
Abstract
Objectives:
Ear deformity caused by burns is one of the most difficult types of deformity to treat with plastic surgery, and the reconstruction of burned ears undoubtedly remains a substantial challenge. This study aims to report the therapeutic regime of using a superficial temporal fascial flap to cover the framework in burned ear reconstruction.
Methods:
Autologous costal cartilage was used to form the ear framework in all of the reconstruction cases. A superficial temporal fascial flap was used as soft tissue to cover the ear scaffold.
Results:
Five patients with 6 ears were included in our study. The external ear healed well and the location, size, and shape of both ears were generally symmetrical. No complication was observed in any of the patients.
Conclusions:
The superficial temporal fascial flap is a good choice for covering the autogenous cartilage framework when treating ear deformities after burns.
Introduction
As a dominant landmark of the human face, the pinna not only maintains facial symmetry and aesthetics but also plays an important role in collecting sound waves into the auditory canal and maintaining the environmental stability for the middle and inner ear.1,2 The prominent and fixed position makes the auricle vulnerable to flame and chemical burns, and the limited vascular in the cartilage and the thin subcutaneous tissue makes auricular burns a unique type of facial burns. Facial burns that involve the auricle are associated with greater total body surface area and often require a longer hospitalization. 3 According to Gault, who reviewed 249 patients with traumatized ears, burned ears had worse results compared with other mechanisms of injury, and an increased rate of complications was observed after reconstruction. 4 Repairing and reconstructing burned ears are of great benefit for the rehabilitation of the patient’s mental and social well-being, and these processes are also important for patients who wear glasses and earrings.
Similar to ear reconstruction in patients with congenital microtia, the 2 primary principles for reconstructing burned ear deformities are the transplantation of a moderately elastic scaffold and the use of covering tissue with a matched color and adequate vascular supply.5,6 Numerous studies have focused on the application of an autologous costal chondral graft or prefabricated porous polyethylene implant as the ear scaffold.6,7 However, the skin in and around the auricle is often damaged due to the burn deformity, resulting in scar hyperplasia and bad skin quality with poor blood supply and reduced elasticity; these features represent additional challenges for plastic surgeons for ear reconstruction.3,4 In this article, we introduced our experience of ear reconstruction using a superficial temporal fascia flap for patients with burn damage.
Patients and Methods
Clinical Data
We performed ear reconstruction using superficial temporal fascia flaps in 5 patients, who had from ear deformity caused by burns, from January 2013 to December 2016. This study included 4 men and 1 woman ranging in age from 5 to 42 years. One patient had bilateral injuries, and the remaining patients all experienced unilateral ear deformities. The cause of the burns was flame, with the exception of 1 patient who was injured by boiling water. More detailed information is provided in Table 1. This study was approved by the Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, and all the patients or their parents provided written informed consents.
Demographic features of the patients.

Preparing for the Operation
The residual auricle and the skin around it were the main factors when performing an assessment before the operation. All the patients included in this study had severe scars in the mastoid region and the postauricular fascia could not be used. Patients were told to clean the skin of the postauricular region carefully with soapy water the day before the surgery. It is important to be aware of the variability in the vasculature, so Doppler ultrasound was used to identify the ipsilaterally robust axial vessel. An X-ray film was used to create a template per the intact contralateral auricle. For the patients with bilateral ear deformity, the ear of a family member or anthropometric measurements of the auricle could be used as references. The psychological status was also an essential component of the preoperative evaluation. Patients who had extremely high expectations received specific counseling before the surgery. Therefore, future disappointment in unexpected results can be avoided by eliminating unrealistic objectives. The general condition of the patient was always the most important when considering the risks and benefits of surgical options. Patients with severe cardiovascular disease were advised not to undergo plastic surgery due to poor health.
Surgical Procedures
General anesthesia was administered, and the patient was placed in a supine position. Autologous costal cartilage was used to form the ear framework in all of the reconstructed patients (Figure 1). A fusiform incision was designed on the chest just above the costal margin, and the skin was excised to create a full-thickness skin graft, which would be used later. We preferred the right side of the chest to prevent exposure of the heart if the ribs were harvested from the left side. After the rectus abdominis was incised, the appropriate amount of costal cartilage was harvested according to the film. Then, the costal cartilage was carved and sutured together into a new framework.
