
Abstract
Objectives:
The aim of this study was to use immunohistochemistry to differentiate solid papillary carcinoma in situ from intraductal papilloma with usual ductal hyperplasia (IPUDH). Three types of high-molecular-weight cytokeratins (CKs) – CK5/6, CK14, and CK34betaE12 – were targeted.
Methods:
We studied 17 patients with solid papillary carcinoma in situ and 18 patients with IPUDH diagnosed by at least two pathologists. Immunohistochemical analyses used antibodies to CK5/6, CK14, and CK34betaE12 to make the differential diagnosis of solid papillary carcinoma in situ versus IPUDH. Immunohistochemical staining was scored as 0–5 using Allred score.
Results:
Immunohistochemistry with CK5/6 and CK14 antibodies produced scores of 0–3 in all patients with solid papillary carcinoma in situ and 2–5 in all patients with IPUDH. Immunohistochemical staining with CK34betaE12 antibody produced scores of 1–3 in all patients with solid papillary carcinoma and 3–5 in all patients with IPUDH. In tissues from patients with IPUDH, significantly more cells were stained with CK34betaE12 than CK5/6 (p < 0.05) or CK14 (p < 0.05).
Conclusion:
The immunoreactivity of CK5/6, CK14, and CK34betaE12 antibodies was useful to differentiate solid papillary carcinoma in situ from IPUDH. CK34betaE12 is especially useful for distinguishing solid papillary carcinoma from IPUDH.
Keywords
Introduction
Solid papillary carcinoma (SPC) in situ is a noninvasive ductal carcinoma with neuroendocrine differentiation that was first characterized by Cross et al. 1 in 1985. More detailed reports were later published by Tsang and Chan 2 and Kawasaki et al. 3 The incidence of SPC in situ is accepted as 6.8%–23.3%1,3 of all cases of ductal carcinoma in situ (DCIS). Many patients are elderly, 2 and bloody nipple discharge is a common symptom. 3
Histopathologically, SPC in situ shows a solid growth pattern that includes a fibrovascular core in the dilated duct.1,2 The tumor cells are polygonal, oval, or spindle shaped with well-defined cell borders1,2 and granular acidophilic cytoplasm. 2 The extracellular mucin in the microglandular spaces and septa are stained by periodic acid-Schiff, mucicarmine, and Alcian blue, which indicates that the mucin is of epithelial origin. 2 SPC in situ is a malignant tumor that is difficult to differentiate from benign lesions such as epitheliosis, intraductal epithelial hyperplasia, and florid hyperplasia, because proliferation of duct cells of those benign lesions resembles those of SPC in situ.1,2,4–6
The breast duct comprises two types of cells: duct and myoepithelial cells. However, some cells cannot be classified into either cell type. These cells are called stem cells/ progenitor-like cells and have the potential to differentiate into either duct cells or myoepithelial cells. 7 Many properties, markers, or cell populations are used to identify breast stem cells including cytokeratin 5 (CK5), 7 p21, 8 Musashi 1, 8 CK19, 9 alfa6 integrin (CD49f), 10 side population cells,8,11 label-retaining cells, 8 epithelial specific antigen-positive/Muc1-negative cells,9,10 and epithelial membrane antigen-positive/common acute lymphoblastic leukemia antigen-negative cells. 11
SPC in situ is a specific type of DCIS and should be differentiated from intraductal papilloma with usual ductal hyperplasia (IPUDH). CK5/6 and CK34betaE12 include CK5 as progenitor cell marker. CK14 is a component of one tetramer that is composed of two CK5s and two CK14s. 12 In this study, we examined whether staining with antibodies of CK5/6, CK34betaE12, and CK14–related progenitor cell marker (CK5) could differentiate between SPC in situ and IPUDH.
Materials and methods
Patients and tumors
This study included 18 consecutive patients with SPC in situ from the 211 DCIS patients (18/211, 8.5%) who had a tumor removed surgically at St. Marianna University Hospital (Kawasaki, Japan) from April 2003 to March 2009. One patient was excluded because the specimen obtained provided insufficient material for immunohistochemical staining. The area of usual ductal hyperplasia from samples obtained from 18 patients with IPUDH whose tumor was also removed surgically during the same period was used as a control.
The patients with SPC in situ who were selected to participate in this study showed some or all of the histological features of SPC in situ as described by Cross et al. 1 and Tsang and Chan. 2 All samples were positive for either chromogranin A or synaptophysin, or showed positive Grimelius staining.
