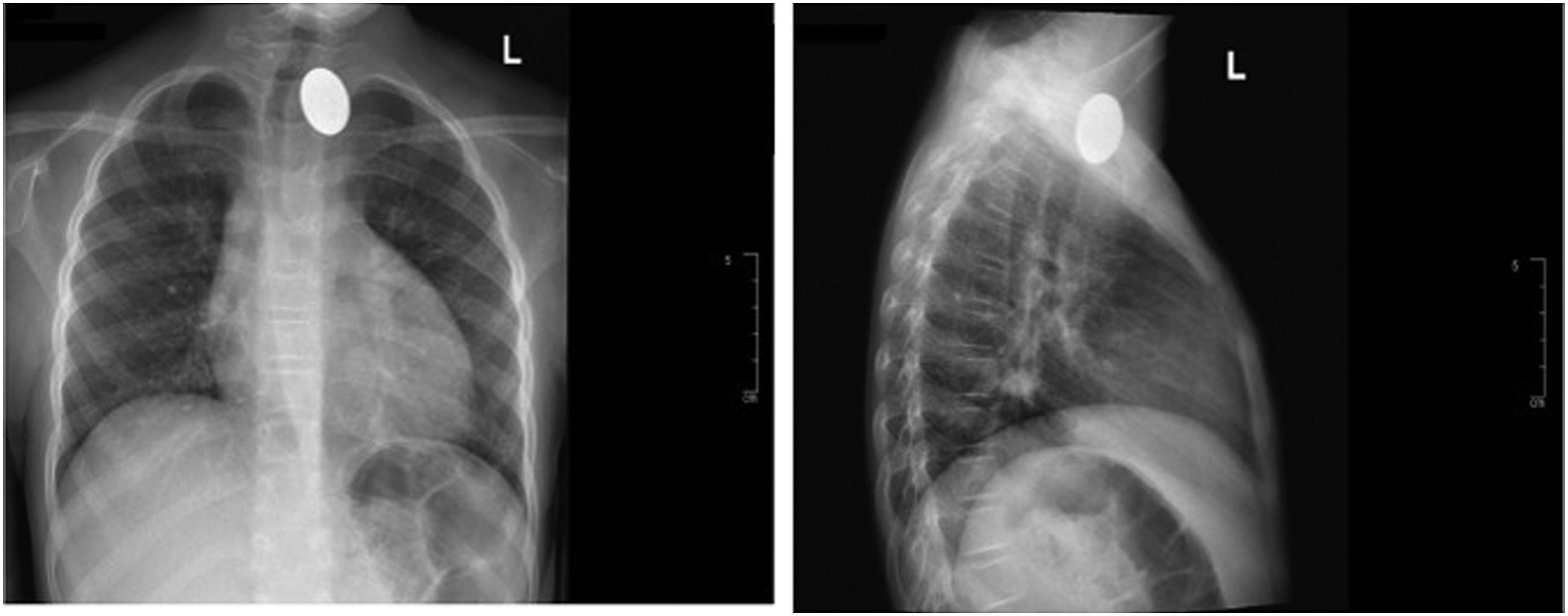
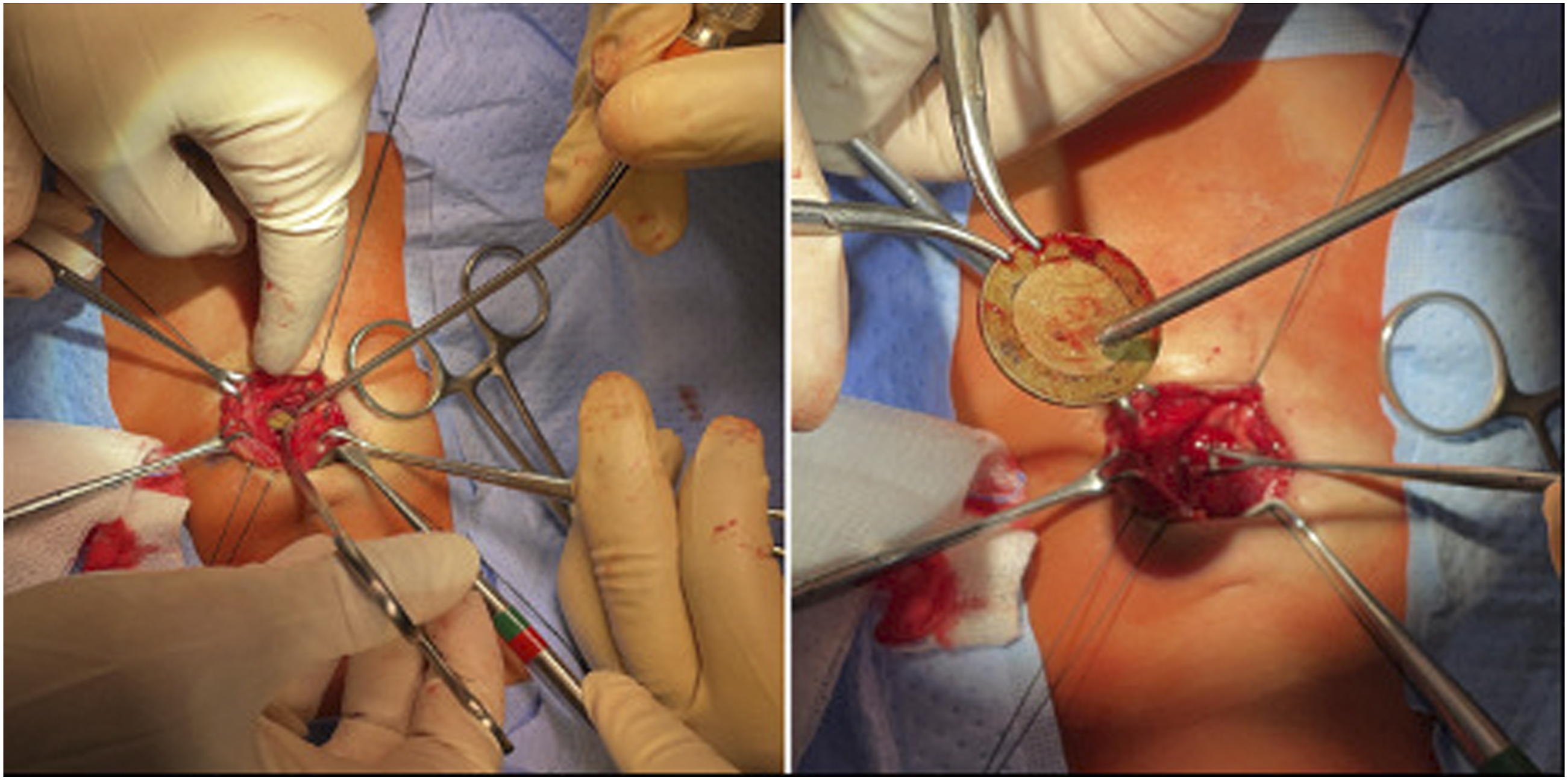
The patient was taken to the operating room. First, a bronchoscopy was performed, which was noted to be normal with no external compression or evidence of tracheoesophageal fistula. Next, a flexible esophagoscopy revealed the foreign body had migrated through the esophageal wall with only a slight indentation into the lumen of the esophagus and intact overlying esophageal mucosa (Figure 4). It was not amenable to endoscopic removal. We proceeded with a neck exploration through a collar incision. The surgical field was noted to be fibrosed, which distorted the anatomy. The tracheoesophageal groove was identified, and the coin was retrieved with meticulous dissection (Figure 5). Intra-operatively, a nerve stimulator was used to check for the recurrent laryngeal nerve, and signals were observed. Finally, a repeated esophagoscopy was performed at the end of the operation, and a leak test showed no evidence of a leak. Intra-operative flexible esophagoscopy showing slight indentation over the wall of the esophagus. Foreign body removal using transverse neck incision.