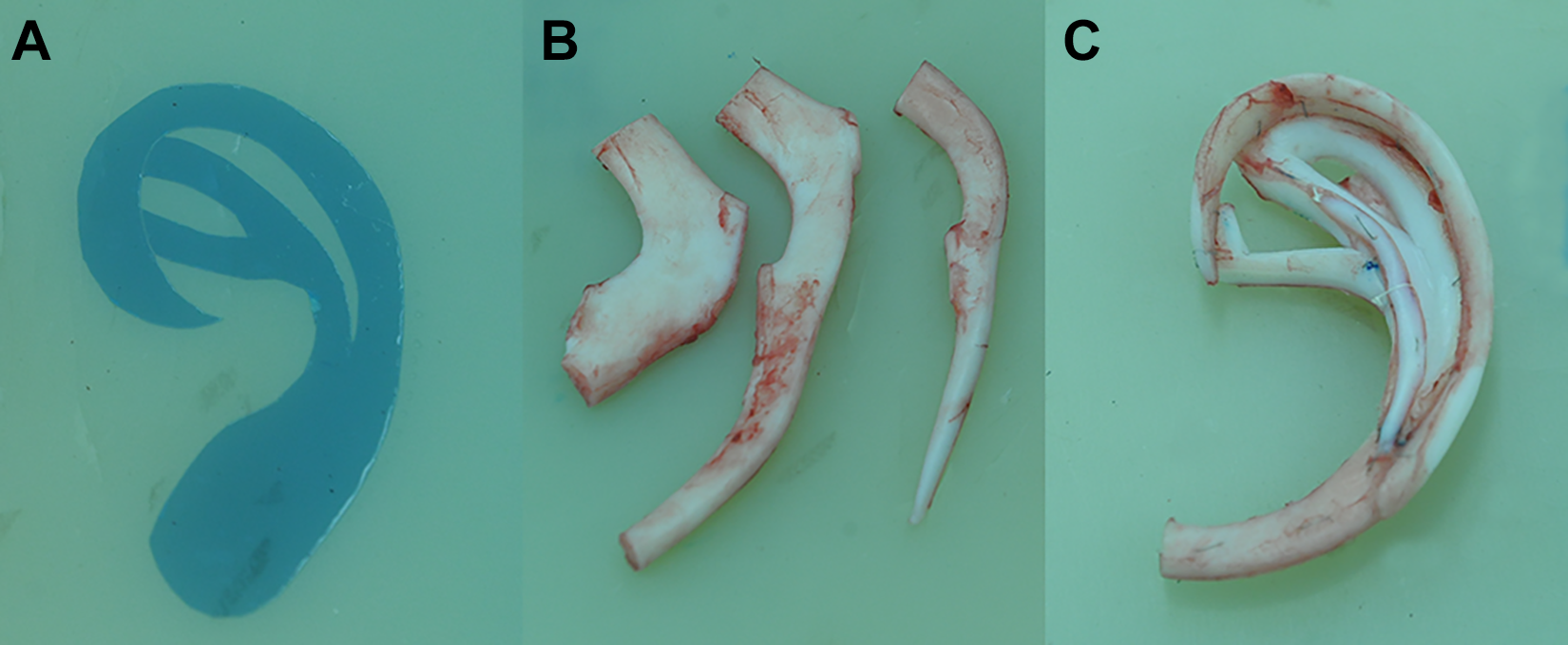
The X-ray template and the ear framework. A, The X-ray template; (B) cartilages from the sixth, seventh, and eighth ribs; and (C) the ear framework.
The scarred skin from the ear remnant was elevated as a thin anteriorly based flap to partly cover the anterolateral surface of the reconstructed ear. Then, the contracted scars and cartilage were excised, and the edge of the residual auricular cartilage was removed. A Y-shaped or curved incision was designed in the hairline above the proposed auricular region according to the preoperatively labeled superficial temporal artery. The scalp was cut below the hair follicles to avoid long-term alopecia. The superficial temporal fascia was raised as an axial pattern flap immediately above the underlying deep temporal fascia, and it was important to take care of vessels in the pedicle. Then, the superficial temporal fascia flap was lifted and rotated inferiorly. The size of the flap was determined by the residual auricle and was large enough to cover the posteromedial portion of the ear stent without tension.
The ear stent was placed posteriorly to external auditory meatus and inserted between the posterior scar flap and the superficial temporal fascia flap. The upper limit was the level of the eyebrow. For patients with partial auricle defects, the residual ear cartilage was connected with the ear scaffold using titanium wire after removing the hyperplastic tissue of the residual ear margin. A suction catheter was placed between the framework and temporal flap to drain the exudate and coapt the flap to the framework for 5 days. The surface of the superficial temporal fascia flap was transplanted with a full-thickness skin graft, and a light pressure dressing applied. The dressing and suture could be removed 12 to 14 days after the operation.