Immunohistochemical analysis
Immunohistochemical staining of paraffin-embedded tissue was performed using antibodies to the following: chromogranin A, synaptophysin, CK5/6, CK14, and CK34betaE12 (which recognizes CKs 1, 5, 10, and 14).
Table 1 shows a list of the sources and dilutions of these antibodies. Immunoreactions were visualized using the avidin–biotinylated peroxidase complex method.
Sources and dilutions of antibodies to chromogranin A, synaptophysin, CK5/6, CK14, and CK34betaE12.

Scoring of sections
Using the 0–5 proportional scoring method of Allred et al., 13 we estimated the percentages of immunohistochemically stained tumor-like cells in hyperplastic lesions of duct cells, excluding myoepithelial cells. A score of 0 corresponded to 0%; 1, <1%; 2, 1% to <10%; 3, 10% to <33.3%; 4, 33.3% to <66.7%; and 5, ⩾66.7%.
Cutoff score
The cutoff score was defined as the boundary score based on which we determined a specimen to be negative or positive for a marker. In other words, if we set 2 as the cutoff score, we determined scores 0, 1, and 2 to indicate negativity and scores 3, 4, and 5 to indicate positivity.
The final objective of this pilot study was to determine whether there was a difference between IPUDH and DCIS in the rate of positivity for each of the three antibodies (CK5/6, CK14, and CK34betaE12).
Statistical analysis
The statistical significance of differences was analyzed using Fisher’s exact probability test when indicated. p-values less than 0.05 were considered significant.
Ethical approval
The study was approved by the ethics committee of St. Marianna University (approval no. 1524).
Results
Clinical data
At St. Marianna University Hospital, the incidence of SPC in situ was 8.5% (18/211) of all DCIS cases. The average age of the 17 patients with SPC in situ was 60 (range: 25–87) years and 18 patients with IPUDH was 47.4 (range: 24–76) years. SPC in situ with the chief complaint of bloody nipple discharge was found in 64.7% (11/17) of these patients. The positivity rates for neuroendocrine markers were as follows: synaptophysin, 94.1% (16/17); chromogranin A, 100% (17/17); and Grimelius staining, 88.2% (15/17). The positivity rates for hormone receptors were 100% (17/17) for the estrogen receptor (ER) and 94.1% (16/17) for the progesterone receptor.
Immunohistochemistry (CK5/6, CK34betaE12, and CK14)
We immunohistochemically stained surgical specimens from 17 patients with SPC in situ (Figure 1(a) and (b)) and 18 patients with IPUDH (Figure 2(a)) using antibodies to CK5/6 (Figures 1(c) and 2(b)), CK14 (Figures 1(d) and 2(c)), and CK34betaE12 (Figures 1(e) and 2(d)), and compared the staining scores for each marker.

Solid papillary carcinoma (SPC) in situ. (a) Histopathologically, SPC in situ shows solid, expansive growth. (b) A higher magnification of an SPC in situ lesion shows solid growth and a fibrovascular core. Tumor cells are polygonal and oval, and have well-defined cell borders and granular acidophilic cytoplasm. (c)–(e) Sample obtained from patient 12 showing positive immunostaining indicative of SPC in situ: (c) CK5/6 (score 1), (d) CK14 (score 1), and (e) CK34betaE12 (score 1).
