
Abstract
Objectives:
Chronic suppurative otitis media (CSOM) induced tympanic membrane perforation (TMP) can be accompanied by anterior mallear ligament (AML) calcification. So far, comparative evaluations of TMP with and without AML calcification have rarely been reported. The aim of the current study is to compare the hearing outcomes of TMP with and without calcification of AML under transcanal endoscopic type I tympanoplasty.
Methods:
Records of 67 patients diagnosed with CSOM and receiving transcanal endoscopic type I tympanoplasty were divided into the AML calcification group (Cal group, n = 31) and the non-AML calcification group (non-Cal group, n = 36). The 31 patients in the Cal group were divided into subgroup A and B according to the severity of calcification. The operation time, closure rate, and pre- and postoperative audiometric results were retrospectively collected and analyzed.
Results:
Preoperatively, the Cal group had higher mean air–bone gap (ABG; P = .022), and ABGs at 250 Hz (P = .017) and 500 Hz (P = .008) compared with the non-Cal groups. The Cal group showed higher improvements of ABGs at 250 Hz (P = .039) and 500 Hz (P = .021) compared with the non-Cal groups postoperatively.
Conclusions:
The TMP with AML calcification leads to higher ABGs at low frequencies. The hearing outcomes are similar for TMP both with and without AML calcification after surgery. Our results suggest that transcanal endoscopic type I tympanoplasty is an appropriate surgical method for TMP with AML calcification, if the lesion can be detected and completely eliminated.
Keywords
Introduction
Chronic suppurative otitis media (CSOM) is a chronic inflammation of the middle ear and mastoid, which affects more than 300 million individuals worldwide. 1,2 Patients suffered from CSOM present with tympanic membrane perforation (TMP), recurrent otorrhea, conductive hearing loss, and cholesteatoma formation. 3,4 The infection may initially lead to pure TMP without other alterations in the middle ear. However, prolonged inflammatory stimulation can result in additional lesions of ossicular chain (OC). Ossicular chain involvement is quite common in the CSOM, and the prevalence is estimated up to 33%. 5 Postinflammatory pathological changes include hyalinization of collagen, fibrosis and calcification of epithelium and ligament, new bone formation, and tissue necrosis. 6 All these changes contribute to fixation, disconnection, and erosion of the OC.
Calcification of the anterior mallear ligament (AML), which may result in partial fixation of malleus, can be easily ignored during middle ear surgery. 7,8 In a research on revision surgery for otosclerosis cases, fixation of malleus caused by AML calcification was detected intraoperatively in 37.5% of cases and was supposed to be the main reason for unsatisfactory hearing improvement after initial surgery. 9 Instead of conventional microscopic ear surgery, the transcanal endoscopic surgical system developed recent years provides a clearer wide field of vision, which may increase the detection of AML calcification. Theoretically, the AML can be pathologically altered by long-term inflammation in the process of CSOM. However, few studies have reported the AML calcification involvement in CSOM cases.
The TMP induced by CSOM causes a mild hearing loss. However, the addition of malleus fixation may lead to augment of hearing threshold for 10 to 30 dB. 10 Therefore, surgical treatment is required for the purpose of repairing the tympanic membrane and improving the hearing. Tympanoplasty was first systematically proposed by Wullstein and Zollner in the 1950s and became a classical surgical method for CSOM. 11,12 Type I tympanoplasty referring to pure myringoplasty without OC reconstruction is suitable for TMP with an intact and mobile OC. When TMP accompanied by partial fixation of OC, options exist: myringoplasty after freeing the OC, or OC reconstruction with prosthesis. Seidman and Babu demonstrated in otosclerosis cases that remobilizing the OC by laser and drilling could provide marked hearing improvement without prosthesis implantation. 13 However, few researches have focused on the effect of type I tympanoplasty on TMP with calcification of AML. Herein, we conducted the current study to compare the audiological characteristics and surgical outcomes of TMP with and without calcification of AML under transcanal endoscopic type I tympanoplasty.
