
Abstract
Purpose:
To evaluate the improvement in epiphora and need for surgical revision in patients with acquired nasolacrimal duct obstruction following balloon-assisted, middle meatal endoscopic dacryocystorhinostomy with chitosan-based dressing versus bioresorbable polyurethane packing versus no packing.
Patients and Methods:
This was a retrospective study of consecutive adult patients seen from 2015 to 2018 with follow-up evaluation of epiphora at least 3 months after balloon-assisted, middle meatal endoscopic dacryocystorhinostomy. Patients with a history of prior punctoplasty, septoplasty, sinus surgery, or dacryocystorhinostomy of any kind were excluded. Those meeting criteria were stratified by postoperative hemostatic intervention: no packing, bioresorbable packing, and chitosan-based dressing (groups 1, 2, and 3, respectively). Procedural outcomes were graded as successes or failures based on subjective report and anatomical findings at most recent visit within an 18-month postoperative window. Instances of recommendation for revision surgery were also recorded.
Results:
Forty-three cases (36 patients) met the abovementioned criteria. Groups 1, 2, and 3 comprised 12, 17, and 14 cases each, respectively. Average patient age was 55.3 years old, and average duration of follow-up was 6.7 months. Significant variation in outcomes was detected across the 3 groups (P = .0495), particularly between groups 1 and 3 (P = .033). Use of chitosan-based dressing trended toward reduced rates of recommendation for surgical revision (P = .203, P = .113).
Conclusions:
Use of chitosan-based dressing after endoscopic dacryocystorhinostomy was associated with improved subjective and anatomical outcomes. It may also contribute to less frequent need for revision surgery. Further study in a larger prospective trial is recommended.
Introduction
Epiphora is a relatively common complaint with multifactorial etiology spanning lower lid malposition/laxity, nasolacrimal obstruction, punctal stenosis, and reflex tearing. 1 For those with epiphora secondary to nasolacrimal obstruction, dacryocystorhinostomy (DCR) is a proven efficacious surgical intervention. Numerous permutations of the procedure exist, encompassing external and endoscopic approaches with various modifications: drills and microdebriders, 2 lasers, 3 mucosal preservation methods, mitomycin C, 4 stenting, 5,6 flaps, radiofrequency, 7 and balloons. 8
Despite consistent report of adhesions and postoperative bleeding as predominant complications of endoscopic sinus surgery, including endoscopic DCR (eDCR), 9 postoperative care practices of sinus surgeons vary widely in part due to the lack of general consensus on adjunctive approach. 10 In general, morbidities associated with conventional gauze, cotton, and sponge nasal packing—namely scarring, pain, facial edema, and toxic shock syndrome—discourage its rather common use with certain exceptions (larger surgeries or revisions, grafting for cerebrospinal fluid leak, tumor resections, persistent bleeding, or patient history of recent aspirin use or hypertension). Hyaluronic acid–based and other bioresorbable dressings such as polyurethane NasoPore (Stryker Corp, Kalamazoo, Michigan) enhance hemostasis by resorbing water and stimulating clotting before dissolving in days. They reportedly reduce incidence of abovementioned morbidities but often without reducing the risk of granulation reactions, infection, and synechiae. 11
Chitosan is a bioresorbable, nontoxic chitin-derived complex carbohydrate used widely in the nutrition, agriculture, cosmetic, and textile industries for its antimicrobial, hydrating, and other properties. 12 Induction of endothelin production and promotion of red blood cell and platelet adhesion contribute to barrier formation and wound sealing in the surgical setting. 13 Multiple systematic reviews reported that, unlike conventional packing or most other bioresorbable dressings, chitosan-based gel reduced synechiae following endoscopic sinus surgery. No impact on crusting or infection was observed. Reviews also offered mixed evidence for improved granulation at the operative site. 11,14 More specifically, another study found that one type of chitosan-based hemostatic dressing was effective as a hemostatic agent across multiple DCR modalities. 15 A more recent addition to our practice, XeroGel (Entellus Medical Inc, Plymouth, Minnesota) is a biocompatible, dissolvable chitosan-based sponge that expands when hydrated to tamponade local intranasal structures, thereby minimizing postoperative bleeding and edema. 16
In the context of minimal consensus on preferred postoperative hemostatic management based on longer term clinical outcomes, the aim of this study was to evaluate improvement in epiphora and need for surgical revision in patients with acquired nasolacrimal duct obstruction (NLDO) following balloon-assisted, middle meatal eDCR with chitosan-based dressing versus other bioresorbable packing versus no dressing.