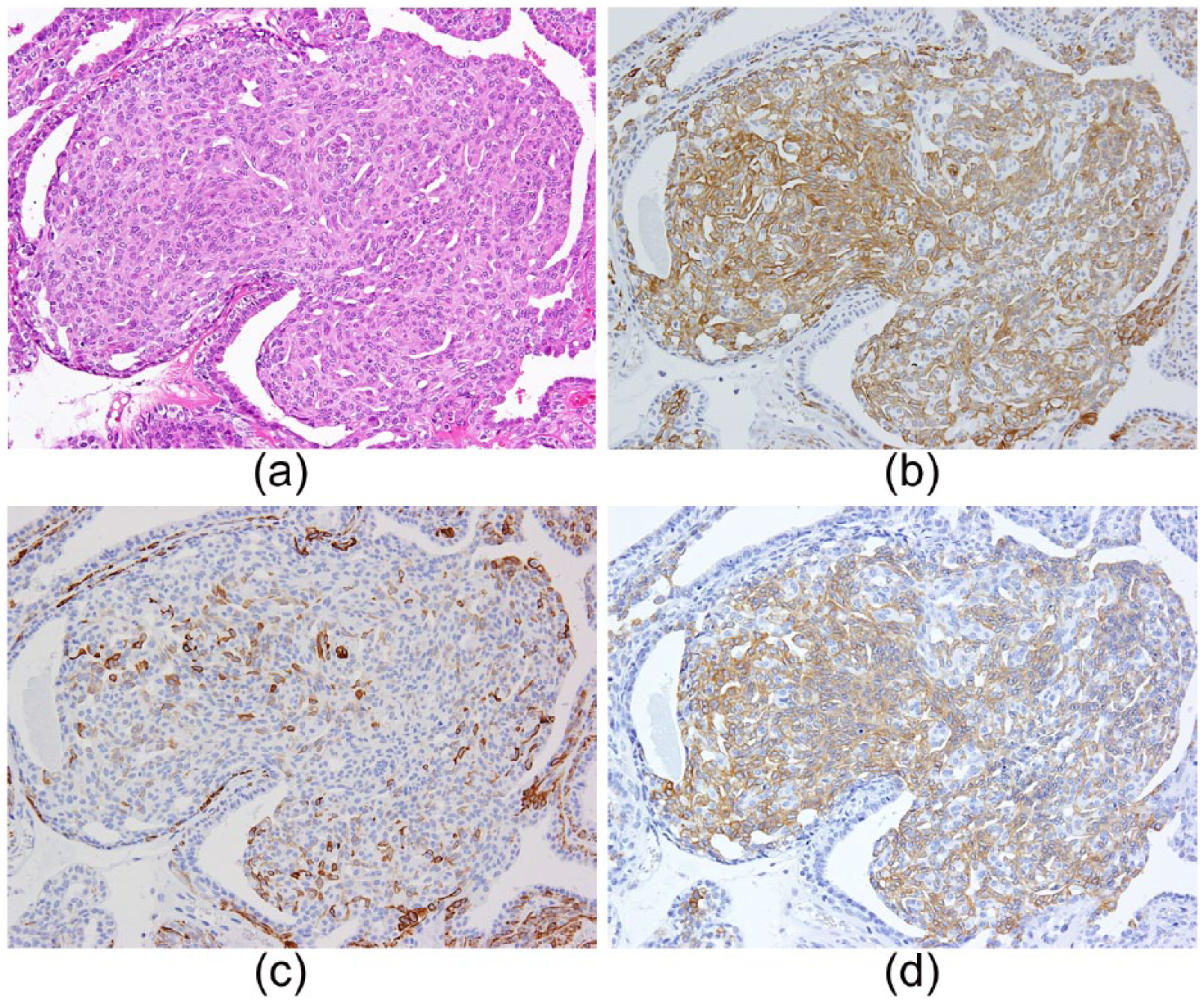
Intraductal papilloma with usual ductal hyperplasia (IPUDH). (a) Histologically, IPUDH shows papillary growth with usual ductal hyperplasia. (b)–(d) Sample obtained from patient 25 showing positive immunostaining indicative of IPUDH: (b) CK5/6 (score 5), (c) CK14 (score 3), and (d) CK34betaE12 (score 4).
For CK5/6, none of the patients with SPC in situ had a score of 4 or 5; three had a score of 0; eight a score of 1; five a score of 2; and five a score of 3 (Table 2). For the patients with IPUDH, none had a score of 0 or 1; seven had a score of 2; four a score of 3; six a score of 4; and one a score of 5 (Table 2).
Diagnosis and immunochemical staining scores based on immunohistochemical staining for CK5/6, CK14, and CK34betaE12.
