
Abstract
Introduction
Congenital auricular deformities are common in clinical practice and affect not only the appearance but also the psychological development of children; therefore, they should not be ignored but should be treated early. Congenital auricular deformities are classified either as deformations or malformations. Deformations are characterized by a dysmorphic but fully developed auricle without skin or cartilage loss. Malformations are characterized by partial skin or cartilage loss resulting in an underdeveloped auricle that requires surgical correction. 1
The traditional treatment for congenital auricular deformities is plastic surgery after the age of 5 years, when the ear has reached 90% of the adult size. 2 However, all surgical schemes have disadvantages, such as significant trauma and complications, which increase children’s pain levels and the economic burden on their parents.
The large amount of maternal estrogen in the circulatory system of newborns increases the malleability and plasticity of the cartilage. The estrogen concentration peaks within 72 hours after birth, after which the concentration gradually decreases and then recovers to normal levels 6 weeks after birth. The level of estrogen determines the content of hyaluronic acid in auricular cartilage, which further determines the plasticity and extensibility of the tissue. 3 Accordingly, the mechanical correction of deformed auricles in infancy can prevent the risk and trauma of school-age surgical correction. 4 Nonsurgical correction of congenital auricular deformations was first proposed in the 1980s by Japanese scholars Matsuo et al 5 Subsequently, many countries gradually carried out experimental studies on the nonsurgical correction of neonatal congenital auricular deformities and achieved highly desirable effects. 6 In 2010, Byrd et al innovatively applied new materials to the design of ear molding appliances, creating the EarWell Infant Ear Correction System (Becon Medical Ltd., Naperville, Ill, USA.), which is regarded as an effective model for nonsurgical auricular correction. 4 Nonsurgical correction is superior to surgical correction because it can produce a more natural auricle. Complications associated with nonsurgical correction are mostly limited to minor skin lesions, most of which heal within a few days. 7
From our clinical experience, newborns start treatment relatively late in China. This may be related to the misconceptions held by many parents, obstetricians, and neonatologists. They believe that the deformities will correct themselves over time, so many children may miss valuable opportunities for early nonsurgical correction. Recent studies have shown that only a minority of newborn auricular deformities heal spontaneously. 8 Some authors have demonstrated that ear molding can improve most congenital auricular deformities when employed shortly after birth. 9,10 Early nonsurgical correction provides more benefits for newborns with congenital auricular deformities.
Recent studies on the nonsurgical correction of congenital auricular deformities have mainly focused on factors influencing the success rate, such as the initial age at correction, the type of anomaly, infant feeding style, and complications. 11 -13 However, the sample sizes have been too small to assess the effect for older children.
In this study, we assessed the effectiveness of ear molding for congenital auricular deformities and analyzed the factors affecting treatment success.
Patients and Methods
Patients
This single-center prospective study was conducted from January 2021 to December 2022 in the department of otolaryngology, Second Affiliated Hospital of Harbin Medical University.
All children had intact auricle skin, no eczema or skin lesions, no external auditory canal or middle ear inflammation, and were in good general condition. They were treated with ear molding, a nonsurgical correction technique, using the EarWell Infant Ear Correction System.
Ethics Statement
All treatments were performed at the department of otolaryngology, Second Affiliated Hospital of Harbin Medical University. Written informed consent was obtained for all patients. All procedures were approved by the Human Experimentation Ethics Committee of Harbin Medical University.
Methods
Before correction, the type of auricular deformity was diagnosed by an aurist. According to the classification system developed by Byrd, 4 the types of congenital auricular deformities included in this study were as follows: protruding ear, cup ear, lop ear, Stahl’s ear, helical rim deformity, conchal crus deformity, cryptotia, mixed auricular deformity, and microtia.
