
Abstract
It is rare for intraductal papilloma, a benign papillary tumor, to occur in the salivary glands. To our knowledge, intraductal papilloma occurring in the minor salivary glands of the larynx has not been reported. In this report, we describe a case of intraductal papilloma that occurred in the minor salivary glands of the larynx. A woman in her 30s presented with hoarseness and dyspnea since a year. Fiber-optic laryngoscopy revealed a submucosal tumor involving the left aryepiglottic fold and the left false vocal fold. Computed tomography and magnetic resonance imaging revealed a 17 × 15 × 10 mm3 mass with homogenous isodensity, with regular, well-defined margins located on the left aryepiglottic fold and the left false vocal fold. Surgical resection was performed, and subsequently a diagnosis of intraductal papilloma was made by pathologic evaluation. During the follow-up period of over 3 years, the lesion has not recurred. In conclusion, intraductal papilloma of the minor salivary glands should be considered in the differential diagnosis of laryngeal submucosal tumors.
Introduction
Ductal papillomas include intraductal papilloma, inverted ductal papilloma, and sialadenoma papilliferum. Among these, intraductal papilloma in the salivary gland is a rare benign papillary tumor. 1 On the basis of histogenesis, intraductal papilloma is considered to originate from the salivary gland duct epithelium.2,3 These papillomas more frequently involve the minor salivary gland than the major salivary gland. 4 Of the minor salivary glands, those of the lips, buccal mucosa, soft palate, hard palate, and ventral tongue have been reported to be involved.2,5-9 However, there has been no reported case of intraductal papilloma arising from the larynx. Herein, we report a case of the intraductal papilloma arising from the minor salivary glands in the larynx.
Case Report
A woman in her 30s was referred to our department from a previous clinic for the evaluation of a tumor in the larynx. The patient reported having hoarseness and dyspnea since a year. Fiber-optic laryngoscopy revealed a submucosal and rounded tumor involving the left aryepiglottic fold and the left false vocal fold (Figure 1). The superficial mucosa of the tumor was intact. The shape of the true vocal folds was normal and both vocal folds were mobile. Nevertheless, incomplete glottic closure was seen. In her neck, there were no palpable masses. The results of the laboratory tests were within normal limits.

