
Abstract
Lacrimal drainage system disorders leading to epiphora are a common ophthalmologic complaint. When such a patient is identified, the ophthalmologist frequently collaborates with the otolaryngologist to perform a dacryocystorhinostomy (DCR). In rare cases, sinonasal sarcoidosis may lead to nasolacrimal duct obstruction (NLD) and dacryocystitis. A 48-year-old Caucasian female was referred to the Otolaryngology clinic for evaluation of a 6-month history of persistent right-sided nasal obstruction and epiphora. After physical examination and computerized tomography (CT) scan, she was diagnosed with right NLD with dacryocystitis. The patient underwent right endoscopic DCR. Pathology from the lacrimal bone and nasal tissue demonstrated noncaseating granulomas suggestive of sarcoidosis. Postoperative evaluation including lung CT scan confirmed systemic sarcoidosis. Nasolacrimal duct obstruction very rarely is the presenting symptom in patients with sarcoidosis. Imaging is necessary to rule out other causes of NLD, and histopathology is essential for diagnosis. Noncaseating granulomas are found along the nasal tissue and lacrimal sac, specifically in the subepithelial layer. Treatment consists of DCR, either endoscopic or external. Both approaches achieve long-lasting resolution of symptoms but may require revision from inflammation and scarring. There is no consensus on the use of intraoperative or postoperative steroids.
Introduction
Lacrimal drainage system disorders leading to epiphora are a common ophthalmologic complaint. When such a patient is identified, the ophthalmologist frequently collaborates with the otolaryngologist to perform an endoscopic dacryocystorhinostomy (DCR). This procedure involves unroofing the lacrimal bone and marsupialization of the lacrimal sac into the nasal cavity. The procedure can be performed either endoscopically or externally based on the surgeons’ experience.
Lacrimal drainage obstruction commonly presents in adulthood and can be either a primary/idiopathic or secondary to inflammatory, traumatic, neoplastic, or structural causes. 1 Resulting stasis of fluid within the lacrimal sac frequently leads to bacterial infection, termed dacryocystitis. The primary etiology, in almost 90% of cases, is characterized pathologically by nonspecific chronic inflammation with or without fibrosis. 1 However, it is important to maintain a certain level of suspicion for other systemic or neoplastic processes.
Sarcoidosis is a multisystem, autoimmune granulomatous disorder of unknown etiology which most commonly presents with pulmonary symptoms, but can affect any area of the body including the nasal passages and perinasal tissues. 2 It is more common among African Americans and female patients, especially between ages 20 to 40. 2 In rare cases, sinonasal involvement may lead to nasolacrimal duct obstruction (NLD) and dacryocystitis.
In this report, we present the case of unilateral NLD and dacryocystitis as the initial presentation for systemic sarcoidosis. We also present an updated literature review on the incidence of dacryocystitis in sarcoidosis patients.
Case Report
A 48-year-old Caucasian female was referred to the otolaryngology clinic for evaluation of a 6-month history of persistent right-sided nasal obstruction and epiphora. These symptoms had begun after an episode of acute sinusitis treated by the primary care physician with a course of oral antibiotics and intranasal corticosteroids. Complete head and neck exam including nasal endoscopy was unremarkable. A computerized tomography (CT) scan of the sinuses revealed left deviation of the mid portion of the nasal septum, diffuse mild mucosal thickening of the paranasal sinuses, but otherwise normal anatomic variations. In conjunction with ophthalmologic consultation, a diagnosis of right NLD with dacryocystitis was made.
The patient failed conservative therapy including lacrimal duct irrigation, so endoscopic DCR was performed. Intraoperatively, there was purulence in the lacrimal sac, but grossly normal anatomy of the nasal cavity except mildly inflamed mucosa. There were no discrete mucosal or submucosal intranasal lesions appreciated. The nasal mucosa and lacrimal bone that were removed were sent for histologic examination and cultures were performed. Pathology demonstrated noncaseating granulomas suggestive of sarcoidosis (Figure 1). The Ophthalomlogy team placed bicanalicular Crawford tubes along the superior and inferior puncti, and secured these to the nasal cavity with a 6-0 silk suture.