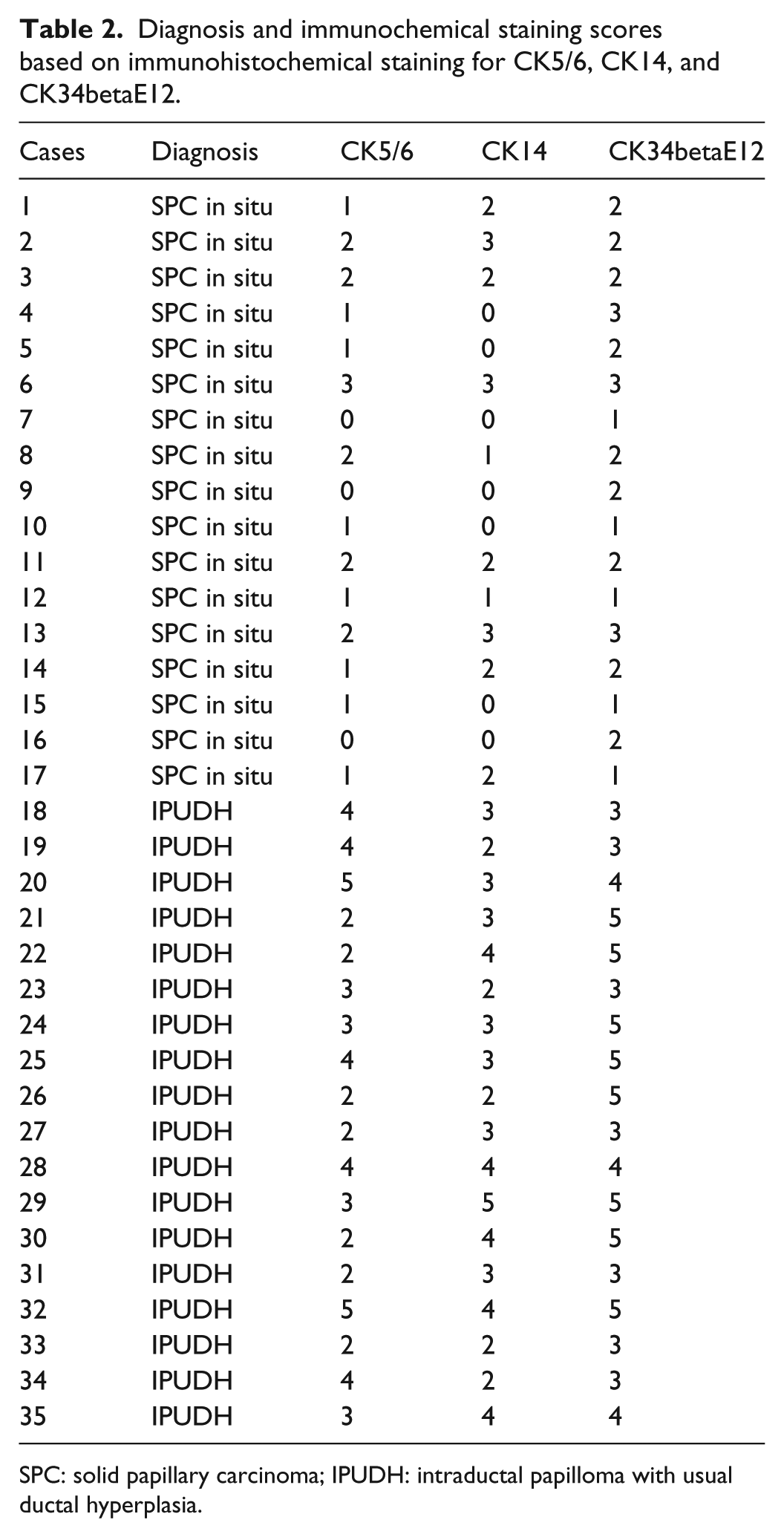
SPC: solid papillary carcinoma; IPUDH: intraductal papilloma with usual ductal hyperplasia.
For CK14, none of the patients with SPC in situ had a score of 4 or 5; seven had a score of 0; two a score of 1; five a score of 2; and three a score of 3 (Table 2). For the patients with IPUDH, none had a score of 0 or 1; five had a score of 2; seven a score of 3; five a score of 4; and one a score of 5 (Table 2).
For CK34betaE12, none of the patients with SPC in situ had a score of 0, 4, or 5; five had a score of 1; nine a score of 2; and three a score of 3 (Table 2). For the patients with IPUDH, none had a score of 0, 1, or 2; seven had a score of 3; three a score of 4; and eight a score of 5 (Table 2).
Sensitivity and specificity using a cutoff score of 2
At a cutoff score of 2, 10% of all tumor cells counted were positive for immunoreactivity (Table 3). For CK5/6 immunoreactivity, this gave a sensitivity of 69.6% and a specificity of 91.7%. For CK14 immunoreactivity, the sensitivity was 73.3% and the specificity was 81.3%. For CK34betaE12 immunoreactivity, the sensitivity was 87.5% and the specificity was 84.2%.
