
Abstract

The development of postlaryngectomy pharyngocutaneous fistula is not only a troublesome complication for the clinician, it frequently heralds a frustratingly long healing course for the patient. From its presentation until restoration of oral feeding, the clinician and patient may watch with discouragement as a small fistula expands into a full wound breakdown with the unsafe exposure of the great vessels and necessity of corrective flap surgery.
The current accepted practice of “organ preservation therapy,” with high doses of radiation and concomitant chemotherapy, has amplified the rate of pharyngocutaneous fistulae after salvage laryngectomy. It is universally accepted that prior radiation treatment significantly increases the occurrence of fistulae by up to 50%, and likewise, flaps appear to diminish their incidence and ameliorate their worsening.
1
Other clinical features, including hypoalbuminemia, hypothyroidism, diabetes, anemia, other comorbidities, and the presence of a preoperative tracheotomy, are often mentioned but are less crucial factors.
2
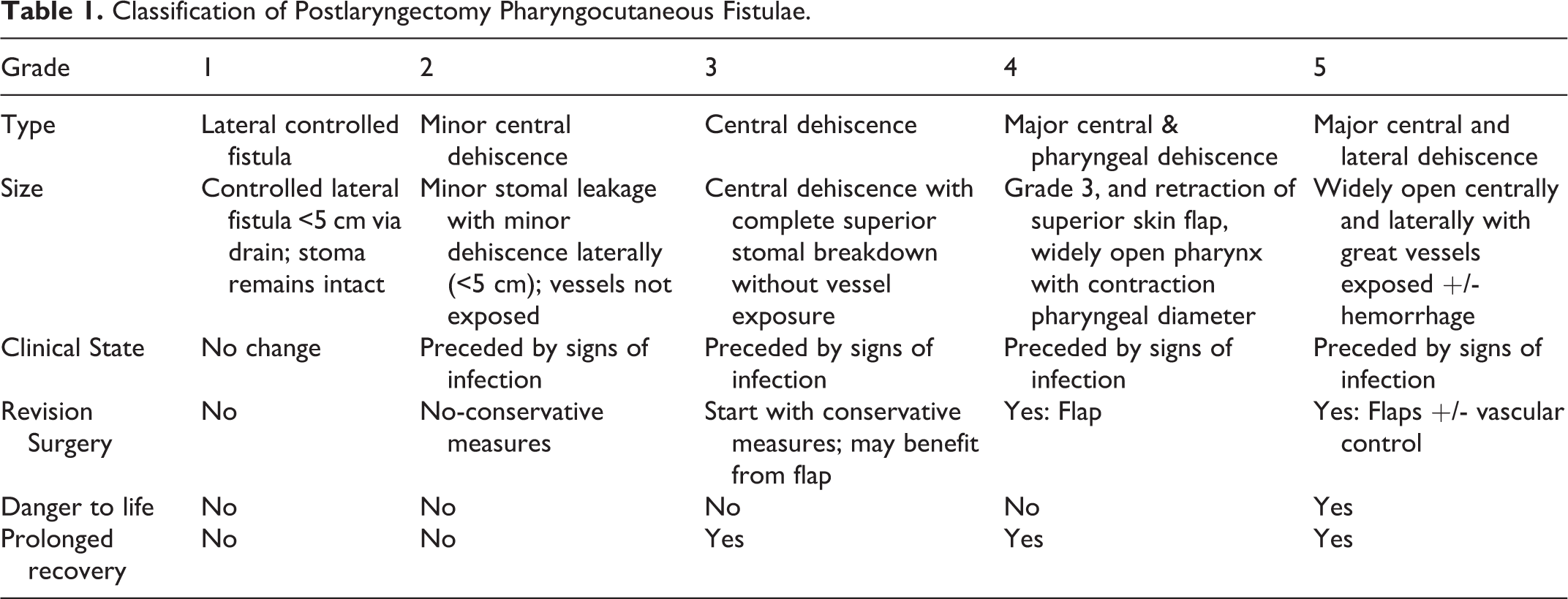
However, once a fistula develops, the clinician is faced with an open wound of varying degrees and must decide whether patience and supportive measures are adequate, or a more aggressive surgical repair is indicated. After many such trials and tribulations (25 postradiation and 10 without prior radiation), we have tried to organize these fistulae into safe fistulae as opposed to more ominous ones. This novel, clinical, classification (Table 1) for postsurgical complications enables: Reliable recording and interpretation of results, permitting accurate comparison of institutions and differing surgical techniques. A consistent decision-making algorithm regarding surgical revisions or other related procedures, and Evaluating more accurately the patient’s prognosis, length of hospitalization, and economic expenses.
Classification of Postlaryngectomy Pharyngocutaneous Fistulae.
The clinical staging, based on our cohort of patients, was approved by the local internal review board (Helsinki: 0102-15-HMO).
This classification includes
Grade 1: Essentially a controlled fistula (<5 cm in diameter) via the lateral neck drain without further breakdown and without changes in the clinical state. The stomal integrity is maintained with no leakage. This is considered a safe fistula and it heals quickly by conservative measures.
Grade 2: Minor central dehiscence with stomal leakage; superior stomal integrity is maintained; the great vessels are not exposed. There may be a minor dehiscence <5 cm lateral to the stoma which may be preceded by signs of infection. The fistula is safe and is most likely to heal by conservative measures.
Grade 3: Central wound dehiscence, with complete superior stomal dehiscence from the superior skin flap, without great vessel exposure, but with copious salivary secretions. Although it is a safe fistula and conservative measures may suffice, revision surgery with a flap accelerates full healing.
Grade 4: Major central wound dehiscence with retraction of the superior skin flap, exposing a widely open neopharynx and subsequent contraction of the pharyngeal mucosal diameter. Although a safe fistula from the point of view of vascular rupture, flap reconstruction of the skin and pharyngeal remnants is required.
Grade 5: Wide breakdown, both centrally and laterally, with exposure of the great vessels and concomitant high risk of rupture. This is the classic unsafe fistula which requires urgent insertion of a flap for coverage of the vessels and subsequent fistula closure. Life-threatening hemorrhage may require additional intervention with either angiography or ligation of the carotid artery.
The intent of these specific categories is to portray a progressive spectrum of complications, which would properly reflect the clinical problems. We have attempted to address 3 aspects of fistulae which may have impact on the decision to undergo revision surgery—great vessel exposure, superior skin flap retraction, and contraction of the pharyngeal diameter, all requiring revision surgery with flap reconstruction. Although supportive perseverance suffices in grades 1 to 2, further surgery is recommended in grades 3 to 4 and is required in grade 5 breakdown. The wound healing in radiated fields is consistently unreliable and frequently worsen making reassessment of treatment decisions a daily ritual. We hope this classification prompts better assessment and routing of patient care, enabling better outcomes. Using the classification will allow better documented, quantified measures essential for future studies investigating time/percentage of fistula healing, other complications, need for surgical intervention, possible directed nonsurgical medical treatment, and so on.
This classification stratifies pharyngocutaneous fistulae into easily recognizable categories of patients, allowing better comparison and aiding the clinician with bedside decision-making.
Footnotes
Authors’ Note
J.M.W. and R.E. contributrd equally.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.