
Abstract

Multiple central giant cell granulomas of the jaws may be associated with systemic conditions such as hyperparathyroidism, cherubism, Noonan-like syndrome, Ramon syndrome, and Jaffe–Campanacci syndrome.1,2 If clinical examination and laboratory tests do not suggest the diagnosis of hyperparathyroidism or an inherited syndrome, then most children with multiple symmetrical giant cell granulomas represent a form of cherubism. However, there have been rare reports of multiple synchronous giant cell granulomas for which other causes have been excluded.3,4 There is a familial tendency to multiple lesions of this nature in some cases. 5
Giant cell granuloma of the jaws tends to occur in younger patients, most frequently before the age of 20 years, and it affects twice as many females as males. The lesion may arise in any area of the jaws but is seen more often where there are or have been deciduous teeth (ie, anterior to the first permanent molars).
The radiographic appearance of giant cell granuloma depends on the size of the lesion (Figure 1). Smaller lesions are unilocular (totally radiolucent), and larger lesions have a faint granular pattern of internal calcifications. 6 In some lesions of the later type, there is one or more ill-defined wispy septa. Occasionally, the septa are rather substantial and coarse which divide the internal structure into a multilocular “soap bubble” appearance. The lesion usually has a well-defined cortical border, although it may have ill-defined margins, raising the possibility of a malignant condition. 7 Some giant cell granulomas have markedly undulating margins. If present, coupled with some wispy internal septa, this is suggestive of the lesion. Often there is rather marked expansion of the adjacent cortical plates. Enlarging lesions are capable of causing bone destruction, occasionally with extension into the surrounding soft tissues. 6 Tooth displacement and resorption are common. 8
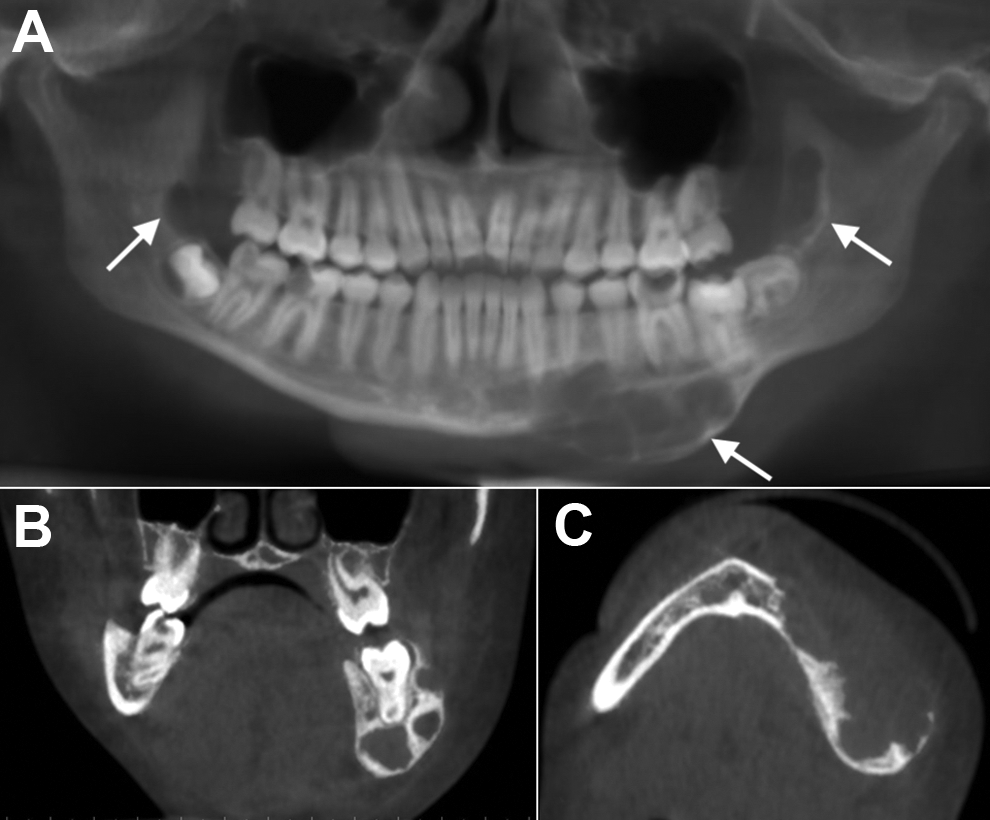
Multiple giant cell granulomas of the jaw in an otherwise healthy 14-year-old girl. A, Reformatted panoramic cone-beam computed tomography (CBCT) image shows 3 giant cell lesions throughout the mandible (arrows). B, Coronal CBCT image shows a multilocular lesion in the body of the left mandible. Note the thick, curved septa. C, Axial CBCT image demonstrate significant expansion of the mandibular body as well as destruction of the buccal cortex; also note the crenations causing scalloping of the endosteal surface.
Giant cell granulomas of the jaws are usually treated by enucleation and curettage, sometimes supplemented with local osteotomy, although some aggressive and recurrent lesions require more radical surgery. Recurrence rates range from 13% to 49%. 8
Footnotes
Authors’ Note
This study is not previously presented or published.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.