
Abstract
In adults, a large metal foreign body in the esophagus is rarely seen and is usually caused accidentally. Here, we have described an unusual case of foreign body (spoon) in the esophagus of an adult patient. A 48-year-old woman initially presented to the emergency department with marked dysphagia, drooling, and radiating pain to the chest. She had swallowed a spoon while trying to vomit because of feeling sick. Radiological images revealed a spoon stuck in the esophagus. The edge of the spoon was grabbed with forceps and safely extracted under hypnic anesthesia. No esophageal perforation was detected on evaluation with esophagography using Gastrografin on the next day. This case highlights an unusual situation in an adult patient showing long nonfood-type foreign body in the esophagus. It is important that an appropriate workup and removal of foreign body is performed according to the location and type.
A 48-year-old woman presented to the emergency department with marked dysphagia, drooling, and radiating pain to the chest. She had swallowed a spoon while trying to make herself vomit because of abdominal discomfort. She had no past medical history, including mental illness and neuromuscular disease.
Plain radiograph of the neck with anteroposterior (Figure 1A) and lateral views (Figure 1B) showed that the spoon was lodged from the hypopharynx to the esophagus up to the level of the seventh thoracic spine. The spoon bowl was observed to be stuck in the larynx using a nasopharyngolaryngoscope. First, we attempted to remove the spoon by grabbing and pulling it with a rigid laryngoscope. However, the patient complained of pain in her larynx, and we halted this procedure.
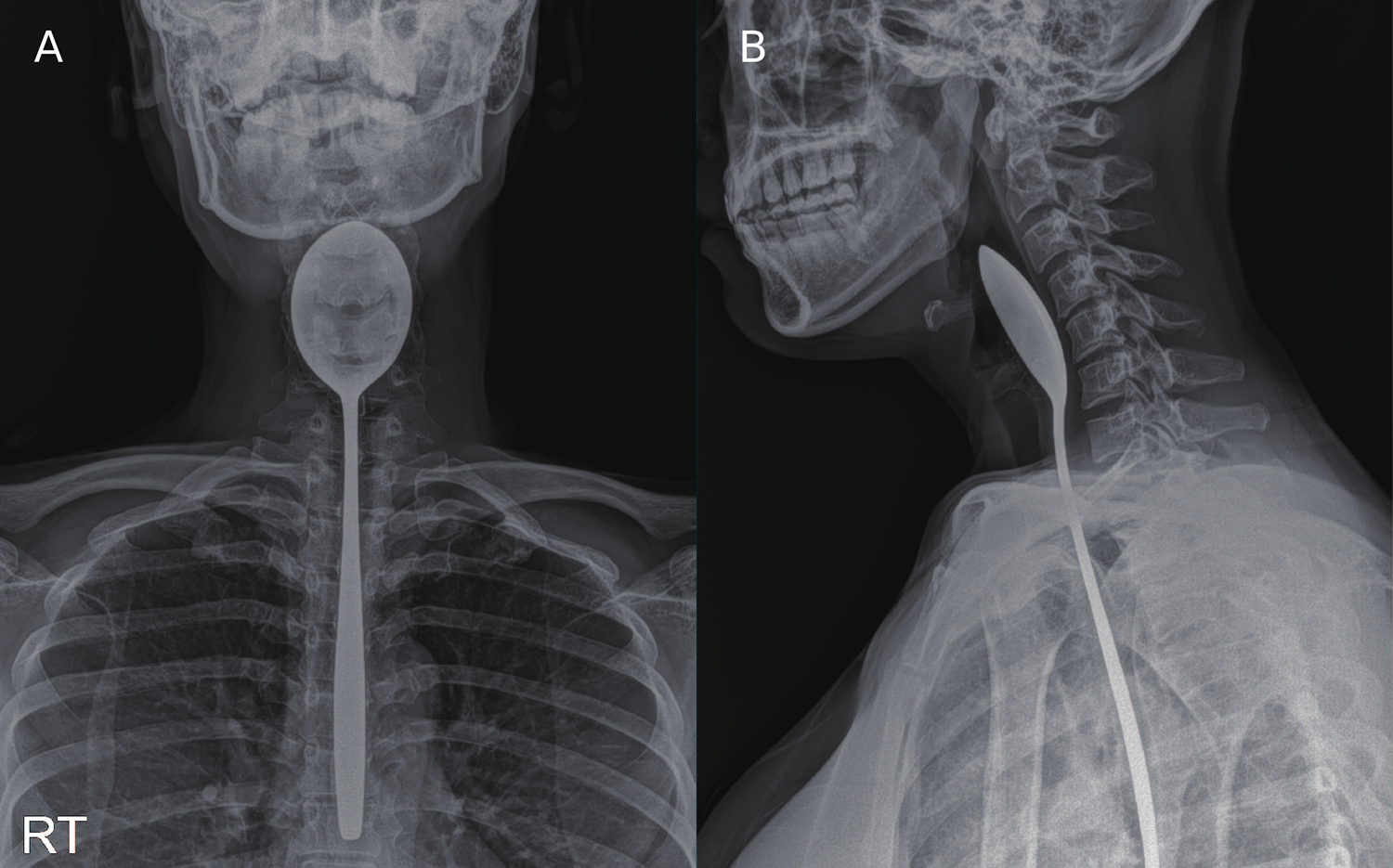
Radiographic imaging. A, Neck anteroposterior view, the spoon can be seen vertically in the esophagus. B, Neck lateral view, the spoon can be seen sideways in the esophagus. RT indicates right side.