Sensitivities and specificities of staining for CK5/6, CK14, and CK34betaE12 (cutoff scores of 1, 2, and 3).

Comparison of immunoreactivity between patient groups
A comparison of the immunoreactivities to CK5/6, CK14, and CK34betaE12 between the 17 SPC in situ patients and the 18 IPUDH patients revealed significant differences (p < 0.05) distinguishing SPC in situ from IPUDH, as determined by Fisher’s exact probability test using cutoff scores of 2 (see Tables 3 and 4). Comparison of immunoreactivities to CK5/6, CK14, and CK34betaE12 in the 17 SPC in situ patients showed no significant differences between CK5/6 and CK14, CK5/6 and CK34betaE12, or CK14 and CK34betaE12 (Figure 3). Comparison of the immunoreactivities to CK5/6, CK14, and CK34betaE12 in 18 IPUDH patients revealed significant differences between CK5/6 and CK34betaE12 and between CK14 and CK34betaE12, but not between CK5/6 and CK14 (Figure 4).
Immunoreactivity to CK34betaE12 in tissues from patients with SPC in situ or IPUDH and the results of the Fisher’s exact probability test for a cutoff score of 2.

SPC: solid papillary carcinoma; IPUDH: intraductal papilloma with usual ductal hyperplasia.

Comparison of immunoreactivities for high-molecular-weight cytokeratins (HMWCKs) in SPC in situ: comparison of immunoreactivities to CK5/6, CK14, and CK34betaE12 in the 17 SPC in situ patients showed no significant differences between CK5/6 and CK14, CK5/6 and CK34betaE12, or CK14 and CK34betaE12.

Comparison of immunoreactivities for high-molecular-weight cytokeratins (HMWCKs) in IPUDH: comparison of the immunoreactivities to CK5/6, CK14, and CK34betaE12 in 18 IPUDH patients revealed significant differences between CK5/6 and CK34betaE12 and between CK14 and CK34betaE12, but no significant difference between CK5/6 and CK14.
Discussion
It has been reported that CK5/6 is a more useful antibody than CK34betaE12 for differentiating DCIS from intraductal papilloma. 14 In this study, CK5/6, CK14, and CK34betaE12 showed similar immunohistochemical staining patterns. We observed no significant differences between tissues from patients with IPUDH and SPC in situ in the rates of immunoreactivity of antibodies to CK5/6, CK14, and CK34betaE12 (Table 4), although these antibodies are considered to be useful for differentiating between IPUDH and SPC in situ.
A total of 20 members of the human CK family have been defined on the basis of their molecular weights, which range from about 39 to 68 Kd.12,15 Of which, 16 CKs (1–8, 10, 11, and 14–19) have been immunohistochemically or biochemically identified in normal or malignant breast epithelial cells.12,15,16 According to Steinert and Roop, 15 CKs can be classified into acidic keratins (type I) and neutral-basic keratins (type II). Most CKs are tetramers comprising two type-I keratins and two type-II keratins, for example, one tetramer that is composed of two CK5s and two CK14s. 16 CK34betaE12 is an antibody that recognizes CKs 1, 5, 10, and 14.12,17 Theoretically, antibodies to CK5/6 and CK14 should show similar immunohistochemical staining patterns to CK34betaE12.
Böecker and colleagues18,19 reported that a progenitor cell marker stains weakly positive around tumor cells in DCIS but stains diffusely positive in usual ductal hyperplasia. Antibodies to CK5,7,18 CK5/6,6,14,20–22 CK14,6,20,22 and CK34betaE126,14,21–23 recognize these progenitor cell markers. CK5/6, CK14, and CK34betaE12 stain proliferative cells diffusely (mosaic pattern) in ductal hyperplasia and duct papillomatosis. 17 The rate of positive staining of tumor cells by CK34betaE12 is 60%–100% in ductal hyperplasia.14,24,25 CK14 has been reported to stain positively >95% of cells in tissue from IPUDH patients.21,26 Several studies have reported that CK34betaE12 stains positively 0%–20% of tumor cells in tissue from DCIS patients.24,25,27 However, another study reported that 40%–100% of tumor cells stain positively for CK34betaE12 in 10% of patients with DCIS. 25
We diagnosed SPC in situ and IPUDH histopathologically using the conventional criteria, and we calculated the sensitivities and specificities of staining with antibodies to CK5/6, CK14, and CK34betaE12 in determining the optimum cutoff scores. At a cutoff score of 1, the sensitivities of these antibodies were high, but their specificities were insufficient. At a cutoff score of 3, their specificities were as high as 100% but their sensitivities were low. At a cutoff score of 2, we considered that the sensitivities and specificities were sufficiently high and were useful for differentiating between SPC in situ and IPUDH (10% of cells). We also used Allred’s proportion scoring and found that a staining rate of 1% for all tumor cells indicated SPC in situ and a staining rate of 33.3% for all tumor cells indicated IPUDH.