Patients and Methods
This was a retrospective review of the medical records of consecutive adult patients who underwent surgery for primary acquired NLDO over a span of 4 years (2015-2018). Ethics approval was obtained from the Institutional Review Board of Weill Cornell Medicine prior to enrolling study participants. The study adhered to the tenets of the Declaration of Helsinki and was Health Insurance Portability and Accountability Act of 1996 compliant with protection of individually identifiable health information.
All surgeries were performed via the middle meatus with balloon dilation using 2 consecutive 60-second inflations of 3 or 5 mm LacriCATH balloon catheter (Quest Medical Inc, Allen, Texas; Figure 1). Patients were retrospectively assigned to 1 of 3 groups based on intraoperative selection of hemostatic intervention. Group 1 received no packing or hemostatic dressing. Group 2 received standard bioresorbable polyurethane packing (NasoPore), and group 3 received bioresorbable chitosan-based dressing (XeroGel) immediately following the procedure. No other modifications were made to the procedure apart from dressing use.
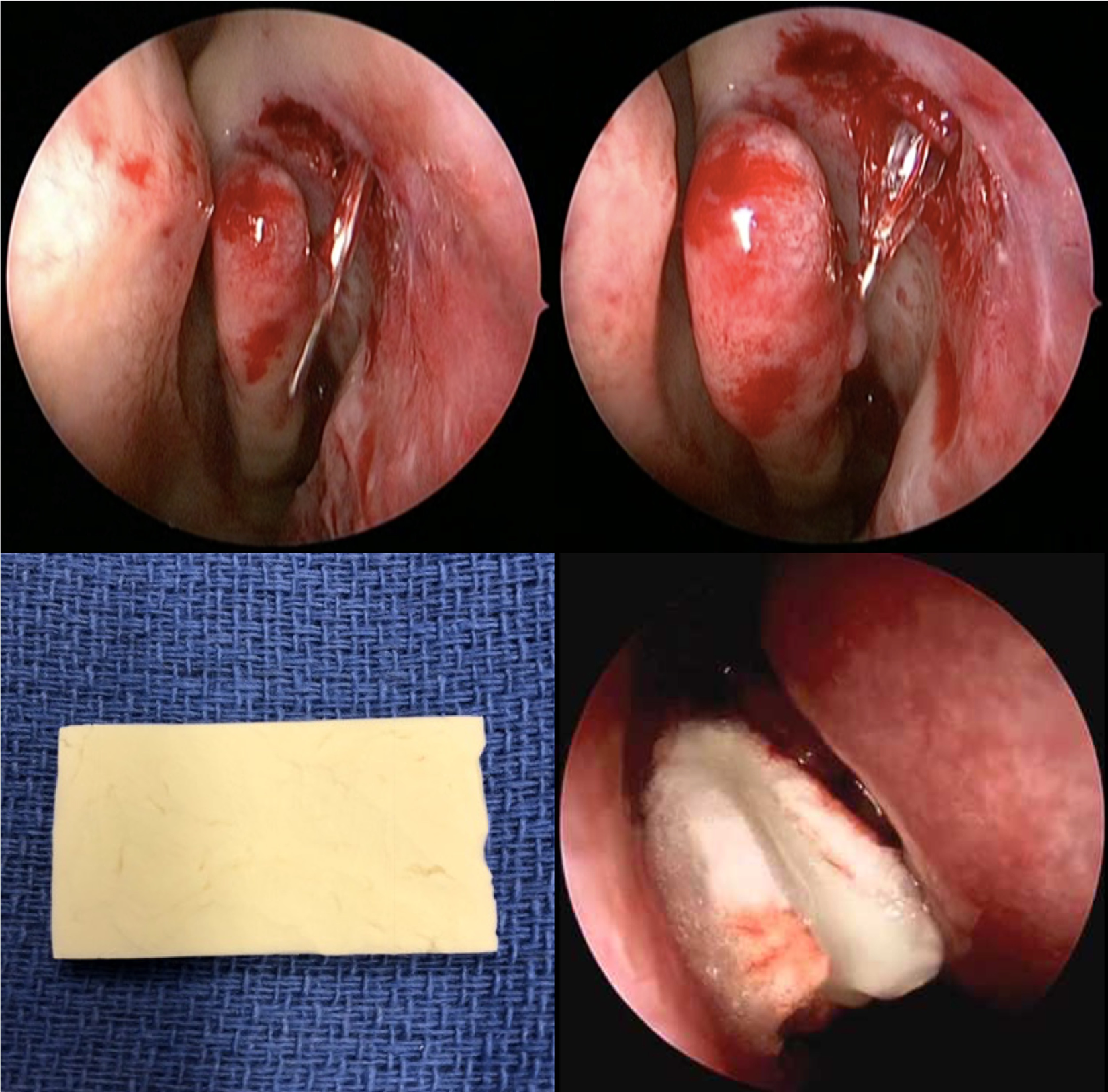
Insertion of balloon catheter probe into the middle meatal osteotomy (upper left). Inflation of the balloon catheter (upper right). Dry XeroGel prior to placement (lower left). XeroGel following intranasal placement (lower right).
Each patient was evaluated postoperatively in the clinic with a single question: “Do you feel improvement in your tearing?” Subjective report was corroborated by objective findings on irrigation performed in standard fashion using a drop of proparacaine, 26-gauge lacrimal cannula, and 3-mL saline syringe to irrigate through the lower punctum. Improvement in stenosis was assessed by estimating percentage of fluid reaching the nasal passage under gentle pressure with syringe when compared to that assessed preoperatively. Drawing upon findings of reduced rates of subjective relief of