
Abstract
Objectives:
The objective of this study was to report the feasibility and safety of a novel 4-trocar approach for transoral endoscopic thyroidectomy via the vestibular.
Methods:
In this study, we first used 4 trocars via vestibular area to perform transoral endoscopic thyroidectomy. We reported the safety and surgical feasibility of transoral endoscopic thyroidectomy using a 4-trocar technique in our institute from February 1, 2020, to May 10, 2020.
Results:
Transoral endoscopic thyroidectomy via the vestibular approach using 4 trocars was carried out in 5 patients. No complications such as bleeding, mental nerve injury, recurrent laryngeal nerve injury, or hypoparathyroidism were reported. All patients were completely satisfied with the cosmetic results.
Conclusions:
Transoral endoscopic thyroidectomy with 4 trocars via vestibular approach is an effective and feasible method. Markedly, this technique can assist surgeons to expose and preserve both parathyroid glands and recurrent laryngeal nerve easily when performing transoral endoscopic thyroidectomy.
Introduction
The transcervical thyroidectomy is still applied worldwide as a surgical standard to treat several thyroid diseases. 1 Nonetheless, the scar in front of the neck area has negative effects on young women in Asia where aesthetic issues are concerned. Recently, the transoral endoscopic thyroidectomy via vestibular method has been widely carried out for its promising advantages. 2 The procedure was performed based on Anuwong technique which consists of 3 trocars placed in the vestibular area of the lower lip (1 trocar 10-15 mm at the middle and 2 trocars 5 mm on both sides). 3 Nevertheless, from our prospective of view, there are certain limitations with 3 trocars in which 1 trocar is set for the camera and only the other 2 are used for the thyroidectomy. Indeed, applying a 5-mm trocar to pull the thyroid lobe to the opposite side, it can be difficult in exposing and preserving parathyroid glands and recurrent laryngeal nerve while only using the other 5-mm trocar. On the other hand, it could be challenging even for experienced surgeons to control bleeding intraoperatively especially in Tubercle of Zuckerkandl landmark or the tracheoesophageal groove.
Therefore, we improve the technique by placing 4 trocars to perform the procedure more easily in a narrow cavity. To the best of our knowledge, this is also the first report in the literature that 4 trocars are used in the transoral endoscopic thyroidectomy via the vestibular approach.
Patients and Methods
All female patients with a right benign thyroid tumor were performed transoral endoscopic thyroidectomy using a 4-trocar technique in our institute from February 1, 2020, to May 10, 2020. Thyroid fine needle aspiration result revealed a benign tumor (Bethesda II) and thyroid function tests were normal. The patients had a desire to remove the tumor with the highest aesthetic results by surgery. The patients were performed right transoral endoscopic hemithyroidectomy with 4 trocars via oral vestibule area by a high-volume endocrine surgeon who had carried out many transoral endoscopic thyroidectomy vestibular approach (TOETVA) procedures. The study was approved by the ethics committee of our hospital.
Operative Technique
Preparation for surgery
The patient was placed in the supine position with the neck extended. General anesthesia with nasotracheal intubation was initially implemented on the patient. After that, 30 minutes before the initial incision, the patient was prescribed by the prophylactic antibiotic (amoxicillin–clavulanic acid). Povidone-iodine was used to sterilize the oral cavity.
Surgical Steps
Step 1: Inserting 3 trocars
The middle of the oral vestibule was initially incised by a 15-mm incision. Then, the tunnel from the first incision to the chin was created by using an electrocautery. A Veress needle with a 1:10 000 epinephrine solution in normal saline is inserted to the subplatysmal area in order to further develop this plane. A 12-mm trocar was placed into the first incision to subplatysmal space. The visualization could be supplied by the placement of the standard 10-mm, 30° laparoscopic camera in the middle port with 6-mm Hg CO2 pressure insufflated. A right 5-mm lateral incision was made in the vestibular area of canine and first premolar teeth. Then, a left 5-mm lateral incision was placed similarly to the right side; however, the location is slightly higher and closer to the lower lip to insert the fourth trocar more easily. Finally, two 5-mm trocars were inserted into the subplatysmal space. An external 2-0 absorbable suture was placed in the anterior midline of the neck in order to elevate subplatysmal tissue for expanding the space.