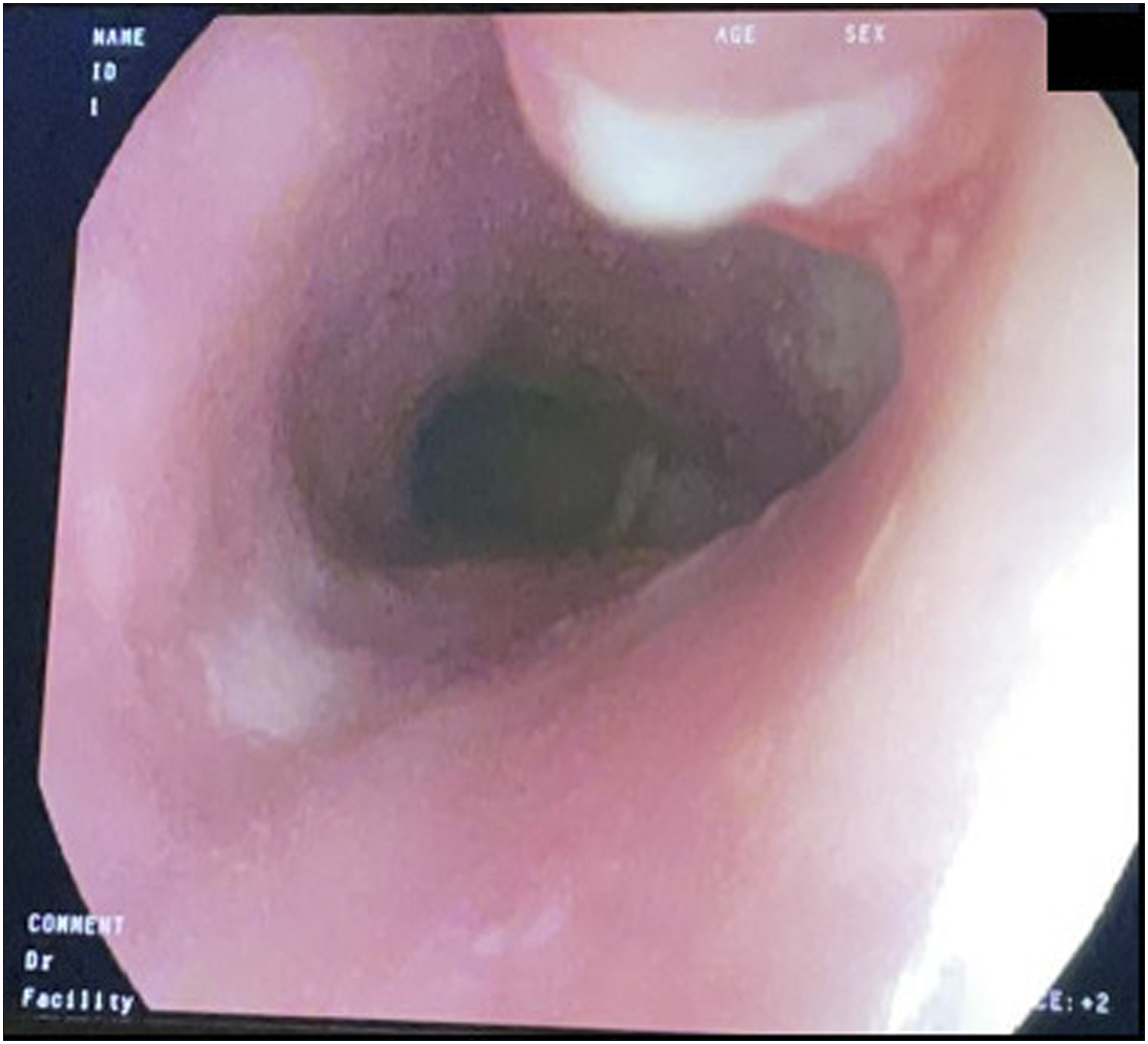
Postoperatively, the patient was kept NPO, and a contrast swallow was performed on postoperative day 3; it revealed no signs of leaks or strictures. The patient was started on a clear liquid diet, advanced to a regular diet without issues, and was finally discharged 4 days postoperatively with instructions and an outpatient follow-up appointment. On postoperative day 10, she presented to the hospital owing to fluid leakage through the surgical wound that increased with oral intake. A CT scan of the neck was performed, and it revealed air tracking from the esophagus to the skin, suggestive of a fistula. She was admitted to the hospital again and kept NPO. She was administered broad-spectrum antibiotics and total parenteral nutrition. A contrast swallow was conducted 10 days later, revealing a small sinus tract arising from the anterior aspect of the lower cervical esophagus (Figure 6). At the time of the study, a nasogastric tube (NGT) was placed under fluoroscopy guidance, and enteral feeding was subsequently started and tolerated well by the patient. She was discharged on NGT feeds and an outpatient appointment to repeat the contrast swallow in 1 week. The repeated contrast study showed improvement of the previously noted outpouching arising from the anterior aspect of the lower cervical/upper thoracic esophagus. Another contrast study 2 weeks later revealed complete resolution of the leak and outpouching. The NGT was removed, and the patient resumed oral feeding without issue. She was seen in the outpatient clinic 3 months postoperatively and was tolerating oral feeding well and gaining weight with no active complaints. X-ray fluoroscopic upper gastrointestinal Gastrografin study reveals the sinus tract with irregularity in the anterior surface of the upper esophagus at the C6 vertebral level.