Results
All 5 patients with burned ear deformities obtained good results after reconstruction without any complications, such as skin flap necrosis, poor wound healing, and stent exposure during more than 6-month follow-up period. The reconstructed ears were ruddy in color, which was basically commensurate with the surrounding skin. The reconstructed ear and contralateral ear exhibited similar positions and shapes. Patient satisfaction was high and the results were well accepted.
Patient 1
A 10-year-old boy sought treatment at our department for ear defect (Figure 2A). He had lost his right ear in a flame burn when he was 3 years old. Considering the heavy scars in the postauricular region, we used the superficial temporal fascia flap to cover the autogenous rib cartilage scaffold (Figure 2B and C). The postoperative period was uneventful. The suction catheter was removed 5 days and the dressing and suture were removed 12 days after the operation (Figure 2D). This patient underwent follow-up by telephone for 4 months because of a long distance to the hospital, and he was pleased with the texture and color of his reconstructed ear.
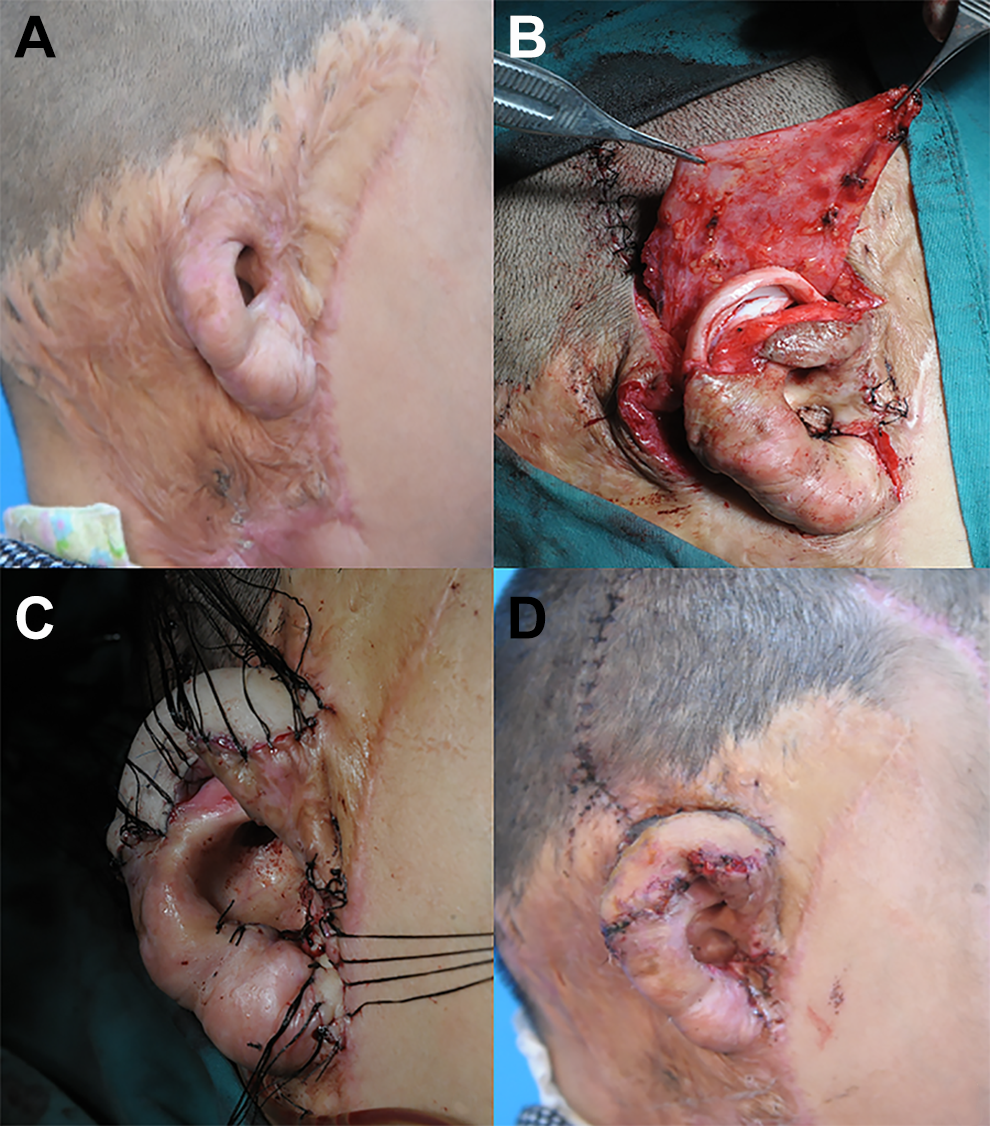
Ear reconstruction using superficial temporal fascia flap in a 10-year-old boy. A, Preoperation view; (B) at the time of superficial temporal fascia flap dissection; (C) immediately after the skin was grafted; and (D) 12 days after surgery when the dressing and suture were just removed.