Step 2: Creating a working space
The working space was expanded further caudally by a laparoscopic cautery hook and ultrasonic scalpel to reach the sternal notch inferiorly and to the sternocleidomastoid laterally. Then, the 4 incision was made in the left oral vestibular area (Figure 1) in order to insert the four 5-mm trocar into the working space. The assistant held both the scope and the fourth trocar.
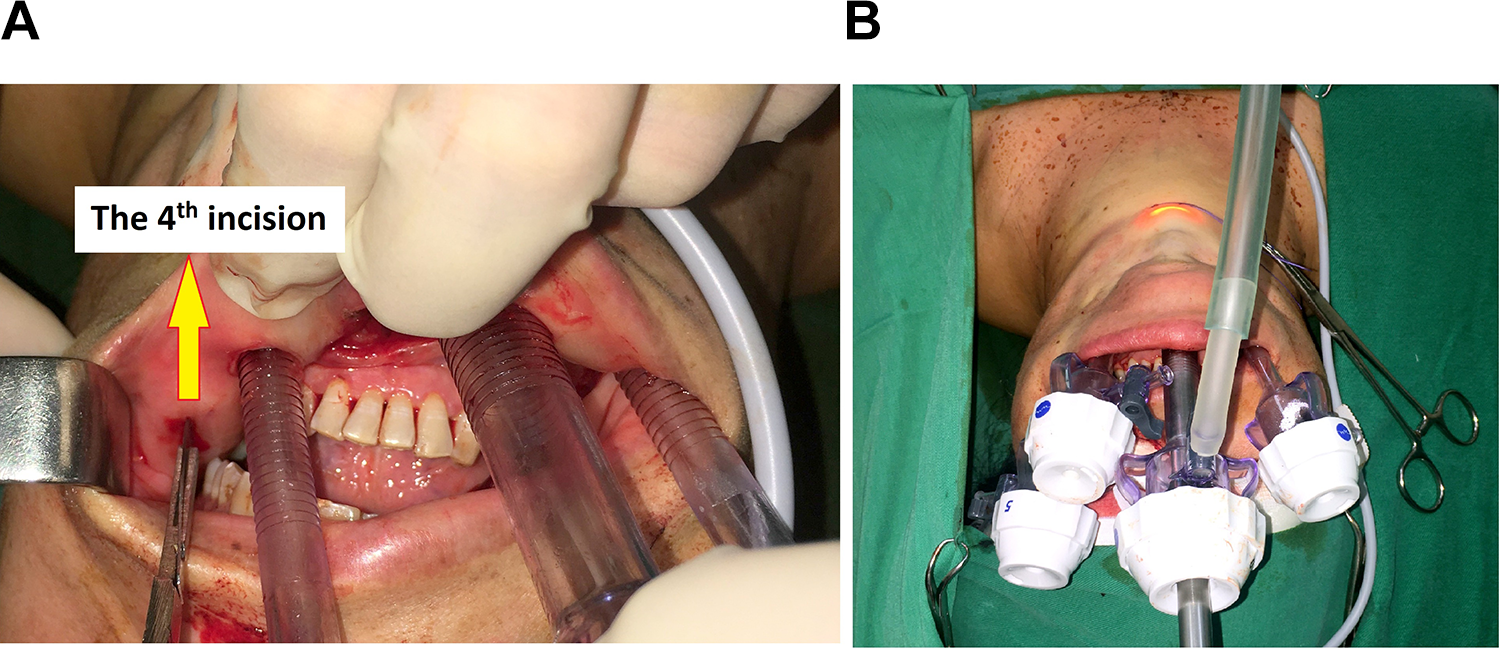
A, The 4 incision was made in the oral vestibular. B, Four trocars through oral vestibular were placed.