The doctor discussed the treatment benefits, risks, and alternatives with the parents, who then signed the informed consent form after being fully informed about the study. Then, the doctor selected the appropriately sized mold. All patients were treated with ear molding (EarWell Infant Ear Correction System) following the class method described in the literature. 13 One week was considered a treatment cycle. The patients were seen weekly for complications, photos, and treatment interruptions, such as shifting of the apparatus. Photographic records of the patients’ ears were taken before, during, and after the treatment and stored. Demographic and clinical information, including age at treatment initiation, treatment cycles, family history of auricular defects, feeding patterns during treatment, treatment decision-makers, psychological status of decision-makers, complications (allergy, pressure sores, dermatitis, bruises), and recurrence were recorded. The treating physician contacted all the children’s families and conducted follow-ups at 1, 3, and 6 months after treatment completion.Photographs were assessed by the aurist, who rated the outcome as poor, fair, good, and excellent. Definitions of the grades are explained in Daniali et al’s study. 14
The treatment decision-makers could be parents or grandparents, and their psychological conditions were assessed to see if they had an impact on the age at which treatment was initiated. During follow-up, the treatment decision-makers were evaluated with a psychological questionnaire. The Hospital Anxiety and Depression Scale (HADS), first proposed by Zigmond and Snaith in 1983, is mainly used to help physicians assess anxiety and depression in inpatients. The self-assessed HADS consists of 14 scoring items for calculating the overall patient score, with 7 anxiety-related items and 7 depression-related items. The anxiety and depression subscale scores are determined as follows: 0 to 7 points indicate no symptoms; 8 to 10 points indicate suspected anxiety or depression; and 11 to 21 points indicate the definite presence of anxiety or depression. A score of 8 points is used as the starting point; that is, suspected and symptomatic people are considered to have anxiety or depression.
Statistical Analysis