Patient 2
A 7-year-old boy came to our department with a defective auricle (Figure 3A). He had sustained a severe burn 4 years ago and had undergone plastic surgeries on the right side of his face at another hospital, except for his right ear. The superficial temporal fascia flap was used to cover the framework (Figure 3B and C). The dressing and suture were removed 14 days after the operation, and the flap survived completely. The follow-up period of this patient was 7 months. Good color match was noted between the reconstructed ear and the surrounding skin, and the patient was satisfied with the treatment outcome (Figure 3D).
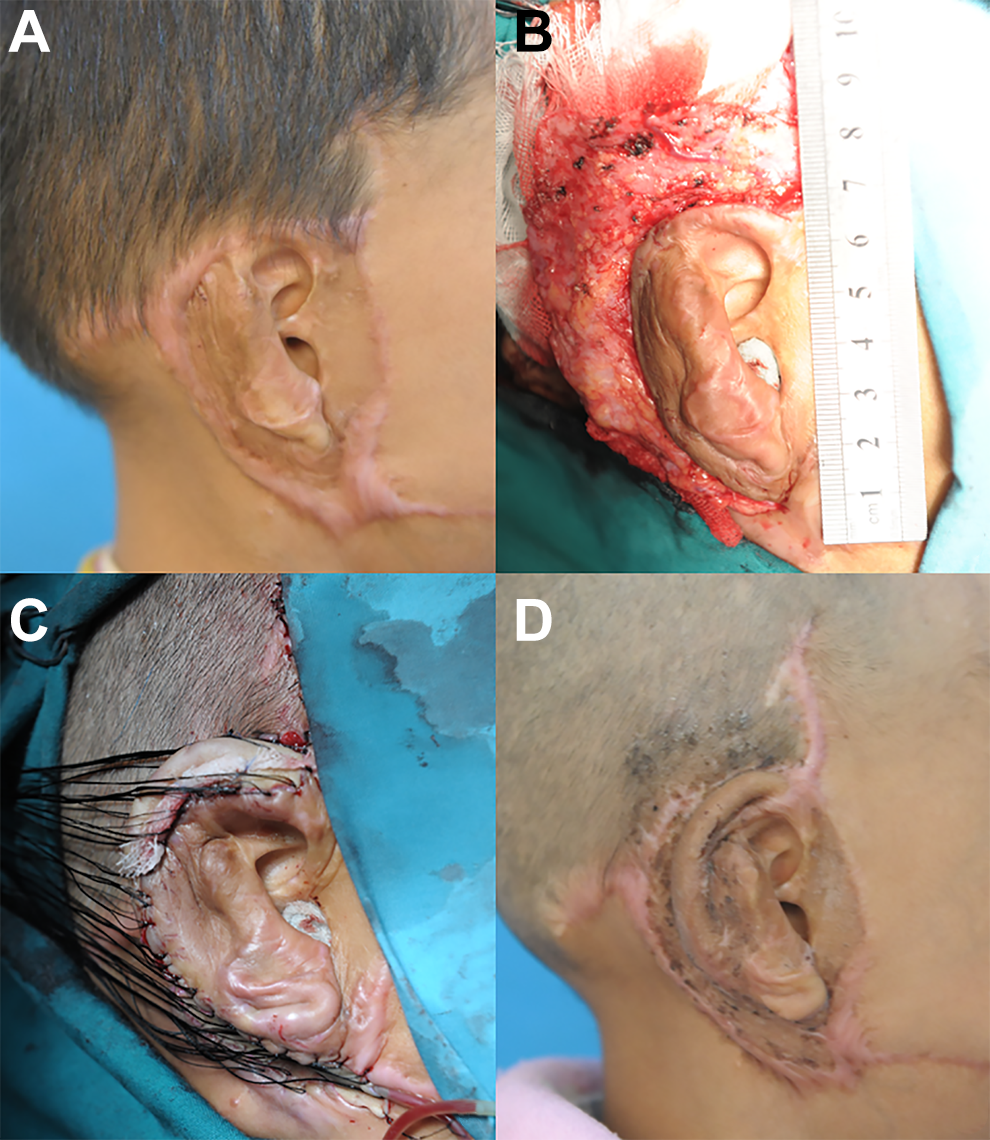
Ear reconstruction using superficial temporal fascia flap in a 7-year-old boy. A, Preoperation view; (B) at the time of superficial temporal fascia flap dissection; (C) immediately after skin was grafted; and (D) 7 months postoperatively.