Step 3: Exposure of the thyroid gland
The strap muscles were divided in the midline. Then, the right ipsilateral strap muscle was laterally retracted by a transcutaneous 2-0 silk suture to enhance the working space. This step could be better carried out by using of the fourth trocar (Figure 2).
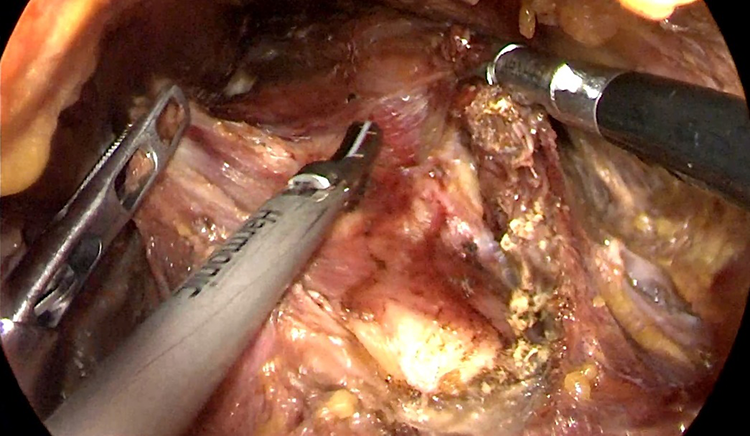
The fourth trocar helped exposure thyroid lobe better.
Step 4: Dissection of the thyroid gland
The pyramidal lobe of the thyroid gland was dissected from isthmus and trachea. Next, the superior thyroid vessels were exposed by the plane bound by the right thyroid lobe and the cricothyroid muscle. Then, the vessels were ligated and divided close to the thyroid lobe with the ultrasonic scalpel to avoid the external branch of the superior laryngeal nerve damage.
The facilitation of the fourth trocar to pull thyroid lobe to the opposite side could efficiently assist the surgeons to use the other two 5-mm trocars to expose the upper parathyroid gland and recurrent laryngeal nerve (Figure 3).