epiphora in comparison to those of anatomical success, 17,18 both subjective report of tearing and objective measure of stenosis/reflux on irrigation were deemed valuable to determination of operative outcome. As described by other groups using a binary scale, 8 success was marked by improvement in tearing and patency on irrigation, whereas failure was indicated by persistent/recurrent tearing and/or complete anatomical failure on irrigation. Moreover, need for surgical revision was confirmed in visit notes explicitly detailing that a discussion and recommendation of repeat surgery had taken place at follow-up.
Inclusionary criteria for the study entailed one or more postoperative follow-up visits with ophthalmology following eDCR. Evaluation at the most recent visit in an 18-month postoperative window was used to determine the result. Patients with a follow-up visit as early as 3 months after surgery were included to allow for tube removal and given reports of strong association between early and long-term postoperative results of eDCR using similar assessment criteria. 19 Patients with history of prior punctoplasty, septoplasty, sinus surgery, or DCR were excluded as were those with inadequate documentation or duration of follow-up.
Results
Retrospective review identified 43 cases in 36 patients (7 receiving bilateral eDCR) satisfying inclusion and exclusion criteria. Overall, 24 (55.8%) cases and 20 (55.5%) patients were female. Average case age was 55.3 ± 15.8 years old; average duration of follow-up was 6.7 ± 3.9 months.
Cases were stratified by postoperative hemostatic intervention into 3 groups: those receiving none (n = 12), standard bioresorbable packing (NasoPore, n = 17), and chitosan-based dressing (XeroGel, n = 14). Notably, all patients in this data set with bilateral procedures underwent identical interventions on either side. Average age, follow-up length, and gender distribution are depicted in Table 1.
Basic Patient Characteristics, Stratified by Intervention.