Patient 3
A 5-year-old boy was burned at 9 months in a scald injury burning the left face (Figure 4A). He underwent ear reconstruction using the superficial temporal fascia flap at our department (Figure 4B and C). The dressing and suture were removed 14 days after the operation. At the 9-month follow-up mark, the reconstructed auricle proved aesthetically satisfactory (Figure 4D).
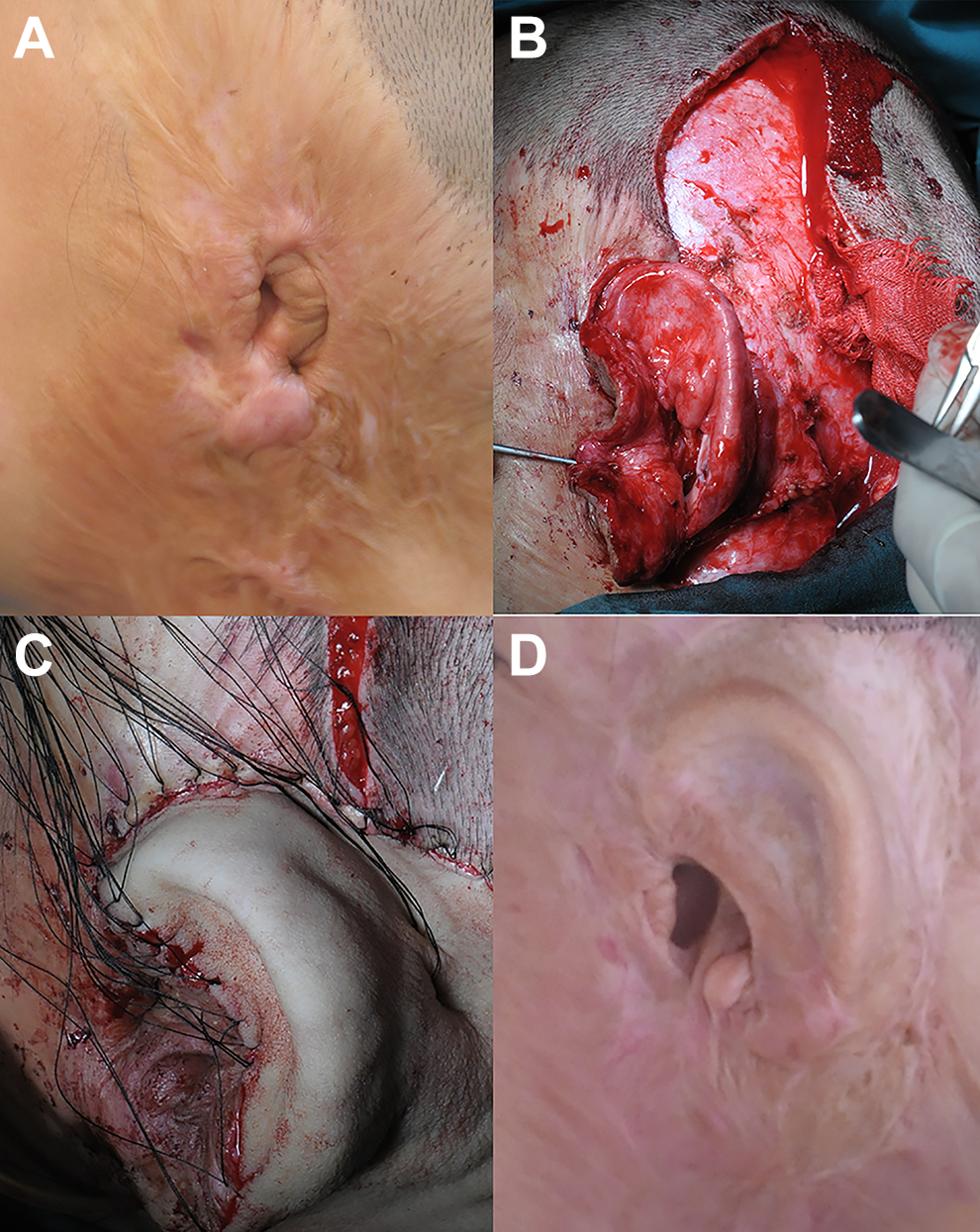
Ear reconstruction using superficial temporal fascia flap in a 5-year-old boy. A, Preoperation view; (B) at the time of superficial temporal fascia flap dissection; (C) immediately after the skin was grafted; and (D) 9 months postoperatively.
