
Abstract
Objective:
To evaluate the effect of the supraclavicular artery island flap (SAIF) in reconstructing pharyngocutaneous fistula in patients with laryngopharyngeal cancer with prior radiotherapy.
Methods:
Six patients with laryngopharyngeal cancer with pharyngocutaneous fistula due to previous radiotherapy and surgery during 2016 to 2019 were retrospectively analyzed. Initially, the fistula was treated conservatively. The SAIF was applied with double folding technique to reconstruct fistula in the patients who failed to heal after conservative treatment.
Results:
The fistulae closed in 4 patients after conservative treatment. After SAIF operation, fistula closure was achieved in the other 2 patients who received highest dose of radiation and had largest fistulae size. The flaps grew well and there were no donor-site complications in these 2 patients. All patients achieved oral feeding without any complications.
Conclusion:
The SAIF is an effective and safe approach to reconstruct the pharyngocutaneous fistula after laryngopharyngeal surgery in patients with laryngopharyngeal cancer with previous radiotherapy, especially for those who have received high-dose radiation and have large fistula.
Keywords
Introduction
Pharyngocutaneous fistula is a troublesome complication after surgical treatment of laryngeal and laryngopharyngeal cancer, especially in patients who have undergone prior radiotherapy. 1 Pharyngocutaneous fistula is the defect of skin and soft tissue in the anterior cervical region, and severely decreases patients’ quality of life. There are many risk factors for pharyngocutaneous fistula, including preoperative radiotherapy, chemotherapy, malnutrition, tumor site and stage, and surgical range. 2 Of these factors, radiotherapy plays a significant role in the development of pharyngocutaneous fistula. Redaelli et al 3 reported the incidence of pharyngocutaneous fistula after radiotherapy was 60%. Comparing to patients without radiotherapy, patients who received conventional radiotherapy were twice more likely to develop pharyngocutaneous fistula, and patients who received high-dose radiotherapy were 4 times likely to develop pharyngocutaneous fistula. 3
Pharyngocutaneous fistula after radiotherapy is difficult to heal by conventional conservative treatment. Therefore, an ideal surgical strategy, which can effectively close pharyngocutaneous fistula and definitely reconstruct the anterior cervical skin and soft tissue defects, is urgently needed. In recent years, the supraclavicular artery island flap (SAIF) has shown promising results in head and neck reconstruction. Previous studies have reported that SAIF was safe for patients who have received radiotherapy on the neck.4,5 Here, we report successful treatment of pharyngocutaneous fistula with SAIF in 2 patients with laryngopharyngeal cancer who received prior radiotherapy and developed fistula after salvage surgery.
Materials and Methods
Patients’ Characteristics
There was a total of 6 patients suffering from pharyngocutaneous fistula between January 2016 and December 2019 in our hospital. Data of these patients were retrospectively analyzed. All patients received radiotherapy before tumor resection and developed pharyngocutaneous fistula after operation. Detailed information of the 6 patients is shown in Table 1. Approval was obtained from the institutional review board of Fujian Medical University Union Hospital prior to the initiation of the study.
Summary of Patient Demographics and Treatment Characteristics.
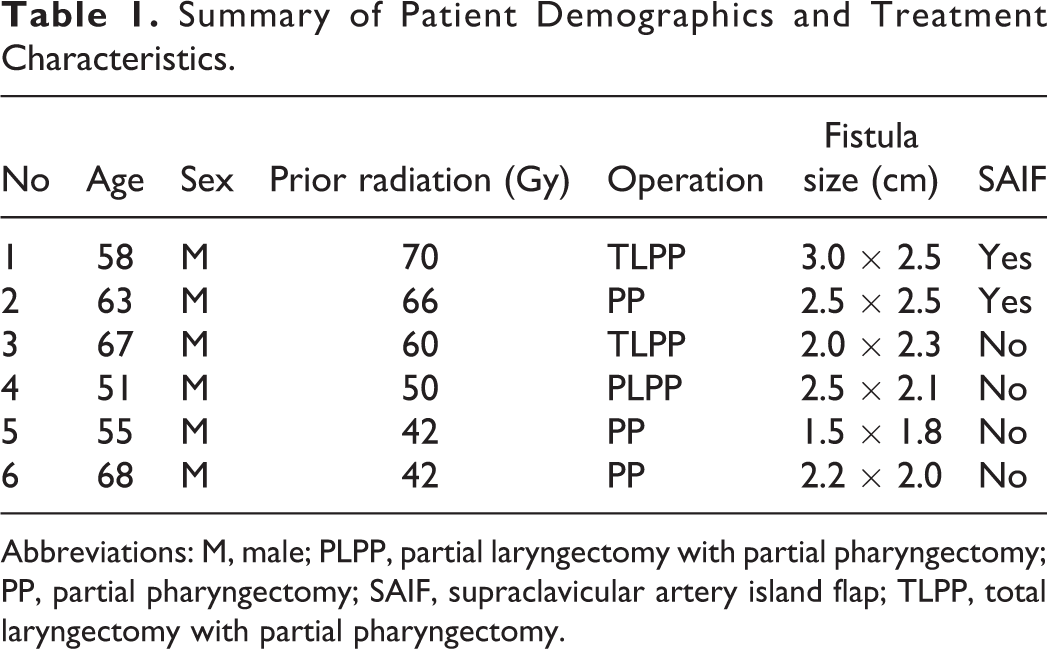
Abbreviations: M, male; PLPP, partial laryngectomy with partial pharyngectomy; PP, partial pharyngectomy; SAIF, supraclavicular artery island flap; TLPP, total laryngectomy with partial pharyngectomy.