Patients and Methods
This retrospective study was conducted with the approval of The Medical Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University. Totally 67 patients diagnosed with CSOM and underwent surgical treatment at the Department of Otolaryngology, Head and Neck Surgery, The First Affiliated Hospital of Wenzhou Medical University between July 2018 and May 2020, were included. The data of patients who met the following inclusion criteria were analyzed: (1) no occurrent otorrhea, (2) receiving type I tympanoplasty under transcanal endoscope, (3) TMP with no evidence of lesions in the tympanic cavity except for the AML calcification, and (4) complete records of preoperative and 6-month postoperative audiogram. Patients with OC disconnection or erosion, otosclerosis, myringosclerosis, active otitis media, cholesteatoma, tumors, revision surgery, or without follow-up compliance were excluded.
According to surgical exploration and operation notes from the electronic medical records system, AML calcification was identified with following criterions: (1) directly seen calcificated AML or a calcific plaque observed between the anterior process of malleus and the anterior wall of epitympanum; (2) the AML was adhered to or wrapped in calcific plaque; or the AML was disappeared in the tympanic cavity after carefully removing the calcific plaque, if the presence of AML in the calcific plague was unable to judge. The 67 patients were divided into 2 groups according to the condition of AML: the Cal group consisted of 31 patients with calcificated AML (Figure 1A), while the non-Cal group consisted of 36 patients with normal tympanic cavity, in absence of any lesions (Figure 1B). Then, the 31 patients in the Cal group were divided into subgroup A (calcification limited around the AML) and subgroup B (calcification completely or near completely filling the anterior epitympanum) according to the severity of calcification. Pure tone audiometry was performed for each patient preoperatively and 6-month postoperatively. The air–bone gaps (ABGs) at the frequencies of 250, 500, 1000, 2000, and 4000 Hz, and the mean ABG at the frequencies of 500, 1000, 2000, and 4000 Hz were calculated according to the air and bone hearing thresholds. A postoperative mean ABG of 20 dB or less in the patients with a preoperative ABG of more than 20 dB was considered successful.
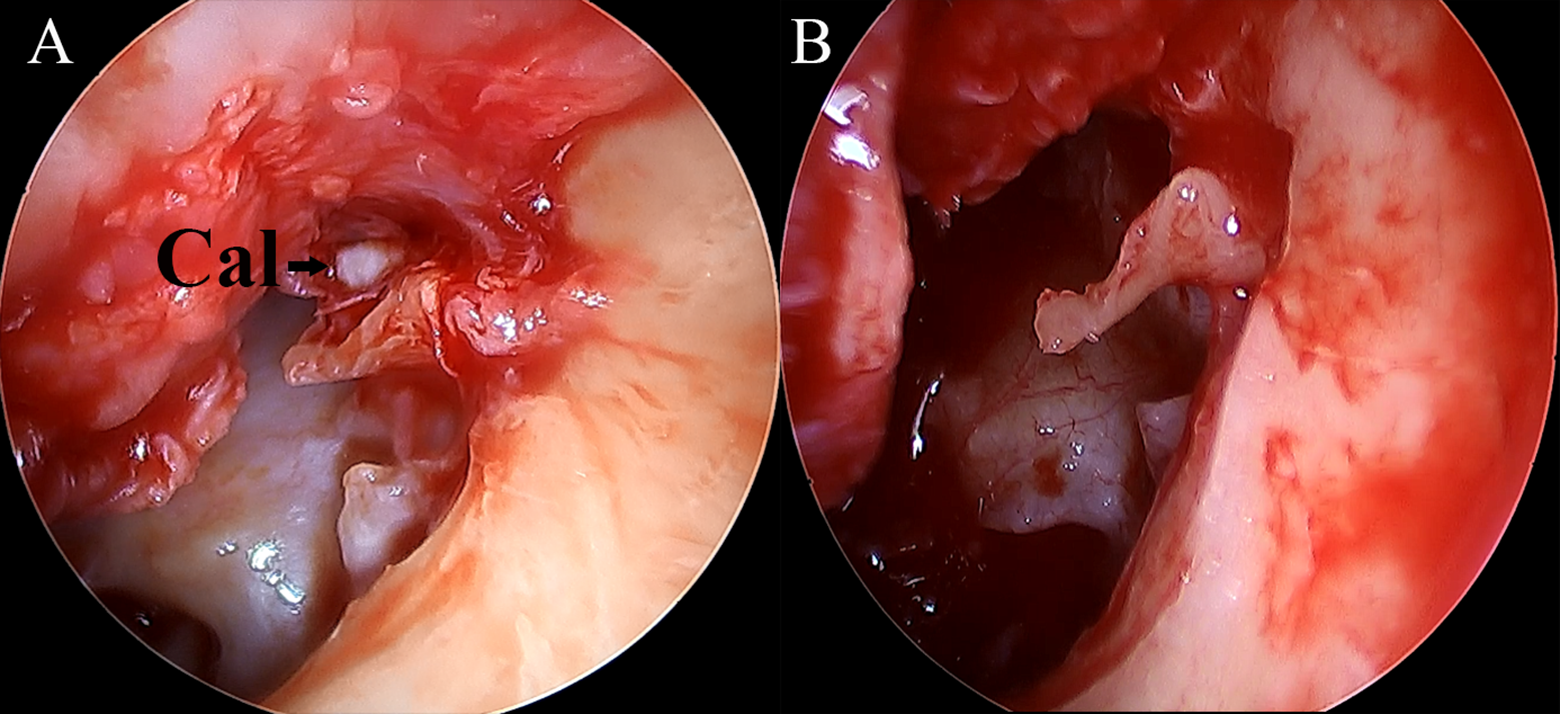
Representative images of tympanic cavity exploration intraoperatively. (A) Tympanic cavity of a patient in the Cal group, black arrow indicates the calcification of AML, (B) tympanic cavity of a patient in the non-Cal group, no calcification is detected.