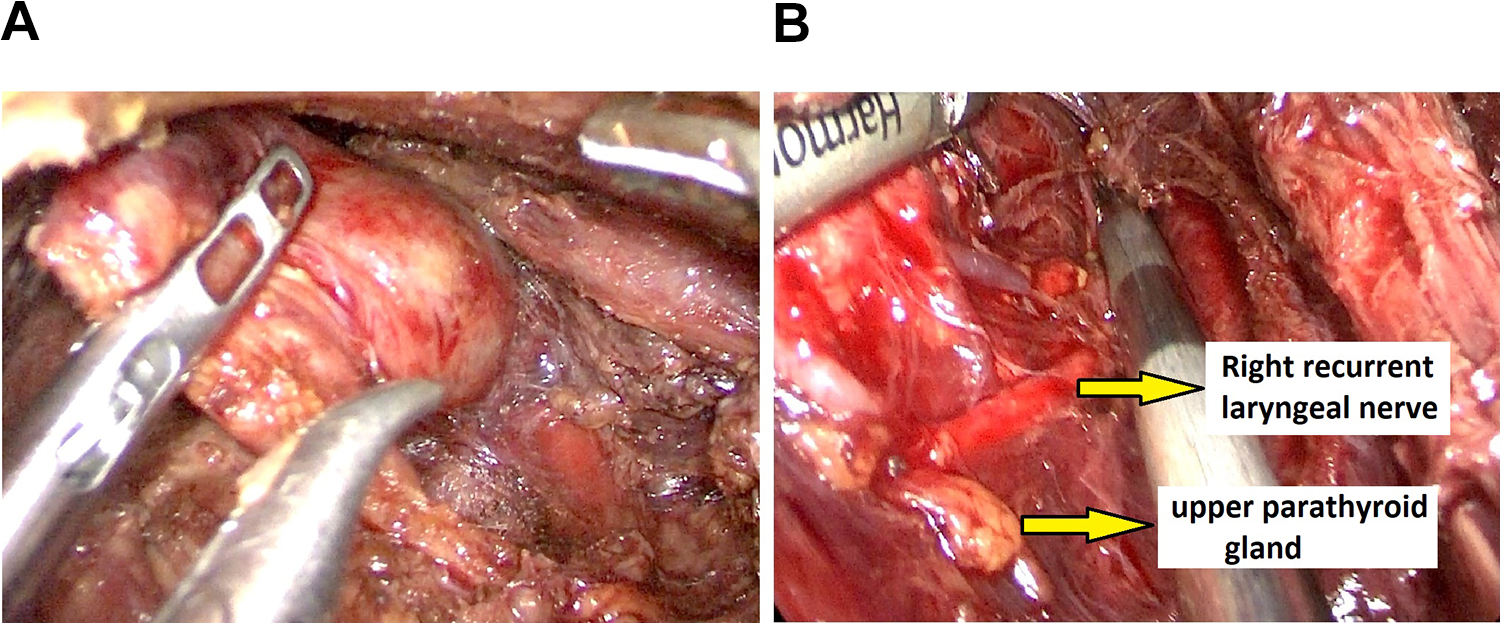
A, The fourth trocar to pull thyroid lobe to the opposite side. B, The upper parathyroid gland and recurrent laryngeal nerve were exposed and preserved.
After that, right lobectomy was carried out with a harmonic scalpel with preserving both parathyroid glands and right recurrent laryngeal nerve (Figure 4).
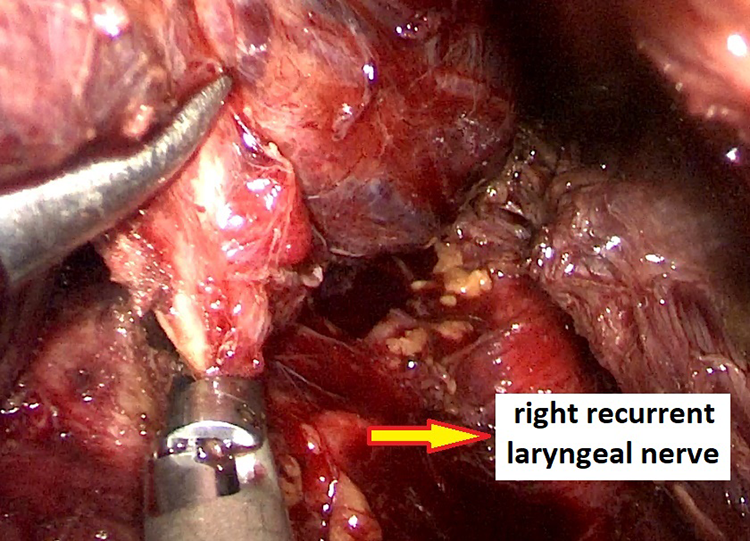
Right lobectomy was carried out with a harmonic scalpel with preserving both parathyroid glands and right recurrent laryngeal nerve.
The thyroid specimen was placed in a retrieval bag and removed via the central trocar. The strap muscles were closed with a 3-0 absorbable suture. The trocars were removed and the incisions were closed by 2 layers with absorbable interrupted sutures (Figure 5). A drain was not placed and a pressure dressing was applied on the chin and upper neck for a day.