Discussion
Foreign body ingestion is a common problem among children aged 5 months to 8 years, with a peak incidence between the first and third years of life. 5 If the clinical history is unclear, the diagnosis may be delayed because up to 50% of patients have atypical or no symptoms. 6 Complications of retained foreign bodies depend on their location, type, and duration of retention. 7 A high relative risk (6.83%) of complications was reported among 161 children who underwent endoscopic or surgical removal of foreign bodies in the esophagus and gastrointestinal tract after 72 h of ingestion. 8 Life-threatening complications of a delayed diagnosis include esophageal perforation, esophageal ulcer, peri-esophagitis, esophageal stenosis, tracheoesophageal fistula, mediastinitis, pneumothorax, pyothorax, unilateral vocal fold paralysis, and tracheal stenosis.9,10 The common signs and symptoms of esophageal foreign bodies retained for less than 24 h are pain, odynophagia, dysphagia, drooling of saliva, vomiting, gagging, anorexia, choking, and cyanosis.3,11 However, respiratory symptoms, such as cough, shortness of breath, stridor, upper respiratory tract infection, and pneumonia, are more consistent with the late (weeks to months) presentation of foreign body ingestion.
The most important factors resulting in a delayed diagnosis of foreign body ingestion among children are unwitnessed ingestion or asymptomatic patients and the presence of radiolucent objects on radiographs.12-15 CT, ultrasonography, and magnetic resonance imaging may be indicated in such patients with questionable foreign body ingestion. 16
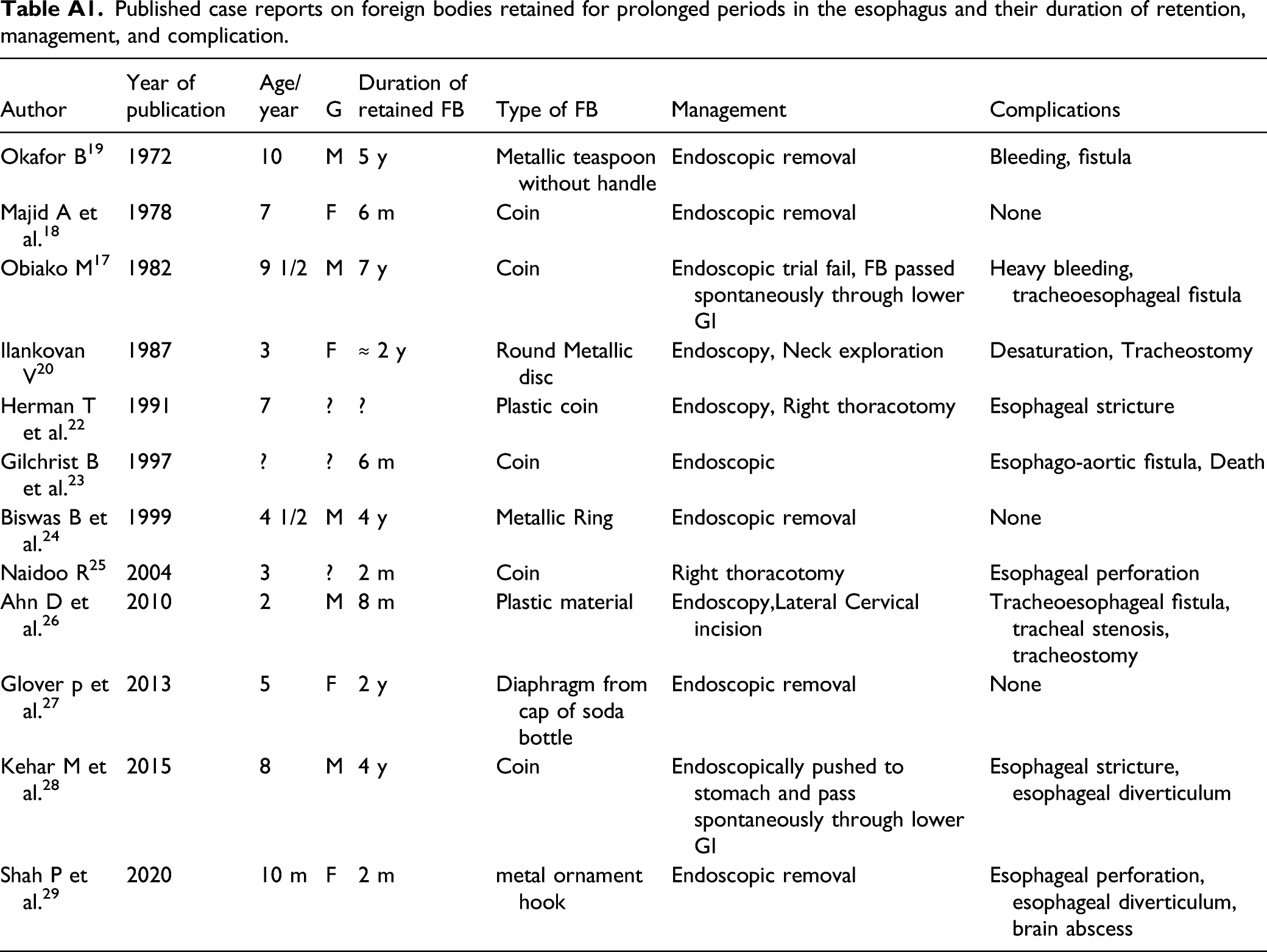
Published case reports on foreign bodies retained for prolonged periods in the esophagus and their duration of retention, management, and complication.