Surgical Technique
All patients received transcanal endoscopic type I tympanoplasty operated by one senior otologist under general anesthesia. Margin of the perforation was freshened and tympanomeatal flap was elevated. Tympanic cavity was explored under transcanal endoscope. Ossicular chain mobility and continuity was assessed. Round window reflex was evaluated. If the AML calcification was detected intraoperatively, the lesion was completely removed and the recovery of OC mobility was confirmed before type I tympanoplasty; otherwise, type I tympanoplasty was performed in the same way except for skipping the debridement of the tympanic cavity. The cartilage perichondrium obtained from the ipsilateral tragus cartilage was placed in an underlay way for repairing the TMP. The tympanic cavity and the tympanic membrane graft were filled and covered with gelatin sponge particles. And the external auditory canal was stuffed with erythromycin spun yarn. Prophylactic antibiotics were used for 7 days after surgery. Post-operation follow-up lasted at least 6 months. The tympanic membrane closure and hearing outcomes 6 months after surgery were recorded.
Statistical Analysis
Statistical analyses were performed with SPSS (Version 22.0, IBM) for Windows. Quantitative variables were presented as mean ± standard deviation (SD) if normal distributed or quartiles (median, [P25, P75]) if non-normal distributed. Categoric variables were expressed as percentages. Differences in gender, surgical site, and perforated size between the 2 groups were examined by Pearson c2 tests. Difference in success rate was analyzed by Fisher exact test. Differences in age, operation time, and hearing outcomes in normal distribution were examined using independent t tests. Hearing outcomes in non-normal distribution were evaluated by Mann-Whitney U test. A value of P < .05 was considered as statistically significant.
Results
Data of 67 patients with CSOM were finally included and analyzed in this study. The study population consisted of 23 (34.33%) males and 44 (65.67%) females, with an average age of 45.99 ± 11.74 years. Transcanal endoscopic type I tympanoplasty operations were performed in 38 (56.72%) left ears and 29 (43.28%) right ears. The characteristics of the Cal and non-Cal groups are presented in Table 1. No significant differences were demonstrated between the 2 groups in age, gender, surgical site, or perforation size.