Conservative Treatment
Pharyngocutaneous fistula occurred in 7 to 14 days after surgery. Once pharyngocutaneous fistula developed, the external orifice of the fistula was expanded and formed a wound with “funnel” shape. Necrotic tissues were first removed and the wound was cleaned with hydrogen peroxide, iodophor disinfection solution, and normal saline, and packed with the gauze. It was observed that the granulation grew slowly in patients with prior radiotherapy due to decreased local blood supply. After a 4-week conservative management, the necessity of further surgical intervention was evaluated based on the fistula size and the granulation status.
Surgical Intervention
Supraclavicular artery island flap was applied to repair the fistula when the fistula size was not effectively reduced after the 4-week conservative management. Preoperative ultrasonography was performed to locate the transverse cervical artery and the supraclavicular artery. The rotation axis point of the flap was located in 1 cm outside the intersection point of the lateral border of the sternocleidomastoid muscle and the transverse cervical artery. Patients were placed in the supine position with shoulder pads and heads tilted to the opposite side. The flap was designed according to the size of the fistula. Generally, the width was slightly wider than that of the skin defect, and the length was a little bit longer than twice that of the skin defect. Supraclavicular artery island flap was harvested following the methods previously reported. 6 Granulation and nonviable tissue around the skin and the internal fistula were removed to expose the fresh tissue. The proximal end of the flap was sutured to the internal fistula (the skin faced to the deep surface of the fistula), and the flap was folded after the internal fistula was closed. The skin in the folding zone was striped and the folding flap (the distal end of the flap) was sutured to the tissue around the outside surface of the fistula. Pharyngocutaneous fistula closure was completed.
Results
Characteristics of Patients
A total of 6 male patients with laryngeal or laryngopharyngeal cancer (mean age 56.5 years, range 44-68 years) were retrospectively analyzed. Patients’ characteristics are summarized in Table 1. Patients received either laryngectomy or pharyngectomy. All patients had received radiotherapy prior to operation. The sizes of the fistula were also recorded in Table 1.
The Effectiveness of Conservative Treatment
Four of these patients healed after the 4-week conservative treatment. However, the fistula failed to be closed by conservative management in the other 2 cases. They had received the highest dose of radiation and had the largest fistula size.
The Effectiveness of SAIF
Supraclavicular artery island flap was applied for pharyngocutaneous fistula reconstruction in the 2 patients with unclosed fistula after conservative management. The preoperative and intraoperative images of the patients are shown in Figures 1 and 2, respectively. No anastomotic leakage and no vascular crisis or necrosis of the flap was observed in both patients. As shown in Figure 3, fistula closure was achieved. They resumed oral feeding after surgery without complications such as wound infection and functional injury after 23 to 30 days. No recurrence of pharyngeal fistula and hypopharyngeal stricture were observed in both patients in 3 years’ follow-up.

Preoperative image. According to preoperative ultrasonographic Doppler detection, the course of transverse cervical artery and the supraclavicular artery were marked, and the SAIF was designed.