Fiber-optic laryngoscopy shows the left aryepiglottic fold and the left false vocal fold swollen by the submucosal intraductal papilloma.
Computed tomography (CT) revealed a 17 × 10 mm2 homogenous, isodense, and regular mass located on the left aryepiglottic fold and the left false vocal fold. The lesion was contained within the laryngeal framework. Cartilage destruction was not evident.
Magnetic resonance imaging (MRI) revealed a mass with a similar shape as observed on CT. T1- and T2-weighted images showed an isointense tumor, whereas short T1 inversion recovery (STIR) images showed a 17 × 15 × 10 mm3 high-intensity unicystic, regular mass with well-defined margins located on the left aryepiglottic fold and the left false vocal fold (Figure 2).
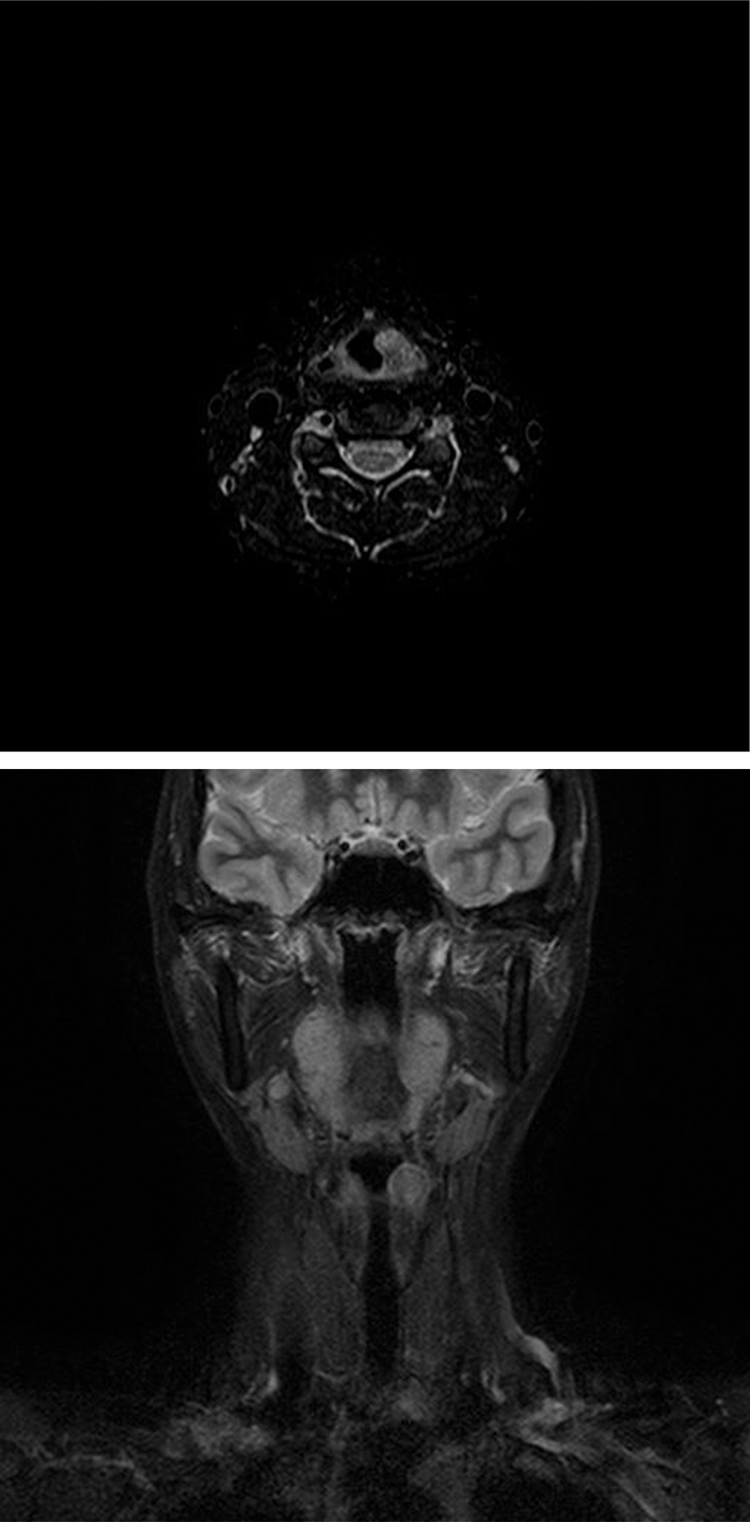
Axial and coronal short T1 inversion recovery images of MRI showing a 17 × 15 × 10 mm3 high-intensity unicystic, regular mass with well-defined margins located on the left aryepiglottic fold and the left false vocal fold. MRI indicates magnetic resonance imaging.
Using the endoscopic procedure, a biopsy sample was obtained from the laryngeal mass. Microscopic examination revealed papillary proliferations with fibrovascular cores and minor salivary glands. The tumor was suspected of being a benign papilloma. Under general anesthesia, transoral video surgery (TOVS) was performed with a WEERDA Distending Video Operating Laryngoscope (Karl Storz). The tumor was completely resected in 2 parts using the tumor splitting approach. There were no complications associated with the surgical procedure.
Following the surgical procedure, the patient experienced a satisfactory course of recovery, and the patient’s symptoms improved. The patient has undergone regular postoperative follow-up as an outpatient once a month for the first 6 months, followed by twice a year for 3.5 years. During the follow-up, the lesion did not recur.
Histologically, the microscopic section showed a submucosal tumor, measuring a maximum of 13 × 10 mm2, located within the duct of the minor salivary gland (Figure 3). The tumor cells were growing into the lumen of the submucosal cystic space. A higher power view of the tumor showed that the papillary tumor was composed of tall columnar epithelial cells with squamous metaplasia and fibrovascular cores. The cyst was lined by cuboidal and goblet cells. No tumor extension beyond the cyst wall was seen microscopically. The tumor cells showed no evidence of malignancy. A diagnosis of intraductal papilloma was made.