Subsequently, we observed the spoon using a suspension laryngoscope in the Boyce position under hypnic anesthesia. The spoon edge was grabbed with Kelly forceps and safely extracted. No other foreign bodies (FBs) or lesions were detected in the larynx and hypopharynx during an additional examination after the spoon extraction. The spoon was 24.8 cm in length, with the spoon bowl being 7.7 cm × 4.7 cm × 1.8 cm at its largest point (Figure 2).

Removed foreign body. The spoon, which was removed from the esophagus was 24.8 cm in length, and the spoon bowl was 7.7 cm × 4.7 cm × 1.8 cm at its largest point.
Evaluation with esophagography using Gastrografin was performed the next day. No signs of esophageal perforation were detected. Since the patient did not complain of any discomfort and had stable vital signs, she was discharged. At the follow-up visit at the otolaryngology outpatient clinic 6 days after the removal, no specific signs were observed in the larynx and pharynx on laryngoscopic examination.
Laryngeal or esophageal FBs are common presentations at otolaryngology clinics. Foreign body cases are more prevalent in children, particularly those aged between 6 months and 6 years. 1 Sharp FBs such as fish bones are most frequently found lodged in the tonsils, while other food or large nonfood-type FBs are commonly found in the esophagus. Small nonfood-type FBs such as batteries are commonly found in the stomach, which require particular attention because they cannot be dissolved or absorbed in the aerodigestive tract. 2 Nonfood-type FBs are commonly found in children because they often accidentally swallow FBs. 3 Generally, food-type FBs, such as fish and chicken bones, are commonly observed in adults. In adults, nonfood-type FBs have been reported as accidental or in patients with a mental illness. 1
The esophagus has 3 physiological stenosis areas, the upper esophageal sphincter, the transition between striated and smooth muscle, and the aortic arch narrowing. The esophagus is the most common site for FBs to become lodged, especially nonfood-type FBs or fish bones.1,4 Esophageal FBs can result in dysphagia, odynophagia, retrosternal pain, choking, and dyspnea, 5 which may be due to laryngeal or pharyngeal irritation. Persistent FBs in the larynx or esophagus can cause serious complications, such as esophageal perforation. Therefore, patients that present with retrosternal pain, chest pain, or sore throat need to be carefully examined. However, we also have to keep in mind that some patients are asymptomatic. 5
Most adults can provide reliable information on the FB type, ingestion time, and symptoms suffered. Physical examination is needed to evaluate FB-related complications. The presence, location, size, configuration, and the number of ingested FBs can be assessed with plain radiography. 5 However, some FBs such as food boluses, fish bones, and glass cannot be detected by plain radiograph and require additional examinations such as esophagoscopy and computed tomography (CT). Rigid or flexible endoscopy can be used if an additional examination is needed. 5
In our case, the patient presented with typical symptoms, including marked dysphagia, drooling, and radiating pain to the chest. First, we tried to remove the spoon by pulling it while the patient was in a sitting position with no anesthesia. However, she complained of a painful sensation in the laryngeal and esophageal areas. Sustained irritation to the esophagus without sedation can result in additional esophageal damage if patients move in response to pain. Therefore, we desisted with this procedure. Next, we attempted to remove the spoon in the Boyce position under hypnotic anesthesia. Suspension laryngoscopy in the Boyce position is considered as the optimum position for direct visualization of the larynx and hypopharynx, including the upper esophageal sphincter area and can help to reduce damage to the esophagus during FB removal. We were able to successfully remove the FB from the esophagus using this procedure without complication.
To the best of our knowledge, there have been few cases of nonfood-type FB ingestion in healthy adults. In 2 cases in the last 10 years,6,7 adult patients with a normal mental status have accidentally swallowed a long FB while trying to induce vomiting, similar to this case. However, in these cases, the FBs were removed using esophagogastroduodenoscopy instead of laryngoscopy.
Nonfood-type FBs stuck in the esophagus rarely occur in healthy adults. While the majority of FBs in the esophagus pass through the gastrointestinal tract without perforation, long nonfood-type FBs might not pass through the esophageal tract without complication and require immediate treatment. Therefore, nonfood-type FBs stuck in the esophagus should be evaluated and removed to reduce the risk of serious complications such as esophageal perforation.
Footnotes
Authors’ Note
Ethics committee approval was obtained from the institutional review board and ethics committee at the Myongji Hospital, Korea.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.