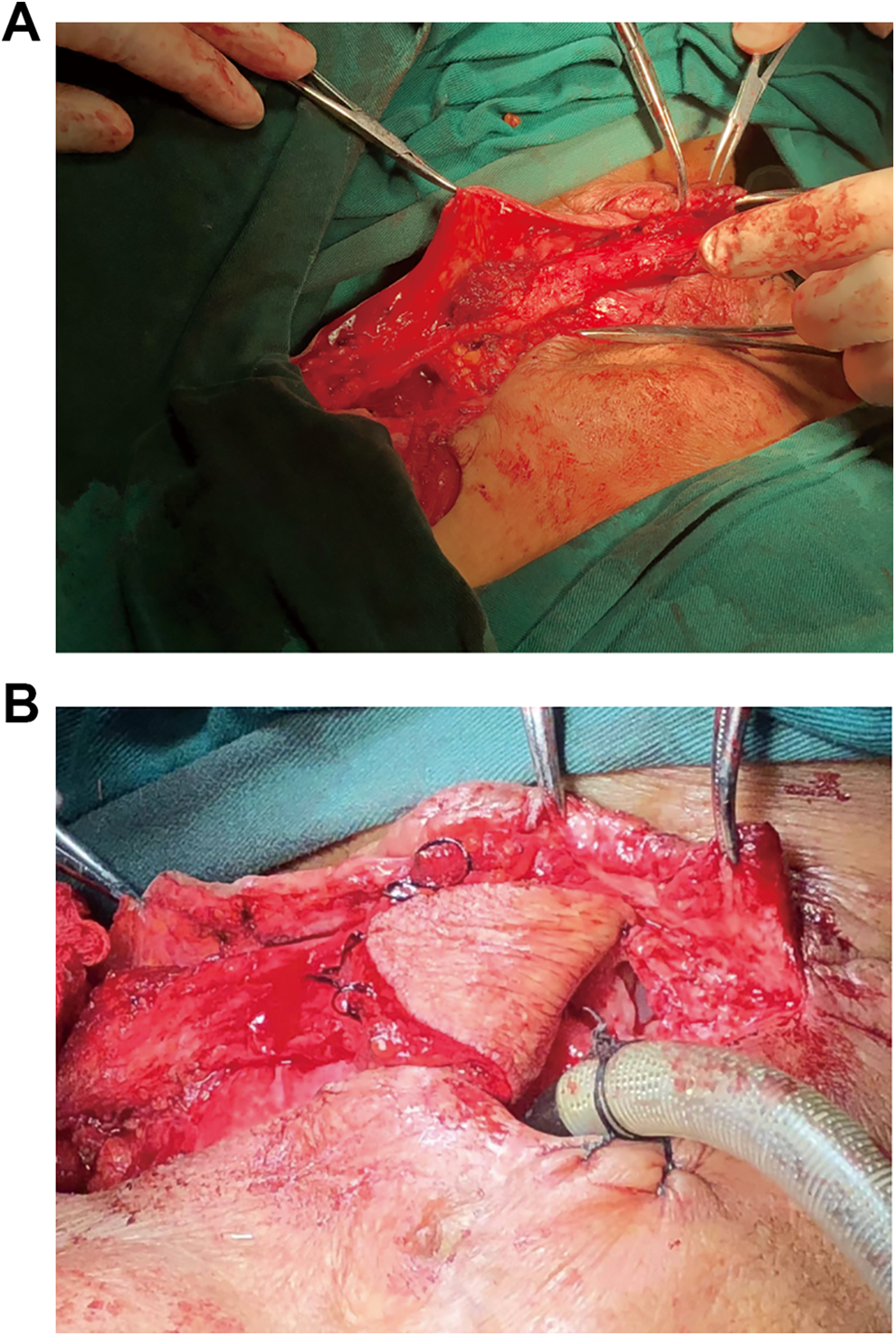
Intraoperative image. A, The flap was lifted from the surface of deltoid muscle, and the vessel fascia pedicle was retained at the proximal end. The flap was dissected to the starting point of the transverse cervical artery. B, Folded flap was made to reconstruct the inner side and surface skin of pharyngocutaneous fistula.

Postoperative image. The pharyngocutaneous fistula was closed.
Discussion
In the present study, we retrospectively analyzed 6 patients with laryngopharyngeal cancer who suffered pharyngocutaneous fistula due to the radiotherapy prior to surgery. The fistula was initially managed conservatively. As a result, 4 of them achieved fistula closure. But the fistula failed to be closed in the other 2 patients who received the highest does of previous radiation and had the largest size of pharyngeal defect. Supraclavicular artery island flap was then applied to treat the fistula in these 2 patients, and the fistula was successfully healed without complication. Supraclavicular artery island flap was proved to be an effective approach to deal with pharyngocutaneous fistula in patients with laryngopharyngeal cancer with prior radiotherapy.
When looking back to the details of the 2 cases where initial conservative treatment was ineffective, we found that the invaded boundary of tumor was much wider, which resulted in greater fistula size. In addition, both patients had received higher dose of radiation and had diabetes, which might hinder fistula closure.