Characteristics of Patients in the AML Calcification and Non-AML Calcification groups.a
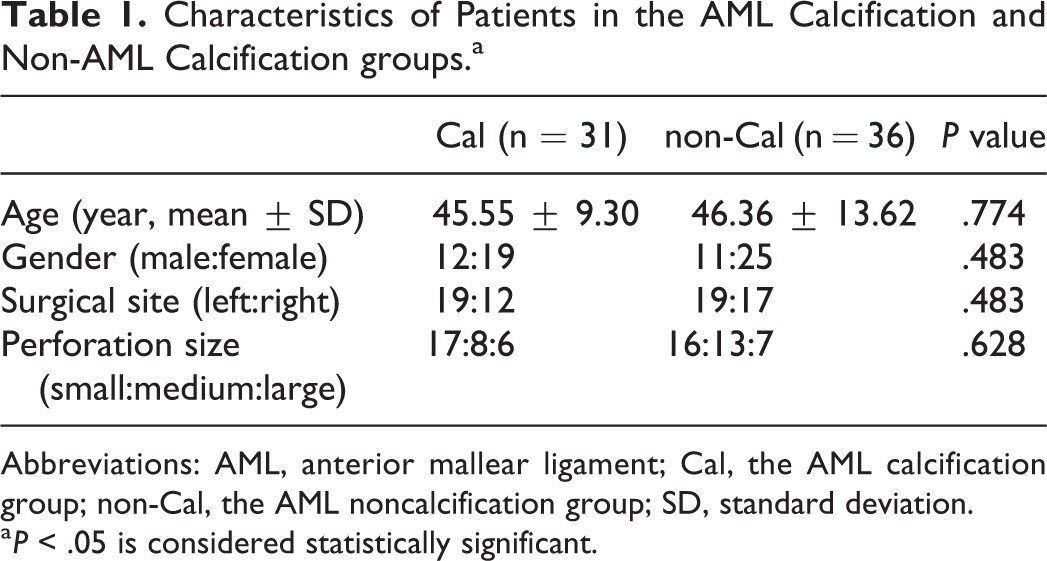
Abbreviations: AML, anterior mallear ligament; Cal, the AML calcification group; non-Cal, the AML noncalcification group; SD, standard deviation.
a P < .05 is considered statistically significant.
As shown in Table 2, all patients of both groups had complete healing of TMP 6 months after surgery (closure rate 100% vs 100%). Patient who showed a mean ABG of more than 20dB preoperatively achieved a postoperative mean ABG of less than 20dB was considered successful. Of the 22 patients who had mean ABG >20dB preoperatively in the Cal group, 21 achieved successful outcomes, while 17 of 21 patients obtained successful outcomes in the non-Cal group. No significant difference was observed between the 2 groups in success rate. And the comparison of operation time between the 2 groups showed no significant difference.
Surgical Outcomes of the AML Calcification and Non-AML Calcification Groups.a
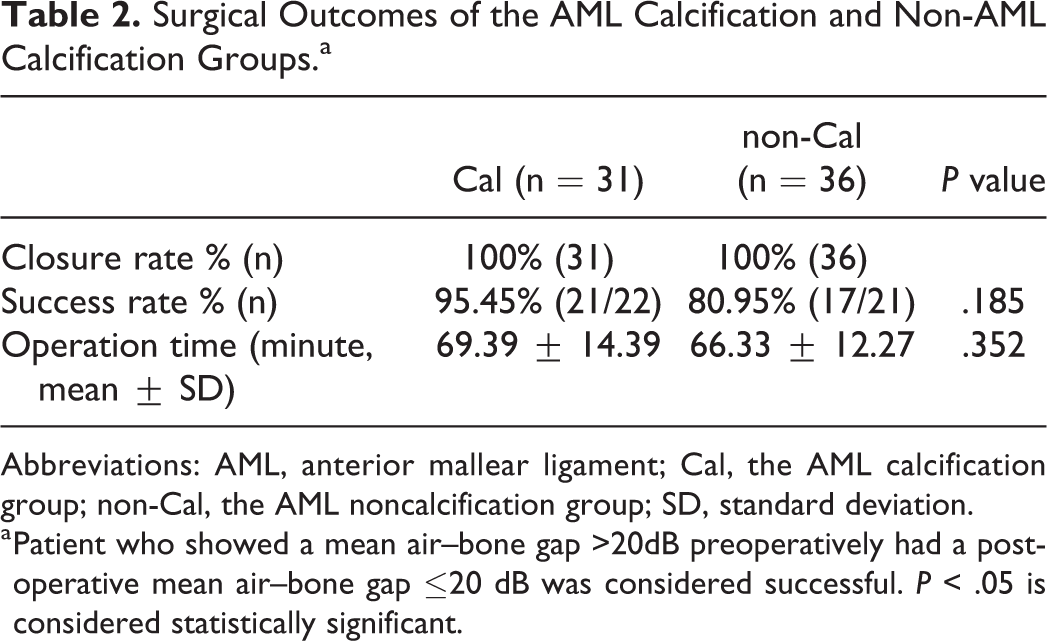
Abbreviations: AML, anterior mallear ligament; Cal, the AML calcification group; non-Cal, the AML noncalcification group; SD, standard deviation.