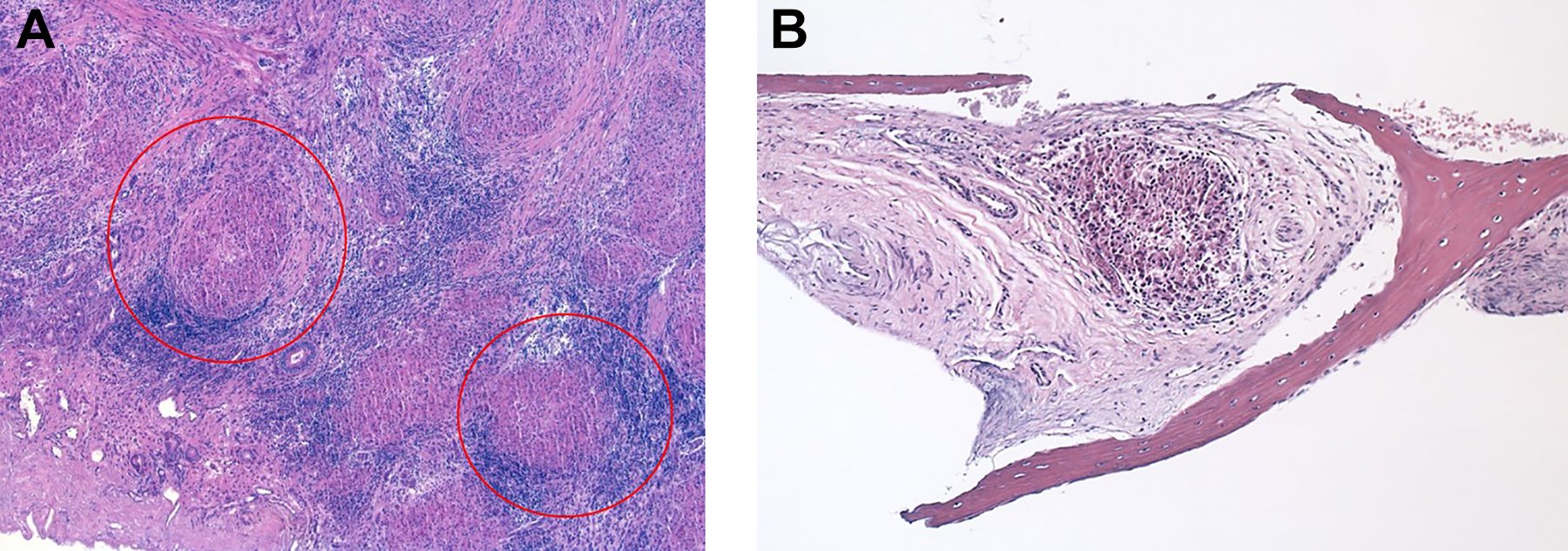
A and B, H&E pathologic preparations of our patient’s surgical pathology. A, Medium magnification view of noncaseating granulomas (examples are red circled). B, Noncaseating granuloma involving lacrimal bone.
Post-operatively patient was placed on nasal saline, without need for ophthalmic medication. On further questioning, the patient reported nonspecific history of arthralgias and arthritis affecting multiple joints as well as fatigue and dyspnea for several years. Review of systems was otherwise noncontributory. Workup for sarcoidosis was initiated and included referral to rheumatology and pulmonology, CT scan of the chest, and autoimmune laboratory tests. Blood work revealed a mildly elevated C-reactive protein level, but normal angiotensin-converting enzyme levels. Computerized tomography scan of the chest showed bilateral bulky partially calcified hilar and mediastinal lymph nodes (Figure 2). A diagnosis of sarcoidosis was made and the patient was started on prednisone daily, with symptomatic improvement. Prednisone was begun at 30 mg daily for 3 weeks, then 20 mg daily for 3 weeks, and finally 15 mg daily with plan to complete a total of 6 months of treatment. She also reported almost complete resolution of nasal congestion and epiphora at her 6 week post-operative visit. Crawford stents were removed at 7 weeks post-operatively by the Ophthalmology team. Her last documented follow up at 4 months post-op continued to show resolution of her nasal and ophthalmic symptoms.
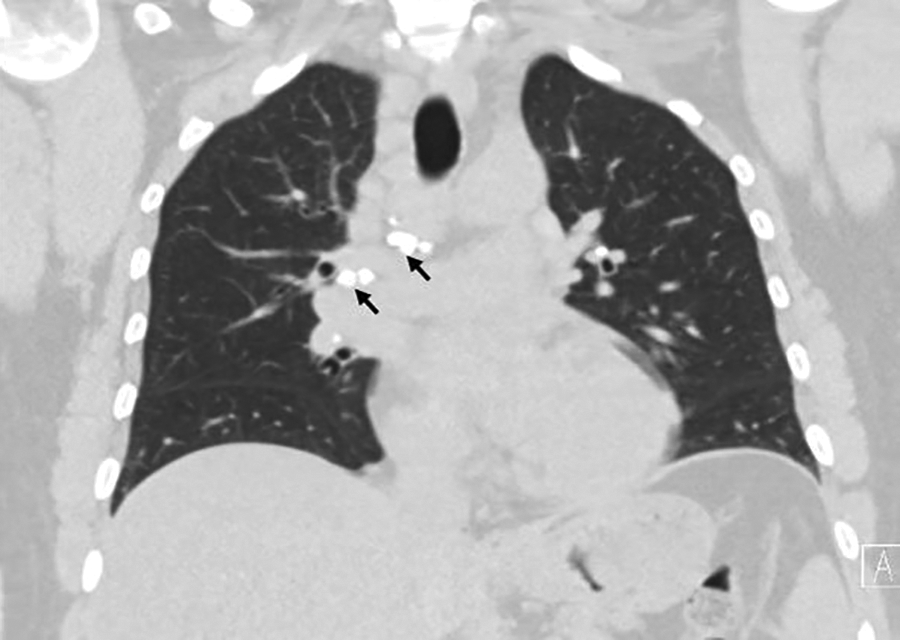
Representative coronal cut of our patient’s CT scan of the chest, showing bulky bilateral partially calcified perihilar and mediastinal lymphadenopathy (black arrows). CT indicates computerized tomography.