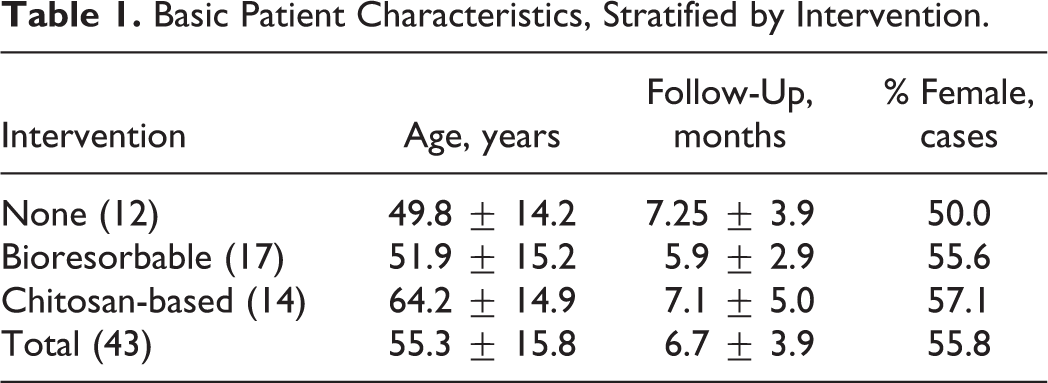
Two-sample Student t tests were conducted between stratified groups for age and follow-up length, yielding statistically significant differences in age between patients who received chitosan-based dressing and no intervention (P = .02) and between patients who received chitosan-based dressing and standard bioresorbable packing (P = .03). No significant associations were observed between postoperative intervention and duration of follow-up.
Freeman-Halton extension of the Fisher exact probability test was conducted for surgical outcome across groups 1, 2, and 3, the distribution of which is depicted in Table 2. A statistically significant difference among the groups was detected (P = .0495). Further analysis by 2-tailed Fisher exact probability test was conducted between each combination of groups (1 vs 2; 1 vs 3; and 2 vs 3). While no difference was noted between outcomes of groups 1 versus 2 (P = .682) or 1 versus 3 (P = .107) that of 1 versus 3 were found to be statistically significant (P = .033).
Contingency Table Charting Surgical Outcomes (Based on Subjective and Anatomical Findings) and Revision Recommendations, Stratified by Intervention.
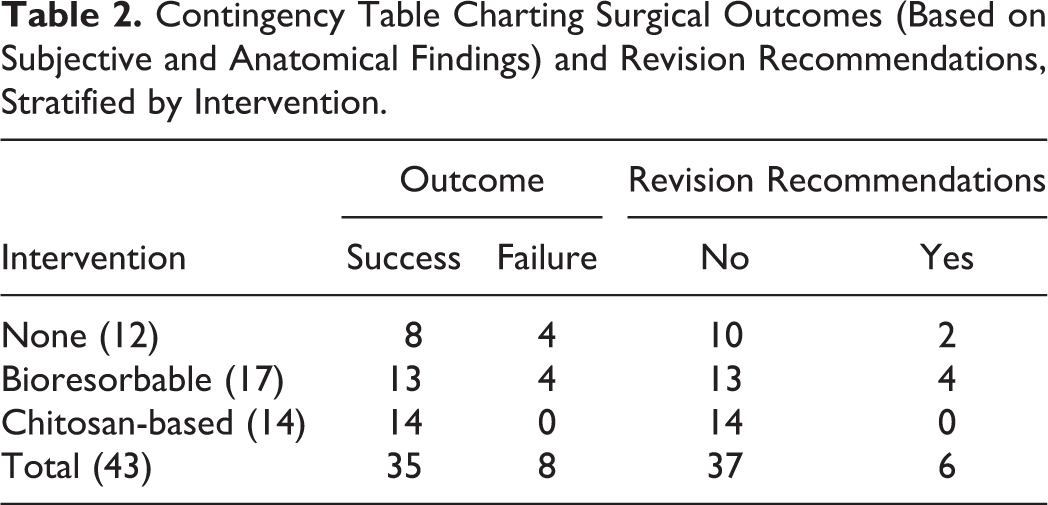
The 4 failures in group 1 were thought to arise in the setting of emergence of granulation tissue (n = 1), inflammation of the middle turbinate with septal deviation (n = 1), or underlying eosinophilic angiocentric fibrosis of the nasal cavity at baseline (n = 2). Those in group 2 were at least partially attributed to granulation tissue (n = 1), recurrent dacryocystitis (n = 1), or concurrent common canalicular obstruction at the time of surgery (n = 2). Ultimately, revision surgery was recommended for 16.6%, 22.2%, and 0% of patients in groups 1, 2, and 3, respectively (Table 2), with septoplasty also recommended for a single case. The 2-tailed Fisher exact probability test was conducted once more for recommendation rates between group pairings, yielding nonsignificant differences for 1 versus 2 (P = 1), 1 versus 3 (P = .203), and 2 versus 3 (P = .107).