a Patient who showed a mean air–bone gap >20dB preoperatively had a postoperative mean air–bone gap ≤20 dB was considered successful. P < .05 is considered statistically significant.
The pre- and postoperative hearing outcomes of the Cal and non-Cal groups are shown in Table 3. Preoperatively, the Cal group had higher mean ABG (P = .022), and ABGs at 250 Hz (P = .017) and 500 Hz (P = .008), when compared with the non-Cal groups. There were no significant differences when comparing the ABGs at 1000, 2000, or 4000 Hz between the 2 groups preoperatively. No significant differences were detected between the 2 groups in mean ABG, or ABGs at 250, 500, 1000, 2000, or 4000 Hz, postoperatively. The Cal group showed higher improvement of ABGs at 250 Hz (P = .039) and 500 Hz (P = .021), when compared with the non-Cal groups. No significant differences were demonstrated between the 2 groups in improvement of mean ABG, or ABGs at 1000, 2000, or 4000 Hz. The pre- and postoperative hearing outcomes of the subgroup A and B are shown in Table 4. No significant differences were demonstrated between the 2 subgroups in preoperative, postoperative or improvement of mean ABG, or ABGs at 250, 500, 1000, 2000, or 4000 Hz.
Preoperative and 6-Month Postoperative Hearing Outcomes of the AML Calcification and Non-AML Calcification Groups.a
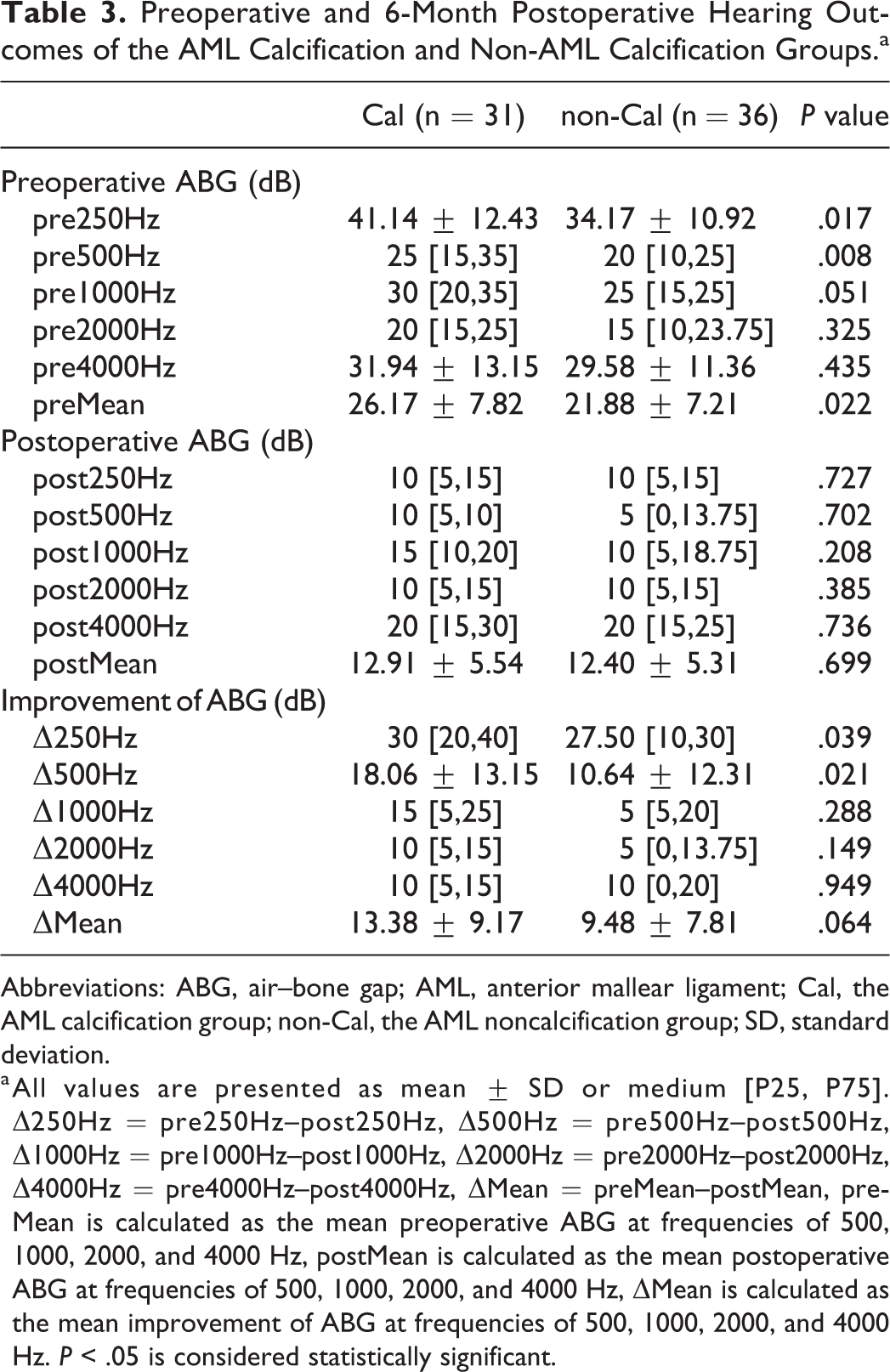
Abbreviations: ABG, air–bone gap; AML, anterior mallear ligament; Cal, the AML calcification group; non-Cal, the AML noncalcification group; SD, standard deviation.
a All values are presented as mean ± SD or medium [P25, P75]. Δ250Hz = pre250Hz–post250Hz, Δ500Hz = pre500Hz–post500Hz, Δ1000Hz = pre1000Hz–post1000Hz, Δ2000Hz = pre2000Hz–post2000Hz, Δ4000Hz = pre4000Hz–post4000Hz, ΔMean = preMean–postMean, preMean is calculated as the mean preoperative ABG at frequencies of 500, 1000, 2000, and 4000 Hz, postMean is calculated as the mean postoperative ABG at frequencies of 500, 1000, 2000, and 4000 Hz, ΔMean is calculated as the mean improvement of ABG at frequencies of 500, 1000, 2000, and 4000 Hz. P < .05 is considered statistically significant.