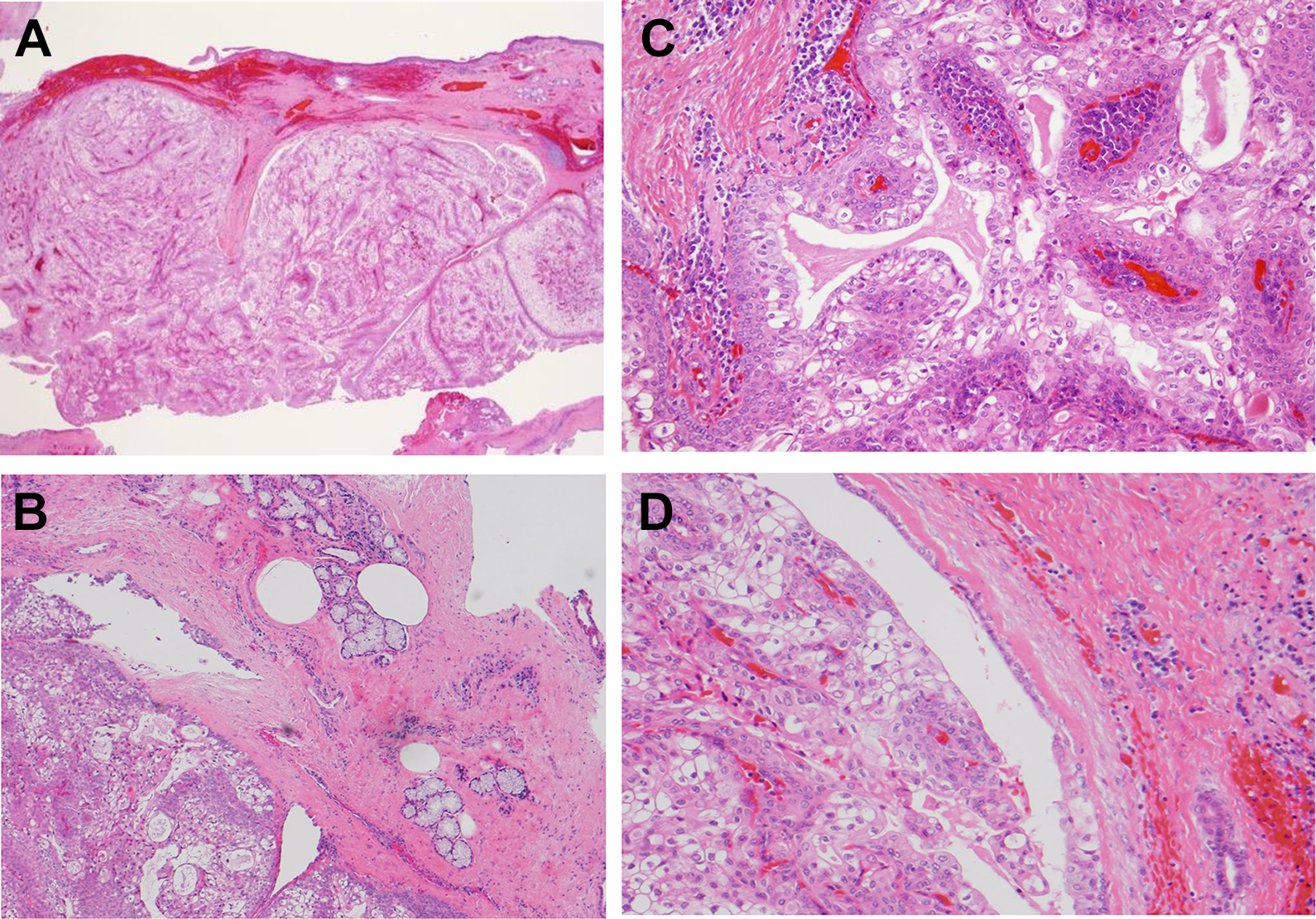
A, Papillary growth of tumor cells in the submucosal cystic spaces (hematoxylin–eosin, ×20). B, Minor salivary gland lobule proximal to the tumor (hematoxylin–eosin, ×40). C, Papillary structure with fibrovascular cores (hematoxylin–eosin, ×200). D, The cyst lined by cuboidal cells and goblet cells (hematoxylin–eosin, ×100).