The pharyngocutaneous fistula is a bothersome postoperative challenge for patients with laryngeal or laryngopharyngeal cancer, especially when they have received radiotherapy. The rate of fistula increased significantly when the dose of radiotherapy exceeded 40 Gy. 7 Radiation can cause vascular occlusion and poor blood supply in the irradiation area. After radiotherapy, tissue regeneration ability is significantly impaired. Additionally, local scar and tension reduce the plasticity of the flap, making it difficult to be sutured. Therefore, the flap technique was widely employed in pharyngocutaneous defects reconstruction. An ideal flap for pharyngocutaneous fistula closure should meet the following requirements: first, the flap can reconstruct the inner side and outer surface of fistula at the same time; second, the color and texture of the flap donor tissue should be similar to tissue in the anterior neck area; finally, the flap should be easily available and be viable after operation.
There are 2 kinds of flaps for head and neck defects: free flap and pedicled flap. The free flap is represented by forearm flap and anterolateral femoral flap.8,9 This kind of flap technique requires high microvascular anastomosis skills, and the operation is complex and time-consuming. Because of severe scarring, adhesion and poor blood supply are common in the pharyngeal fistula area of patients with postoperative radiotherapy, it is difficult to find appropriate vessels for blood supply in the affected area of anastomosis. 10 In contract, the vascular pedicled myocutaneous flap has promising results in reconstructing pharyngeal fistula.11,12
All patients enrolled in this study had received radiotherapy in the neck, and the platysma myocutaneous flap around pharyngeal fistula was not suitable for repairing the pharyngeal fistula. Considering the sternocleidomastoid branch of the superior thyroid artery and its associated veins maybe damaged in cervical lymph node dissection procedure, the role of sternocleidomastoid muscle flap in defect reconstruction is limited. At the same time, the pectoralis major myocutaneous flap is too thick to be folded, which will cause the lack of free skin grafts in the outer surface of fistula. And the skin grafts are difficult to survive because of poor condition surrounding the fistula.
Supraclavicular artery island flap is a kind of fasciocutaneous flap with vascular pedicle, which has been widely employed in reconstruction of the defects of head and neck area, including the mouth base, tongue, 13 oropharynx, 14 hypopharynx, 15 larynx,4,16 and the neck skin. 17 When repairing defect after laryngectomy, the SAIF is a viable alternative for the classical free flap, such as forearm flap and anterolateral thigh flap.15,18 Previous study has reported that SAIF could be used in pharyngocutaneous and tracheoesophageal fistula closure, 17 although patients in this report did not receive prior radiation.
Supraclavicular artery island flap is an optimal treatment strategy for the reconstruction of pharyngocutaneous fistula after surgery in patients with laryngopharyngeal cancer with prior radiotherapy. Because of the constant vascular anatomy, rich blood supply and large-area tissue flap, the SAIF appears to be safer and more reliable in defects repairing. Simultaneously, it can repair the inner side and outer surface of fistula by double folding technique because the flap is thin, soft, and easy to shape. Moreover, it is hairless and its skin color is similar to the face and neck.
The transverse cervical artery and the supraclavicular artery are mainly located in the level V region of cervical lymphatic drainage. Squamous cell carcinoma of the upper respiratory and digestive tract rarely metastases to the lymph node in level V region. Therefore, the transverse cervical artery is safe to be the pedicle. The proximal part of the transverse cervical artery is located in the IV region of the neck, so the transverse cervical artery should be carefully dissected and well protected if lymph node dissection is needed in the IV region. If the transverse cervical artery is invaded, the contralateral supraclavicular artery flap can be used for reconstruction. In a study by Razdan et al, 5 the author considered that SAIF is safe for the patients who have received radiotherapy on the neck or who have had neck dissection in region V on the ipsilateral side. In our opinion, when managing this kind of patients, preoperative ultrasound Doppler is needed to explore whether there are available blood vessels in the bilateral transverse cervical artery and supraclavicular artery, and to find the side with better vascular conditions. The location of the course of the transverse cervical artery and supraclavicular artery should be marked, which can guide the harvest of SAIF.
Conclusion
Supraclavicular artery island flap is a safe and reliable fasciocutaneous regional flap. It can be used by double folding technique in the reconstruction of pharyngocutaneous fistula after surgery in patients with laryngopharyngeal cancer previously treated with radiotherapy, especially those who have received high-dose radiation and have large fistula size. Preoperative ultrasound Doppler is helpful to explore the condition of transverse cervical artery and supraclavicular artery. More studies are required to further evaluate the potential of SAIF as first-line treatment of pharyngocutaneous fistula after surgery in patients with laryngopharyngeal cancer with prior radiotherapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Special Financial Project of Fujian Province [Grant numbers: 2019B022]; Minimally Invasive Medical Fund of Fujian Province [Grant numbers: 2104519#]; Medical Innovation Project of Fujian Province [Grant numbers: 2017-CX-23].