In our case, the patient was asymptomatic for 4 years, had an unwitnessed ingestion, and the foreign body was incidentally found during routine chest radiography performed during the hematologic follow-up for sickle cell disease and thalassemia. However, the foreign body was a radio-opaque coin that had been observed on multiple anteroposterior (AP) view radiographs, but it had been misinterpreted by the primary physician. Although the patient’s father had concerns regarding the radiographic finding and had inquired about it multiple times, he was reassured by physicians that it was an artifact. A similar history of misinterpretation of radio-opaque objects was reported in 1987 by Ilankovan. 20 These findings highlight the importance of acquiring AP and lateral view radiographs and addressing the concerns of the patients and their family, especially because 50% of patients with upper esophageal foreign bodies are asymptomatic. 6 The American Society for Gastrointestinal Endoscopy (ASGE) advocates the use of radiography (both AP and lateral views) as the initial diagnostic tool for patients with suspected foreign body ingestion. Furthermore, when the presentation is equivocal or if radiography is non-diagnostic, the ASGE suggests CT with three-dimensional reconstruction as the subsequent diagnostic procedure. 21
Conclusions
An esophageal coin retained for a prolonged period may place the patient at a risk of complications such as tracheoesophageal fistulas. The management of patients with complicated aerodigestive tract foreign bodies is challenging. To avoid a delayed diagnosis and to improve the patients’ safety, the quality of medical care in rural areas should be monitored by implementing continuous educational programs for primary physicians.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.