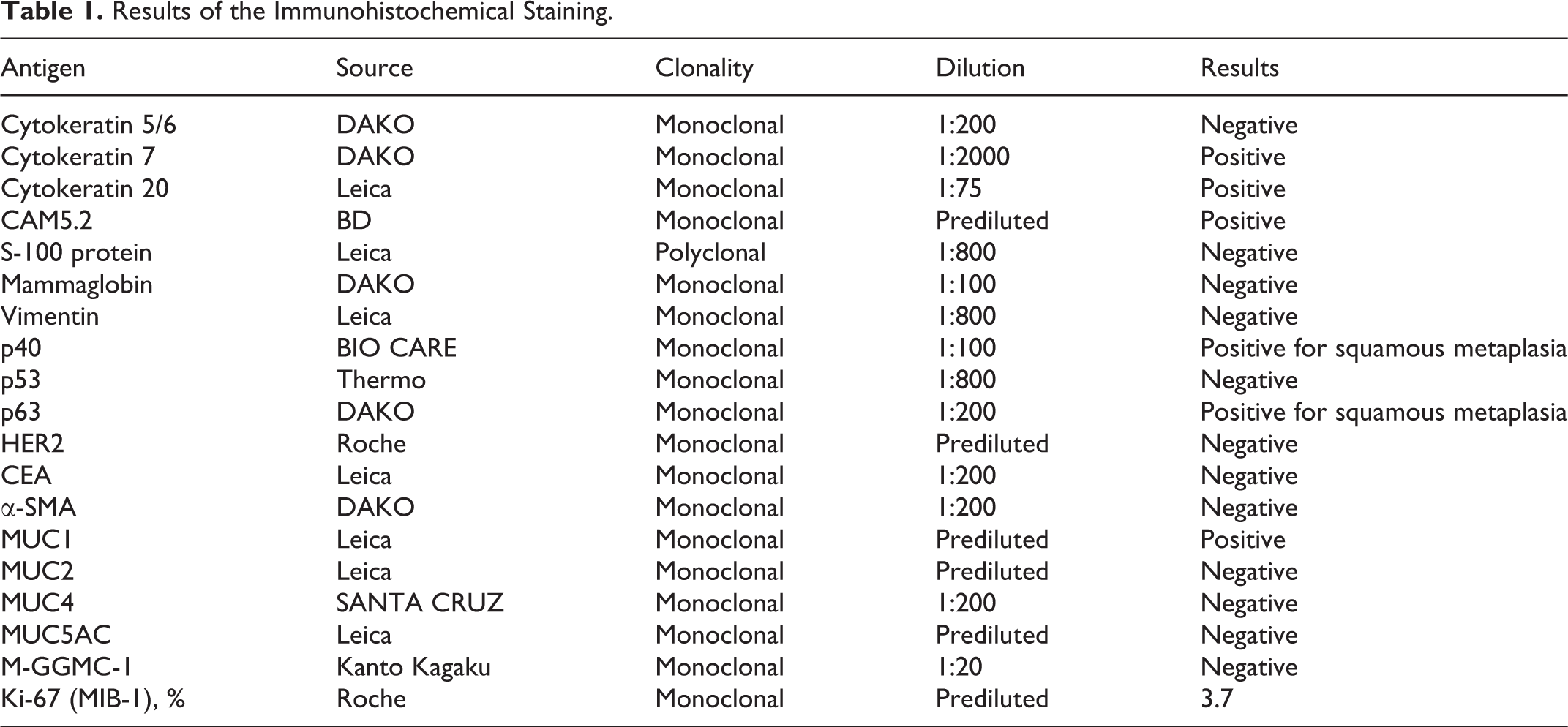
Sections from the paraffin-embedded tissue were examined immunohistochemically, using the primary antibodies listed in Table 1. The percentage of Ki-67-positive cells was recorded as the Ki-67 labeling index. The results of the immunohistochemical studies are summarized in Table 1. In this case, the tumor cells expressed cytokeratin (7, 20), CAM5.2, p63, and MUC1. The cells showed no immunoreactivity to cytokeratin (5 of 6), S100 protein, mammaglobin, vimentin, p53, HER2, CEA, α-SMA, MUC2, MUC4, MUC5AC, and M-GGMC-1.
Results of the Immunohistochemical Staining.
Discussion
We report a case of the intraductal papilloma arising from the minor salivary glands of larynx. Histopathologically, intraductal papilloma is recognized as a luminal papillary proliferation of the duct epithelium that arises from a segment of the interlobular or excretory duct and causes unicystic dilatation. 10 In this case, the microscopic section did not show a typical unicystic tumor because the tumor was resected in 2 parts. However, CT and MRI that were performed before biopsy showed a homogeneous mass with isodensity and regular, well-defined margins. In addition, fiber-optic laryngoscopy showed that the mucosa of the larynx was intact. It has been reported that the cyst wall in intraductal papilloma is lined by a layer of cuboidal or columnar cells, as found in our case.4 Therefore, a diagnosis of intraductal papilloma was made.
The literature shows that the main differential diagnoses for intraductal papilloma of the larynx include benign laryngeal tumors (neurofibroma, lipoma, adenoma, osteoma, chondroma, paraganglioma, schwannoma), non-neoplastic lesions (laryngocele, ectopic thyroglossal duct cyst, laryngeal cyst), and malignant neoplasms. However, it is most important to distinguish intraductal papillomas from malignant and precancerous neoplasms, such as mammary analogue secretory carcinoma (MASC), mucoepidermoid carcinoma, and intraductal papillary mucinous neoplasm (IPMN).