SPSS version 26 (IBM SPSS Statistics) was used for data entry and analysis. Count data and ranked data are expressed as percentages. Comparisons between groups were performed using the chi-squared test or Fisher’s exact probability method, and comparisons of ranked data between groups were performed using the 2 independent-sample Wilcoxon rank-sum test. Measurement data with a normal distribution are expressed as X̅ ± s, comparisons between groups were performed by 2 independent-sample t tests, and comparisons between multiple groups were performed by analysis of variance. Measurement data that did not conform to a normal distribution are described by the median and interquartile range. The Wilcoxon rank-sum test was used for comparisons between 2 independent samples, and the Kruskal–Wallis test was used for comparisons between multiple groups. Logistic regression was used for multivariate analysis. P < 0.05 was considered statistically significant.
Results
Thirty-five patients, including 59 with congenital ear deformities, underwent noninvasive ear molding. One infant did not complete treatment because of the coronavirus disease; however, good therapeutic results were obtained after only 1 week of treatment. Follow-up was performed for up to 6 months after treatment.
Demographics of the 35 Patients
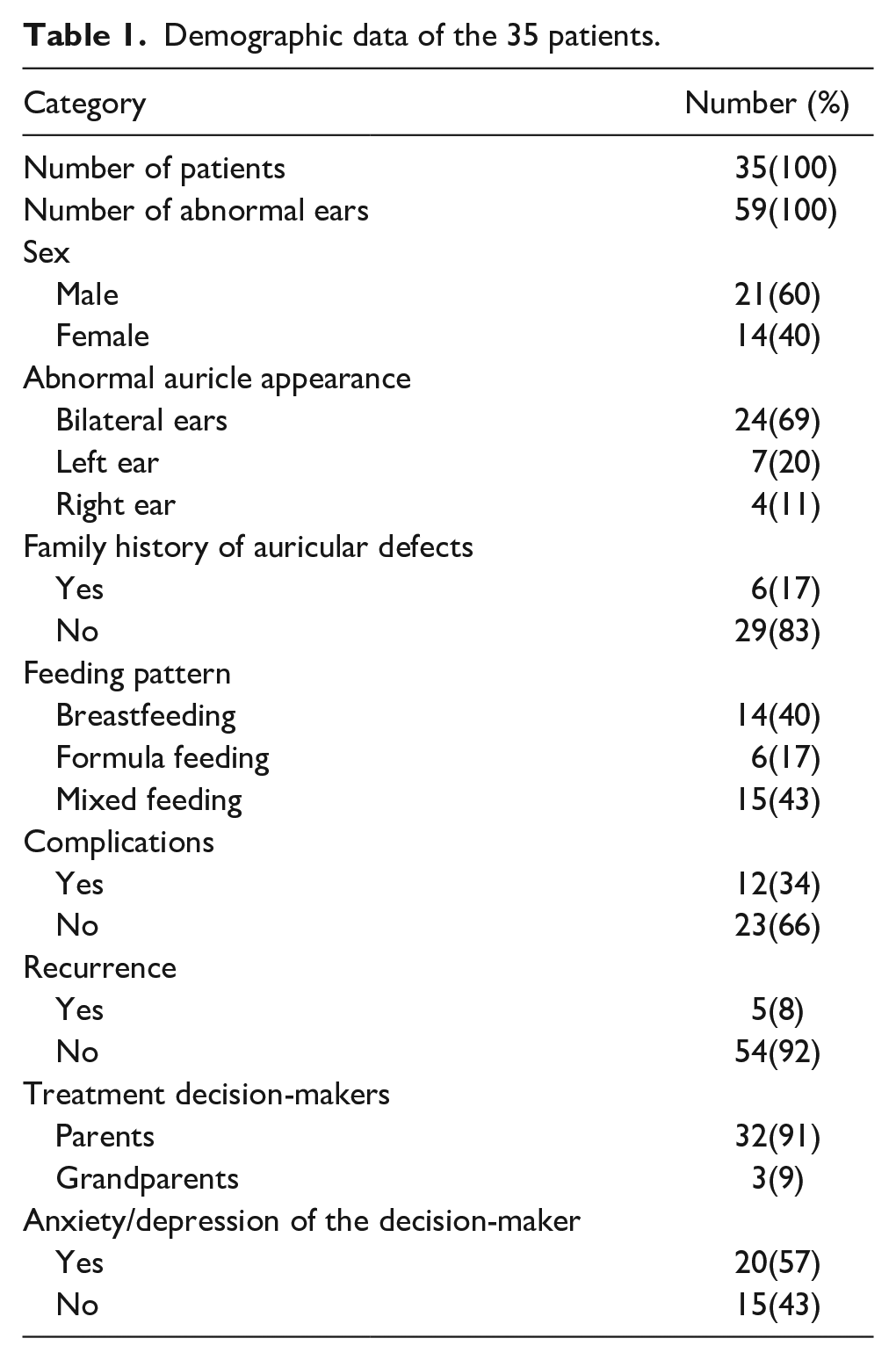
Of the 35 patients, 21 (60%) were male, and 14 (40%) were female. A total of 24 infants (69%) had bilateral auricular deformities, 7 infants (20%) had left auricular deformities, and 4 infants (11%) had right auricular deformities. A total of 29 newborns (83%) did not have a familial history of auricular deformities, and 6 infants had immediate family members with auricular deformities. Fourteen infants (40%) were breastfed, 6 infants (17%) were formulafed, and 15 infants (43%) were both breast- and formulafed during the treatment period. A total of 12 infants (34%) had complications during treatment, while 23 infants (66%) did not have any complications. Five ears (8%) were found to have rebounded at follow-up, while the other 54 ears (92%) had not. Treatment decisions were made by the parents of 32 infants (91%) and by the grandparents of 3 infants (9%). The treatment decision-makers for 20 infants (57%) had anxiety and depression, and those for the remaining 15 infants (43%) did not.
The detailed demographic data of the 35 patients are shown in Table 1.
Demographic data of the 35 patients.
Summary of Congenital Auricular Deformities
The 57 abnormal ears of the 35 patients were classified into 9 types of congenital auricular deformities, including cup ear (10 ears), lop ear (4 ears), helical rim deformity (18 ears), mixed auricular deformity (8 ears), conchal crus deformity (3 ears), microtia (3 ears), cryptotia (20 ears), Stahl’s ear (4 ears), and protruding ear (4 ears). Detailed data on the summary of congenital auricular deformities are shown in Figure 1.