Discussion
The true incidence of sarcoidosis is unclear as the disease may be clinically silent or present with nonspecific generalized symptoms (weakness, fever, arthralgias, lymphadenopathy, weight loss). Patients rarely present with nasal or lacrimal duct problems as the first manifestation of the disease, and many are asymptomatic or afflicted to a minor degree and go undiagnosed for years, frequently with the ultimate diagnosis made incidentally by chest imaging. Our patient is a healthy Hispanic female, with no known history of sarcoidosis or pulmonary symptoms. While lung involvement is present in more than 90% of patients, any organ system can be affected, including the upper respiratory tract which includes the nasal passages, nasopharynx, and larynx. 3 Nasal symptoms are generally due to mucosal edema and irritation and are therefore nonspecific, and tissue biopsy is necessary for pathologic diagnosis. 4 The true incidence of lacrimal system or nasal mucosal involvement is unknown since routine pathologic involvement is not routinely done.5,6 Merkonidis et al reported that only 1% of DCR patients were found to have sarcoidosis on pathologic examination; Banks et al reviewed histopathology of the lacrimal sac after 769 consecutive endoscopic DCRs and found only 10 cases of sarcoidosis.5,6 Avisar et al in 2012 had 12 cases of sarcoidosis with NLD that required endoscopic DCR; 11 of these patients were already diagnosed with sarcoid prior to their operations. 7
Literature review of sarcoidosis-related NLD reveals that most cases are unilateral on presentation; however, Banks et al found that 3/10 patients with sarcoidosis presented bilaterally. Stewart et al performed 75 external DCRs in patients with previously diagnosed sarcoidosis and found about 60% of lacrimal sac biopsies had characteristic noncaseating granulomas in comparison to about 87% of nasal tissue biopsies. 8 Operative records from this study describe the nasal mucosa and lacrimal sac as “thickened,” “inflamed,” or “friable.” 8 Ishikawa et al identified noncaseating granulomas more specifically in the subepithelial layer of the lacrimal sac. They posit that lymphocyte recirculation along the lacrimal drainage–associated lymphoid tissue is the likely originating site for autoimmune disorders such as sarcoidosis. 9
Most authors recommend DCR for treatment of NLD in the setting of sarcoidosis. Both external and endoscopic DCR are reported to achieve sustained and complete symptom resolution7,10; however, a direct comparison between the 2 techniques has not been studied. There has been no evidence to suggest the need for intraoperative or postoperative steroid therapy. Stewart et al reported sustained resolution of symptoms in 53 of 56 patients undergoing primary external DCRs, of which 73% were not on systemic steroids, with a median follow-up of 34 months. 10 The authors propose creation of a wide mucosal tract to prevent inflammation or scarring that may require revision DCR. Our patient was treated with systemic steroids for her pulmonary disease for 6 months. Her lacrimal system presumably remains patent 36 months postoperatively.
Conclusion
Sarcoidosis is a systemic inflammatory disease of unknown cause, which may rarely present with primarily sinonasal symptoms. We describe a rare case of sarcoidosis presenting with NLD, an unusual initial presenting complaint of this condition, with very few reported cases in the literature. Histologic examination of the lacrimal sac and nasal tissue is key to making the diagnosis. Treatment consists mostly of DCR, and both endoscopic and external approaches show long lasting relief of symptoms. More information is needed on need for postoperative systemic steroids for prolonged treatment response.
Footnotes
Authors’ Note
The patient’s history, physical examination, operative reports, imaging, and pathology were accessed using Soarian Cerner electronic medical record, which is part of Tufts Medical Center. In accordance with the Tufts Health Sciences Institutional Review Board (IRB), single patient case reports are exempt from IRB review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.