Preoperative and 6-Month Postoperative Hearing Outcomes of the Subgroup A and B From the Cal Group.a
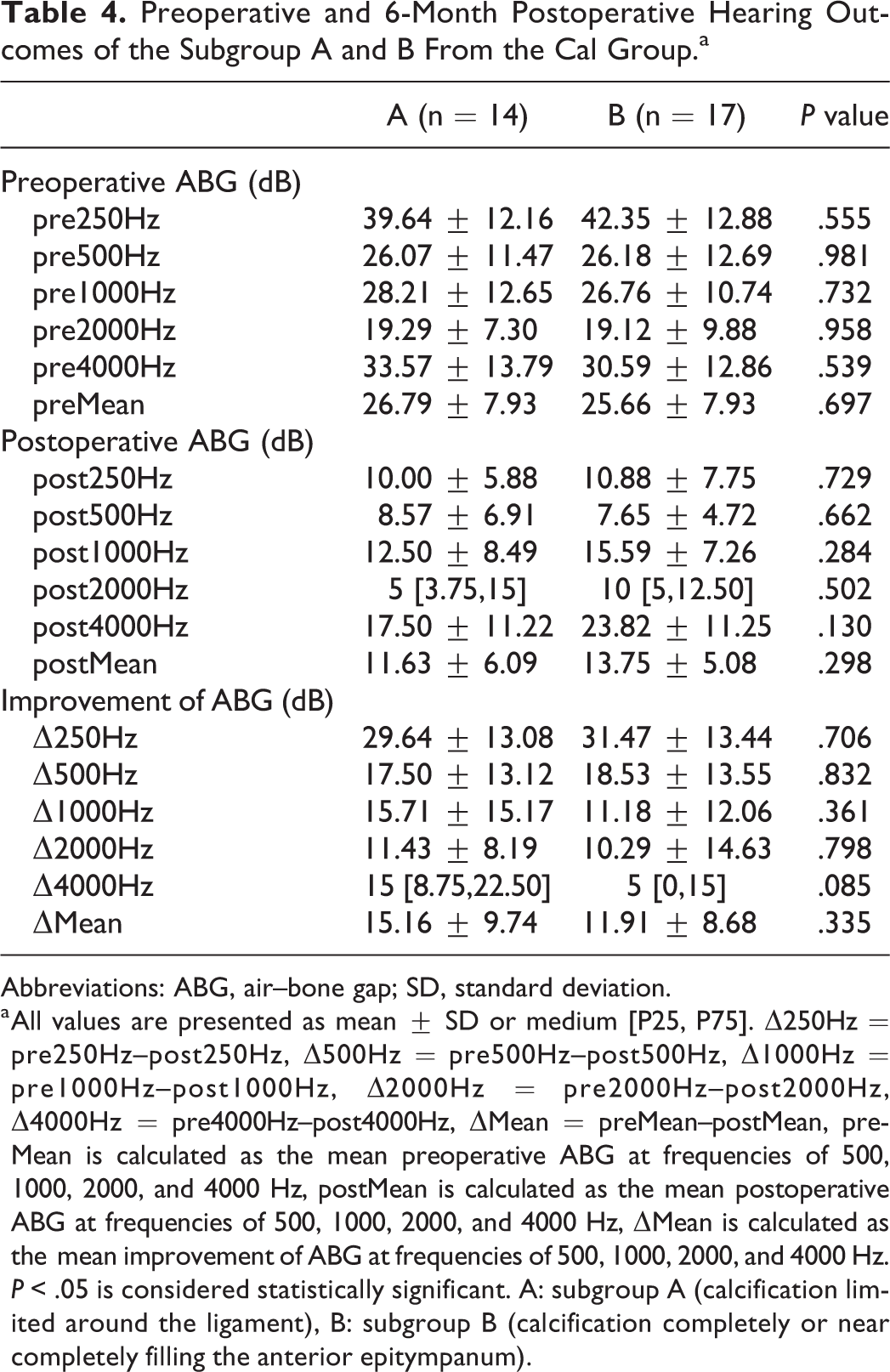
Abbreviations: ABG, air–bone gap; SD, standard deviation.
a All values are presented as mean ± SD or medium [P25, P75]. Δ250Hz = pre250Hz–post250Hz, Δ500Hz = pre500Hz–post500Hz, Δ1000Hz = pre1000Hz–post1000Hz, Δ2000Hz = pre2000Hz–post2000Hz, Δ4000Hz = pre4000Hz–post4000Hz, ΔMean = preMean–postMean, preMean is calculated as the mean preoperative ABG at frequencies of 500, 1000, 2000, and 4000 Hz, postMean is calculated as the mean postoperative ABG at frequencies of 500, 1000, 2000, and 4000 Hz, ΔMean is calculated as the mean improvement of ABG at frequencies of 500, 1000, 2000, and 4000 Hz. P < .05 is considered statistically significant. A: subgroup A (calcification limited around the ligament), B: subgroup B (calcification completely or near completely filling the anterior epitympanum).