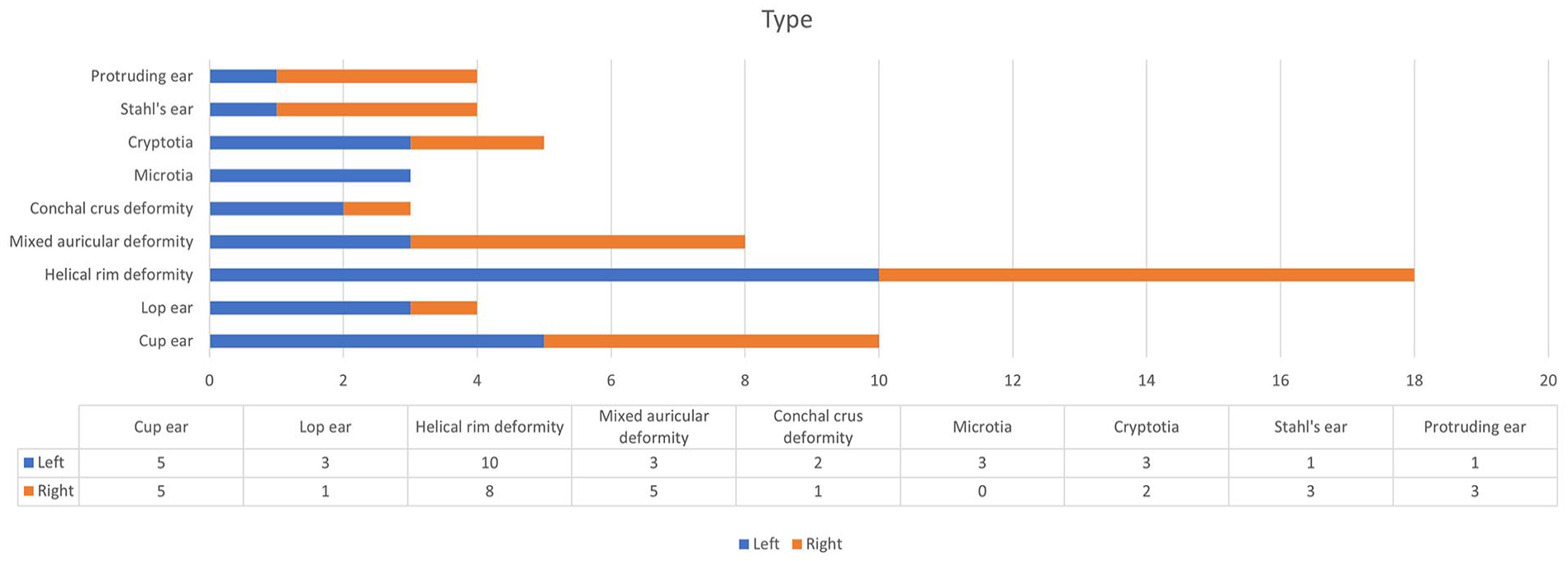
Summary of congenital auricular deformities.
Factors Affecting Outcomes
The factors affecting the outcomes were analyzed, including feeding patterns, types of auricular deformity, treatment initiation age, treatment cycles, and complications.
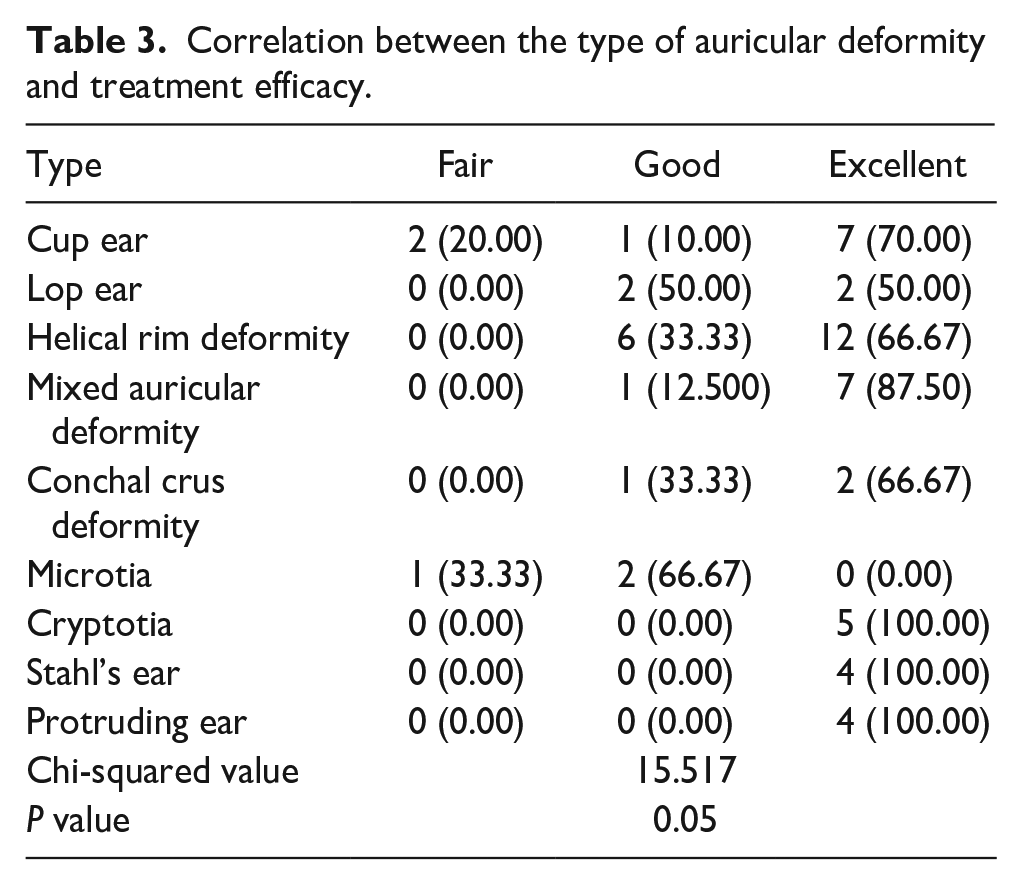
The results confirmed that the feeding pattern had no effect on the outcome, as shown in Table 2 (P > 0.05). There was a significant correlation between the type of auricular deformity and treatment efficacy, as shown in Table 3. The relationships between age at treatment initiation, treatment cycles, and complications and treatment effects are shown in Table 4. There was a significant correlation between the age at treatment initiation and treatment efficacy; the earlier the ear molding was started, the better the efficacy was. There was a significant correlation between the treatment cycle and treatment efficacy; a better efficacy was achieved with a shorter treatment time. However, complications did not appear to affect treatment efficacy.