Discussion
Rationale: Surgical Technique
For the purposes of this study, a middle meatal endoscopic approach with dilation by balloon catheter was selected as the standard of care for multiple reasons. First, although older studies cite inferior success rate with an endoscopic as opposed to external approach, 3,20 a more recent large systematic review cited success rates between 84% and 94% for eDCR and 65% and 100% for external DCR. 21 Despite a strict learning curve associated with the techniques required for endoscopic surgery, experienced surgeons more recently describe comparably, if not improved success rates, shorter operative time and recovery, fewer complications, and increased patient satisfaction compared to traditional external DCR. 22 -25 Similarly, balloon DCR is associated with shorter operative time and reduced postoperative pain compared to a conventional endoscopic procedure without sacrifices in efficacy, safety, or patient quality of life. 8,26 Therefore, in studying this particular surgical procedure, we sought to explore the extent to which an already highly regarded procedure could be improved.
Limitations
This study utilized a small sample size, especially after stratification. Its retrospective, nonrandomized, nonmatched nature elicits concern about how interventions were selected over the course of study. Decision-making was largely dictated by operating room stocking and availability without consideration of the case itself. As time passed, ENT surgeon colleagues provided anecdotal evidence of improved hemostasis and scarring after functional endoscopic sinus surgery also supported in the literature. 27 Therefore, our practice pattern gradually evolved to use XeroGel more frequently over the course of study. As such, surgeon experience is naturally a potential confounder in regard to outcomes, given temporal trends in dressing selection. However, all surgeons involved had been performing various permutations of eDCR for at least 10 years prior to the first documented case, therefore likely having surpassed the procedure’s “learning curve” at that time. Fisher exact probability test for cases performed in 2015 to 2016 versus 2017 to 2018 also failed to yield statistically significant difference in surgical outcomes (P = .99), thus discouraging a presumed temporal influence on outcomes. Additionally, we recognize that a significantly older mean age was noted for the cohort receiving chitosan-based dressings, but given that advanced age has been associated with poor prognosis following eDCR for epiphora and dacryocystitis, 5 it was thought that the older mean age of the chitosan cohort would have obscured additional benefit observed with that particular intervention, if anything.
It remains to be seen how generalizable the findings of this study are to other permutations of eDCR—for example, in targeted approaches via the inferior meatus, without balloon dilation, and so on. Again, another study documented use of chitosan-based dressings after DCR, but in only 2 endoscopic cases. 20 Shared characteristics of alternative procedures (patient anatomy, surgical equipment, and particular technical aspects) and generalities in hemostatic and wound-healing mechanisms may lead one to believe that a comparable benefit is feasible in similar procedures.
Implications
To our knowledge, this is the first study investigating epiphora and need for revision after eDCR under these particular conditions: with application of dissolvable chitosan-based dressing and using a middle meatal approach with balloon dilation. Results support the notion that use of a chitosan-based dressing (rather than standard bioresorbable packing or no packing whatsoever) is associated with high-quality outcomes and reduced need for recommendation of surgical revision, albeit insignificantly so in a rather small sample. Findings justify initiation of larger, randomized prospective studies to lend additional credibility to either claim.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an unrestricted grant from Research to Prevent Blindness.