Discussion
Most cases of auricular burns involve the skin in and around the ear and leave scar hyperplasia that results in poor blood supply and elasticity of the skin. These features represent a substantial challenge in covering the tissue during auricle reconstruction. However, compared with microtia patients, most patients with ear deformity caused by burns retain part of the ear. Based on the residual ear and external auditory canal, the position of the reconstructed auricle can be accurately located. It is particularly helpful if the tragus normally exists. While methods for frame fabrication from autogenous costal cartilage have been described in many studies, the quality and quantity of the skin in and around the auricle make ear reconstruction following burns an extremely challenging job. In this article, we described our experience using superficial temporal fascia flaps as coverage tissue in ear reconstruction following burn injuries, which obtained satisfying outcomes.
The superficial temporal fascia was first described to reconstruct the lower eyelid by Monks 8 in 1898 and commonly used for ear reconstruction after the 1980s. 9 The superficial temporal fascia is a thin, highly vascular layer that lies immediately underneath the subdermal fibrofatty tissue, and it is a versatile tool that has been widely used in the reconstructive process in the head and neck region as a pedicle and a free and composite flap.10,11 The superficial temporal artery with its frontal and parietal branches provides a rich and constant blood supply to the superficial temporal fascia,12,13 which is enough to nourish both the autologous costal cartilage graft and overlying skin graft. Sufficient perfusion pressure of superficial temporal vessels can satisfy the fascia flap blood supply after the pedicle is folded back. The thin, pliable, and flexible quality; reliable blood supply; and minimal donor site morbidity make this flap an ideal coverage tissue for use as an auricular costal cartilage framework.
A variety of coverage tissue in burned ear reconstruction has been reported in previous studies. The postauricular area or mastoid area is commonly used for soft skin coverage in ear reconstruction based on the adjacent position, high vascularity, and matched color. Expanded postauricular skin flaps and postauricular fascia flaps have been widely used to wrap the framework in microtia patients. However, the severe scar caused by burns in the mastoid area may influence the blood supply and elasticity, limiting the usage of postauricular tissue. In that situation, the superficial temporal fascia flap can serve as an effective alternative. Compared with the postauricular fascia flap, the superficial temporal fascia flap has some disadvantages, including inconvenient cutting and long distance. The blood supply may be affected after the flap is turned over. Furthermore, it is difficult to obtain ideal replacement repair material if stent exposure occurs after the removal of the superficial temporal fascia flap. However, for the burned patients reported in this paper, scar hyperplasia was found in the posterior mastoid region, and the posterior fascial flap could not be used to nourish the reconstructed ear stent. Thus, the superficial temporal fascia flap was the preferred flap for both the scaffold and skin flap graft. In particular, for patients with alopecia after burns, it has been reported that the superficial temporal fascial flap and the bald scalp can be removed together to cover the Medpor ear stent. The bald scalp, which would be discarded during scalp reconstruction, can be completely utilized, and separate procedures, can be avoided. 6 It is recommended that subcutaneous fat should remain in the scalp flap as much as possible to protect the hair follicles. To reduce the incidence of postoperative complications, special attention should be paid to protecting the vascular network between the superficial temporal artery and the posterior auricular artery when dissecting the superficial temporal fascia.
Conclusion
The repair and reconstruction of burned auricle defects should be carefully planned according to location, size, and local tissue scar hyperplasia, and a personalized treatment scheme should be developed to obtain ideal results. In this paper, the superficial temporal fascia flap was used to cover an autogenous costal cartilage scaffold in ear reconstruction for patients after burns. When local tissue is suboptimal due to scarring, the superficial temporal fascia flap serves as a good alternative material to cover the ear scaffold.
Footnotes
Acknowledgements
The authors thank all the patients for their participation and permission in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences [grant number 2018PT31051]; CAMS Innovation Fund for Medical Sciences [grant number 2016-12M-1-002]; and The National Natural Science Foundation of China [grant numbers 81571863 and 81401608] Superficial Temporal Fascia Flap for Ear Reconstruction in Burned Patients.