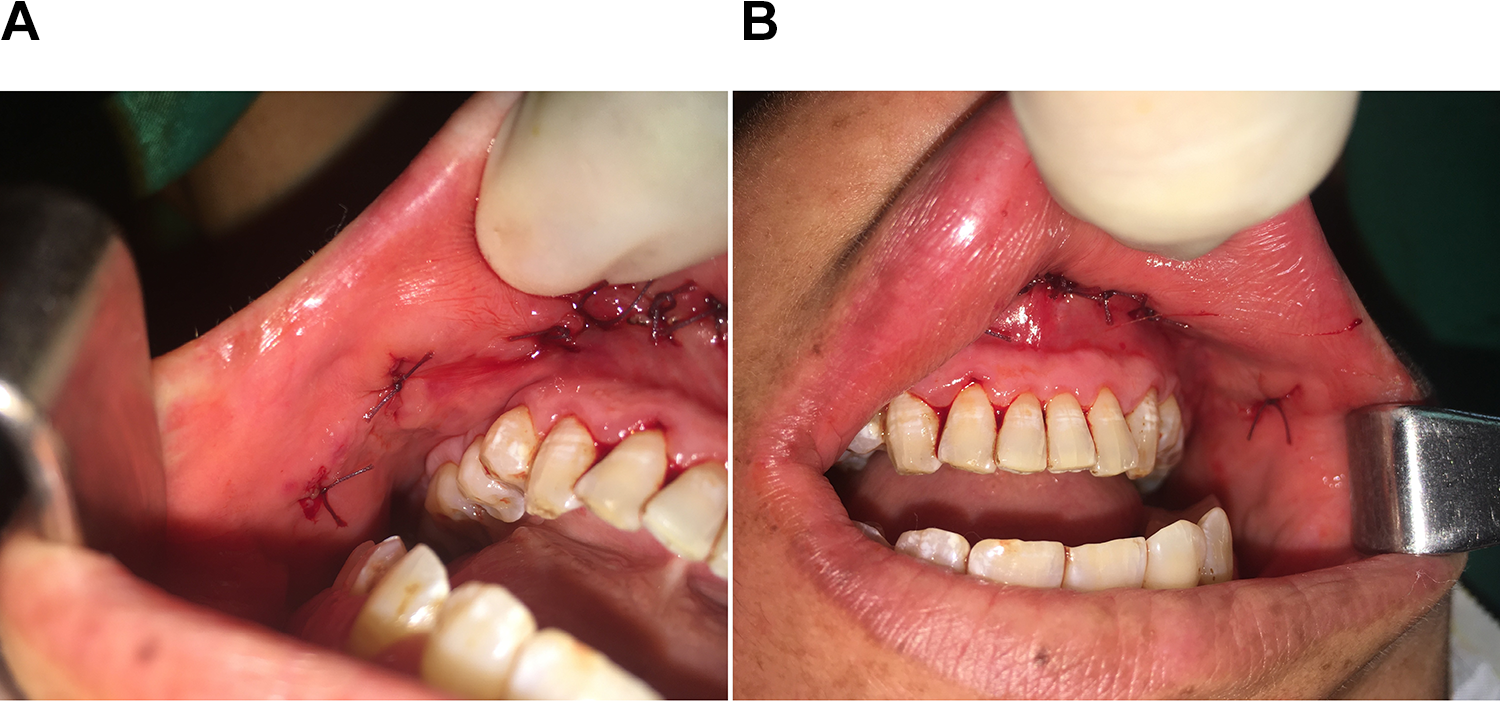
The four incisions were closed by 3.0 absorbable sutures.
Postoperative Management
The patient was carefully checked for signs of bleeding, recurrent laryngeal nerve injury, or difficulty breathing. RLN injury was defined as impaired movement of the vocal cords on laryngoscopy postoperatively. Mental nerve injury was defined as lower lip paresthesia after the surgery. Povidone-iodine 1% was used to rinse the patient’s mouth. On the day of surgery, a liquid diet was provided. Then, soft oral foods were permitted on the first day after operation. Postoperative oral antibiotics were prescribed for 3 days.
Ethical Considerations
This study was approved by the ethics committee in human research (EC1342). Written informed consent to participate in this study was provided by all patients enrolled. All authors abided by the Declaration of Helsinki.
Results
Five patients were operated successfully with transoral endoscopic thyroidectomy using 4 trocars via oral vestibular area. The data of the patients were illustrated in Table 1. The mean operative time was 90 minutes. The pathological results were benign. No patients underwent conversion to open transcervical thyroidectomy. The patients were discharged 3 days after surgery without any complications such as bleeding, infection, mental nerve damage, permanent hoarseness, or hypoparathyroidism. All patients were completely satisfied with the cosmetic result (Figure 6).