It has been reported that MASC is immunohistochemically positive for S-100 protein, mammaglobin, and vimentin. 11 In our case, the immunohistochemical analysis did not show immunoreactivity for vimentin, mammaglobin, and S-100. Mucoepidermoid carcinoma shows a multicystic, multinodular, and infiltrative growth pattern compared to that shown by intraductal papilloma. 1 It has been reported that MUC1 and MUC5AC are more frequently expressed in salivary gland mucoepidermoid carcinoma than in normal salivary glands. 12 However, previous studies have shown conflicting results of MUC1 expression in salivary gland mucoepidermoid carcinoma. 13 In our case, these histopathological findings were not identified and the immunohistochemical analysis did not show immunoreactivity for MUC5AC. Additionally, the Ki-67 labeling index of the tumor was low (3.7%). Intraductal papillary mucinous neoplasm of the minor salivary gland was proposed as a new entity. 14 It has been reported that the typical IPMN expresses MUC5AC, shows architectural atypia, and has no recognizable basal cell layer on immunohistochemical analysis. 15 However, the typical pathological findings of IPMN were not observed in our case. Therefore, we excluded these malignant and precancerous neoplasms from the diagnosis.
The possible methods of preoperative evaluation of this lesion were biopsy, CT, and MRI. In this case, the biopsy sample was obtained using the endoscopic procedure because the submucosal tumor was located in the larynx. The microscopic examination of the biopsy specimen to reveal that the mass was a benign papilloma. Although a confirmative diagnosis of intraductal papilloma should be made on the basis of histopathological findings of the surgical specimen, biopsy may be useful for the exclusion of malignancy and preoperative clinicopathological diagnosis of papillary tumor of the larynx.
According to a previous report, CT and MRI are helpful for evaluating the location, internal features, and behavior of the tumor 16 ; however, it is difficult to make a diagnosis of this tumor preoperatively through radiologic studies because intraductal papillomas are very rare and small. 17 In previously reported cases of intraductal papilloma arising from major salivary glands, CT showed both cystic18,19 and solid features. 20 Furthermore, MRI showed high intensity in T1-weighted images, and various levels of intensity in T2-weighted images of the lesion.16,19 In our case, the CT and MRI findings were not the same. Our CT images showed a solid tumor, while the MRI images showed both iso intensity in T1- and T2-weighted images. In the CT and MRI images, STIR images showed that the margins of the tumor were well defined, which was helpful for making the diagnosis. Therefore, STIR images may be especially useful for locating the tumor.
As no case of intraductal papilloma of the larynx has been reported previously, it is difficult to discuss the best treatment for this case. Mostly, intraductal papilloma is benign; however, cases of malignant intraductal papilloma have also been reported.3,19 Confirmative diagnosis of intraductal papilloma is mostly made on the basis of the histopathologic findings of the surgical specimen, even if a biopsy is performed. Hence, surgical resection can be the first-line treatment for intraductal papilloma of the larynx. It has been reported that the treatments for pleomorphic adenoma arising from the minor salivary glands in the larynx include pharyngotomy or transoral surgery under microdirect laryngoscopy, depending on its size and location. 21 This treatment policy could have been applied in the present case. Because intraductal papilloma is a benign tumor, a less invasive surgery should be performed, as far as possible. Transoral surgery is a minimally invasive approach that requires no skin incision and limits the extent of tissue dissection, disruption of speech and swallowing muscles, blood loss, damage to the major neurovascular structures, and injury to normal tissue. 20 In our case, we performed TOVS and there were no complications associated with the surgical procedure.
Only 4 cases of this tumor with adequate postoperative follow-up (2-2.5 years2,3,7,22) have been reported. In all of them, there was no evidence of recurrence. Our patient has been followed up for 3.5 years, the longest period, and has undergone regular follow-up as an outpatient once a month for 6 months and twice a year for 3.5 years, until the time of this study. During the follow-up, endoscopic examination and CT showed no recurrence of the tumor. However, as a risk of recurrence of this tumor remains, long-term follow-up will be needed.
Conclusion
In summary, intraductal papilloma of the minor salivary glands should be considered as a differential diagnosis of laryngeal submucosal tumors. Although it is difficult to make a preoperative diagnosis of such a tumor by radiologic studies, STIR images of MRI may be useful in making a diagnosis. Surgical resection can be the first-line treatment for such a lesion; a less invasive surgical technique, such as transoral surgery, should be adopted. As there is a risk of recurrence, long-term follow-up is necessary.
Footnotes
Authors’ Note
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Acknowledgment
The authors thank Mr. Brent Bell for having reviewed this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.