Discussion
It is certain that chronic inflammation could consequently produce granulation, fibrosis, or calcification between the OC and its surrounding structures in the middle ear. 5 The AML laying between the anterior process of malleus and the wall of tympanic cavity is inevitable to be involved. 14 Confirmation of AML calcification is mainly by surgical exploration. However, the limited vision in microscopic ear surgery makes challenge to successfully detection of lesions in this area. Until recent years, the development of transcanal endoscopic surgical system, which can afford a wide field of vision, enables easily discovery of the calcification of AML. 15 Temporal CT scan may provide some clues for AML calcification before surgery. 6 Nevertheless, the sensitivity of image examination remains uncertain as only thick bony webs and generalized bony encasement can be visualized. Thus, preoperative audiological examination is crucial for otologists to arouse suspicion of AML lesion. In the current study, the CAL group has higher ABGs at 250 and 500 Hz, and a consequent higher mean ABG (the average ABG of 500, 1000, 2000, and 4000 Hz) than the non-CAL group. These results are partially consistent with the findings of Hideko et al’s, where the fixation of 3 ossicles produced bigger reduction of umbo and stapes velocity at low frequencies (<1 kHz) than high frequencies (>1 kHz) in human temporal bones, and the malleus head fixation had the most prominent detrimental effect. 16 In addition, they demonstrated that the mechanics of the middle ear was governed by stiffness at frequencies <1 kHz, which was different from the mechanics at high frequencies. Furthermore, Huber et al found that AML calcification induced malleus fixation could cause a 10 to 30 dB conductive hearing loss and was low-frequency dominant. 7 Severity of calcification may have different influences on movement of the OC. However, the comparison of preoperative ABGs of the 2 subgroups (representing different severity of AML calcification cases in the Cal group, Table 4) showed no statistical significance. It might indirectly reflect the importance of the AML in the movement of malleus, rather than severity of calcification. Therefore, such audiological performance can hint the possibility of AML calcification and consequent malleus fixation. However, other lesions of middle ear can’t be excluded by audiological test alone.
According to the classification of tympanoplasty proposed by Wullstein and Zollner, 11,12 tympanoplasty using ossicular replacement prosthesis is a proper treatment for improving the hearing when the OC is disconnected or eroded due to inflammation or is immobilized by fibrosis or calcification. In the former case, there is no controversy to trim the futile ossicles and reconstruct the OC with prosthesis. However, surgical treatment options exist when confronted with the fixation of OC, especially the isolated fixation of malleus. Goodhill suggests that the incus should be removed and prosthesis is needed. 17 However, Seidman et al reported that freeing the incus and malleus by laser and drill could distinctly narrow the ABG for otosclerosis cases. 13 Komune et al showed that, instead of tympanoplasty with prosthesis, the combination of atticotomy and myringoplasty was effective to achieve hearing improvement in majority of the CSOM cases with fixation of ossicles. 18 In the current study, we found that the CAL group had a comparable postoperative ABG and success rate with the non-CAL group, and the cases with AML calcification had a higher improvement of ABG at 250 and 500 Hz, under transcanal endoscopic type I tympanoplasty. What is more, the comparison of operating time and closure rate between the 2 groups showed no statistically significant difference. The undifferentiated postoperative ABG of the 2 groups infers that complete removal of AML calcification recovers the mobility of the malleus and restores the physiological function of OC to a near normal level. Functionally, prosthesis can’t be comparable with autologous OC in anatomic form and impedance matching. 19 Therefore, remobilizing the malleus by eliminating the AML calcification and retain the OC may provide better recovery of impedance matching and sound transmission compared with prosthesis implantation. In addition, the management of calcificated AML didn’t have detrimental effect on perforation closure or operation time. Thus, for both practical and ethical consideration, we didn’t make comparison between type I and type II tympanoplasty for such type of patients. Either pure myringoplasty with neglecting the AML calcification or radical prosthesis implantation could lead to unsatisfactory improvement of hearing after surgery.
Our study has several limitations. (1) The current study merely made comparison of CSOM cases with functional OC and those with AML calcification, herein the conclusion can’t be extended to fixation of OC caused by other reasons. (2) The sample size was relatively small. A prospective study with large sample size or multicenter is recommended in the future. (3) A relatively longer follow-up period might be needed to assess the stability of the hearing outcomes.
In conclusion, CSOM with AML calcification has a higher ABG at low frequencies than those with intact and mobile OC. And they show comparable hearing outcomes and tympanic perforation healing under transcanal endoscopic type I tympanoplasty, when the calcification is eliminated. Herein, we suggest that transcanal endoscopic type I tympanoplasty is a recommend option for surgical treatment of CSOM accompanied by AML calcification, with thorough preoperative audiological examination and careful intraoperative tympanic cavity exploration.
Footnotes
Authors’ Note
C.W., X.C. and Y.H. were the co-first authors. F.Y. and X.W. were the co-corresponding authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Zhejiang Provincial Natural Science Foundation of China (No. LY20H130002) and Wenzhou Science and Technology Bureau (No. Y20180090, Y2020027 and Y2020333).