The cutoff scores for CK5/6 and CK14 immunoreactivities vary between previous reports. One study reported on the validation and differentiation of DCIS from benign proliferative lesions at a cutoff score of 50%. 14 Another study by Moriya et al. 6 showed “hot” nodules in a mosaic pattern at a cutoff score of 10% for differentiating DCIS from usual ductal hyperplasia. A study by Moritani et al. 23 using CK34betaE12 showed significant differences between intraductal papillary carcinomas including SPC in situ and IPUDH. We think that the reason of slightly immunopositive for CK5/6, CK14, and CK34betaE12 in some SPCs may be including intraductal papilloma components. Or, some SPCs may be occurred by stem/progenitor cells in intraductal papilloma.
In this study, CK34betaE12 stained significantly more cells than did antibodies to CK5/6 (p < 0.05) and CK14 (p < 0.05) in tissue from IPUDH patients. Tan et al. 21 have reported no significant differences in positive-staining percentages between CK5/CK6 and CK34betaE12 for papilloma. The difference in percentages between our study and that of Tan et al. may relate to the differences in the disease studied, that is, Tan et al. focused on papillomas and papillary DCISs, while we focused on IPUDHs and only SPCs.
Antibody to 34betaE12 recognizes CKs 1, 5, 10, and 14. We found significant differences in staining between CK34betaE12 and CK5 or CK14. This suggests that CK1 and 10 immunopositivity may be important in diagnosing IPUDH. After searching the literature, we found no reports of IPUDH staining for CKs 1 and 10 that might explain the significant differences detected (i.e. that CK34betaE12 immunohistochemistry was useful for identifying IPUDH). However, squamous carcinoma cells are immunopositive for CKs 1 and 10.28–30 It is possible that squamous metaplasia occurring with IPUDH causes the cells to be immunopositive for CK34betaE12.
SPC in situ as studied here and spindle cell DCIS as reported by Farshid et al. 5 are special types of DCIS, and the stainability of high-molecular-weight CKs (HMWCKs) is similar in these diseases to that in usual DCIS. In proliferative lesions of the breast, negative staining for CKs indicates DCIS. We conclude that identification of HMWCKs may be useful in the diagnosis of all types of DCIS including special types.
Our study had some limitations. First, the number of cases was limited and we analyzed only three HMWCKs. Second, age of these two groups (SPCs and IPUDHs) was not matched. However, this study was considered a pilot study. Therefore, further study of additional cases and HMWCKs is needed.
Conclusion
The immunohistochemistry of HMWCKs (CK5/6, CK14, and CK34betaE12) usually yields negative results in SPC in situ, similar to the findings for usual DCIS. We observed significant differences using different cutoff scores for staining by CK5/6, CK14, and CK34betaE12 (1%, 10%, and 33.3%, respectively). However, based on the sensitivity and specificity, we consider that a cutoff score of 2 is appropriate.
We observed that CK34betaE12 stained significantly more cells than CK5/6 and CK14 in IPUDH. Therefore, positive staining of <1% of all tumor cells for HMWCKs may indicate SPC in situ, whereas >33% positive staining may indicate IPUDH.
Footnotes
Acknowledgements
The authors thank Ms Shigeko Ohnuma for technical assistance. I.M. contributed to conceptualization, methodology, resources, writing–original draft, writing–review and editing, project administration, and funding acquisition; S.T. contributed to resources and writing–review and editing; Y.K. contributed to writing–review and editing; and K.T. contributed to review and editing; M.T. contributed to review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the ethics committee of St. Marianna University (approval no. 1524).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Japan Agency for Medical Research and Development (nos 16lk1010007h0001 and 17lk1010006h9902).
Informed consent
Written informed consent was obtained from legally authorized representatives before the study.