The Patients’ Data.


The patient had excellent cosmetic results and was pleased with the aesthetic outcome.
Discussion
Transoral endoscopic thyroidectomy vestibular approach is a new novel technique that offers the best cosmetic result. Many studies have shown the safety and feasibility of this technique in both benign and malignant lesions of the thyroid.4,5 As this procedure only requires some of the basic endoscopic instruments, TOETVA can be broadly applied to plenty of health facilities worldwide, even in places whose medical facilities have not developed yet. 6 Furthermore, the learning curve for TOETVA appears to be relatively short. 7
Notwithstanding initially perform the same TOETVA similar to other authors worldwide, we discover that the 3 trocars approach in which one was in the role of the camera, while 2 others for endoscopic thyroidectomy have certain limitation especially in parathyroid glands and recurrent laryngeal nerve exposure. Indeed, applying a 5-mm trocar to pull the thyroid lobe to the opposite side, it could be difficult in exposing and preserving parathyroid glands and recurrent laryngeal nerve while only using the other 5-mm trocar. On the other hand, when bleeding occurs intraoperatively especially in Tubercle of Zuckerkandl landmark or the tracheoesophageal groove, one 5-mm trocar is used to mobilization of thyroid pole, and there is only the other 5-mm trocar to control bleeding. This step could be a challenge even for experienced surgeons. Thus, it can lead to recurrent nerve injury in this case. Moreover, in some circumstances, total thyroidectomy is indicated for treating thyroid cancer, and it would be difficult to perform all thyroid tissue at the entry point of the recurrent laryngeal nerve.
To circumvent that obstacle, we additionally place a 5-mm trocar in the oral vestibule area so that we can perform thyroidectomy while easily preserving the recurrent laryngeal nerve and parathyroid glands. After cutting the thyroid upper vessels, the facilitation of the fourth trocar to pull thyroid lobe to the opposite side could efficiently assist the surgeons to use the other two 5-mm trocars to expose the upper parathyroid gland and recurrent laryngeal nerve.
Another benefit of the 4-trocar technique in thyroid surgery is application in central neck lymph nodes dissection. More specifically, the fourth trocar helps pushing the trachea to the opposite side in order to expose obviously the central neck lymph nodes. As a consequence, the surgeon may use the other two 5-mm trocars more flexibly to remove the central neck lymph nodes.
Despite the fact that the oral vestibular region is narrow, the addition of the fourth trocar does not bring more specific complications related to TOETVA technique such as mental nerve injury caused by lateral ports or surgical site infection. In our study, we have performed TOETVA 5 cases with 4 trocars, and there is no patient with inherent trauma to the lip warrant or other complications such as marginal mandibular branch of the facial nerve injury, recurrent laryngeal nerve injury, hypocalcemia, hematoma, tracheal injury, and conversion to open thyroid surgery.
Actually, the patients’ outcomes were excellent, and the patients were discharged on the third day after surgery without any complication. Furthermore, our patients had excellent cosmetic results and was pleased with the aesthetic outcome.
To the best of our knowledge, this is also the first report of TOETVA with 4 trocars in the literature. However, the feasibility and long-term outcomes of the innovative technique should be fully evaluated in a larger sample size.
From our point of view, 5-trocar approach is not better than 4-trocar approach to perform thyroidectomy bilaterally because of the following reasons: (1) There is no need to add the fifth trocar to perform thyroidectomy because 4-trocar approach is enough to retract thyroid lobe bilaterally; (2) if the fifth trocar is inserted, the trocars are too close to perform thyroidectomy in a narrow cavity. Thus, it may not only bring benefits but also bring some harms for surgeons.
Conclusion
Transoral endoscopic thyroidectomy with 4 trocars via vestibular approach is an effective and feasible method. Markedly, this technique outstandingly assists surgeons to easily perform transoral endoscopic thyroidectomy.
Footnotes
Authors’ Note
All authors contributed and critically revised the manuscript. Duy Quoc Ngo drafted the manuscript. All authors approved of the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.