
Abstract
A 37-year-old incarcerated male with a history of schizophrenia presented to the emergency department with dysphagia after intentional ingestion of a metallic foreign body. Past medical history was remarkable for multiple prior procedures for removal of esophageal and gastrointestinal foreign bodies. The patient was not in distress and tolerating his secretions. Flexible laryngoscopy was unremarkable. Plain radiography was remarkable for a radiopaque metallic foreign body, consistent with the face of a combination lock, located at the thoracic inlet within the proximal esophagus (Figure 1). The patient failed flexible endoscopic removal by gastroenterology and underwent rigid esophagoscopy with removal of the esophageal foreign body in the operating room (Figure 2).
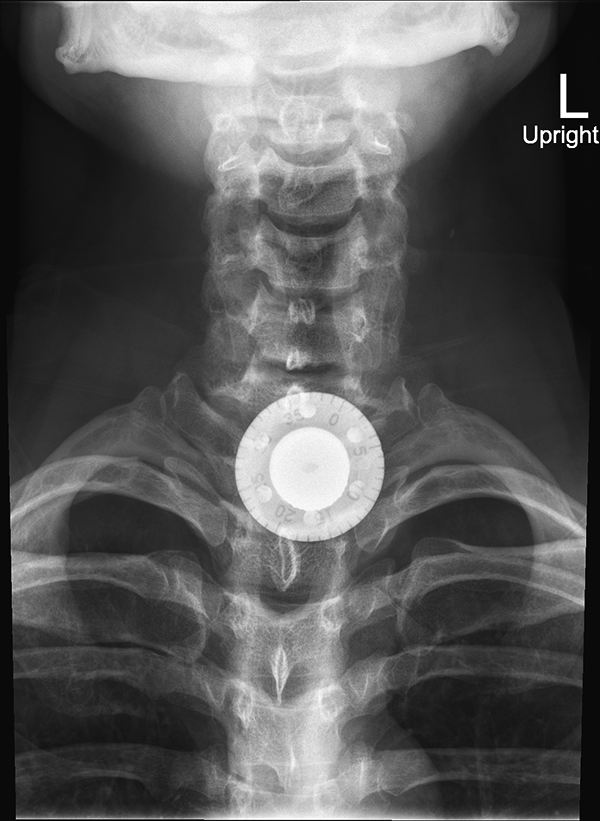
AP radiograph of the neck showing a radiopaque metallic foreign body, consistent with the face of a combination lock, located at the thoracic inlet within the proximal esophagus.
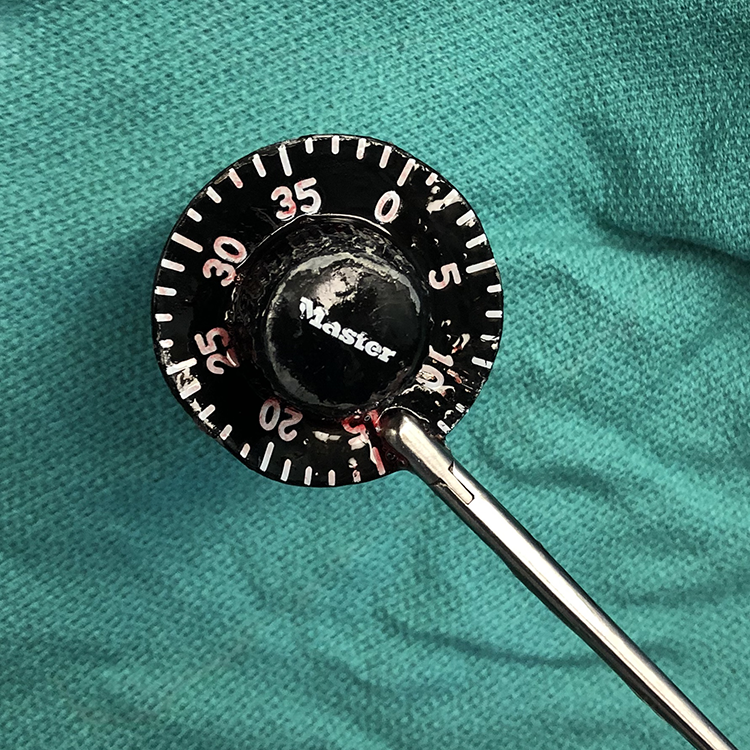
Foreign body after removal by rigid esophagoscopy.
Intentional ingestion of foreign bodies is increasing in incidence and is associated with incarceration, psychiatric disorders, and substance abuse. 1 Motivating factors include malingering, psychosis, pica, and personality disorders. 2 Repeat offenders account for a disproportionately high percentage of intentional ingestions, underscoring the psychosocial factors that drive this behavior.3-4 Psychiatric treatments specific to intentional ingestion have been poorly studied, though the role of behavioral therapy and pharmacologic intervention with antipsychotics or antidepressants appears to be limited in preventing recurrent foreign body ingestion. 4 Prevention of intentional ingestion in the incarcerated population may need to focus on limiting unsupervised access to potentially ingestible foreign bodies. The most commonly ingested objects in prisoners include pens, eating utensils, razor blades, toothbrushes, and various other metal objects, such as combination locks. 5
Management of ingested foreign bodies is dependent on presenting symptoms, foreign body location, number of ingested objects, and associated complications. Most foreign bodies can be successfully removed endoscopically, with surgery reserved for failed endoscopic removal or in the presence of other indications, such as perforation.3,5 Approximately 50% of patients with intentional ingestions present with a foreign body in the stomach, and less than 10% present in the esophagus.3,5 Although some advocate for a conservative observational approach specifically for inmates, 6 foreign bodies that are impacted in the esophagus typically warrant removal, and emergent intervention may be indicated with esophageal obstruction or with specific foreign bodies, such as disc batteries or sharp objects. 7
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.