Correlation between feeding patterns and treatment efficacy.

Correlation between the type of auricular deformity and treatment efficacy.
Correlation among age at treatment initiation, treatment cycles, and treatment complications and efficacy.
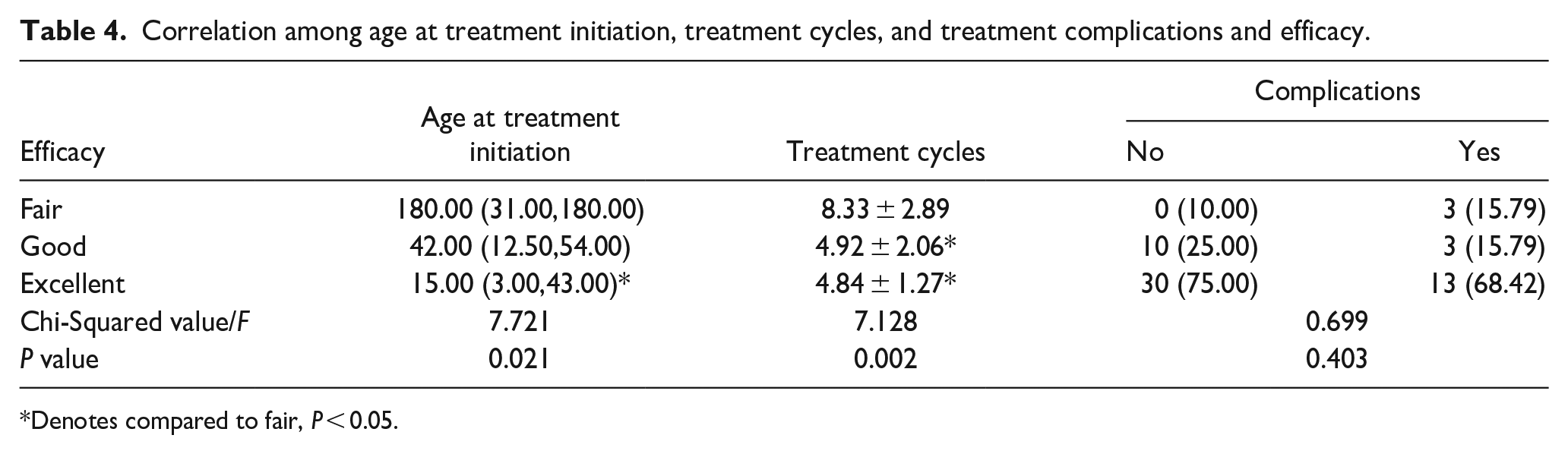
Denotes compared to fair, P < 0.05.
Efficacy for Different Types of Auricular Deformities
The typical auricular shapes of the 9 different kinds of congenital auricular deformities before and after ear molding therapy are displayed in Figures 2 and 3. A 6-month-old baby with a cup ear did not respond well to treatment, as shown in Figure 4. Although the auricles of 2 infants with microtia could not be completely corrected by ear molding, they achieved surprisingly good results, as shown in Figures 5 and 6.
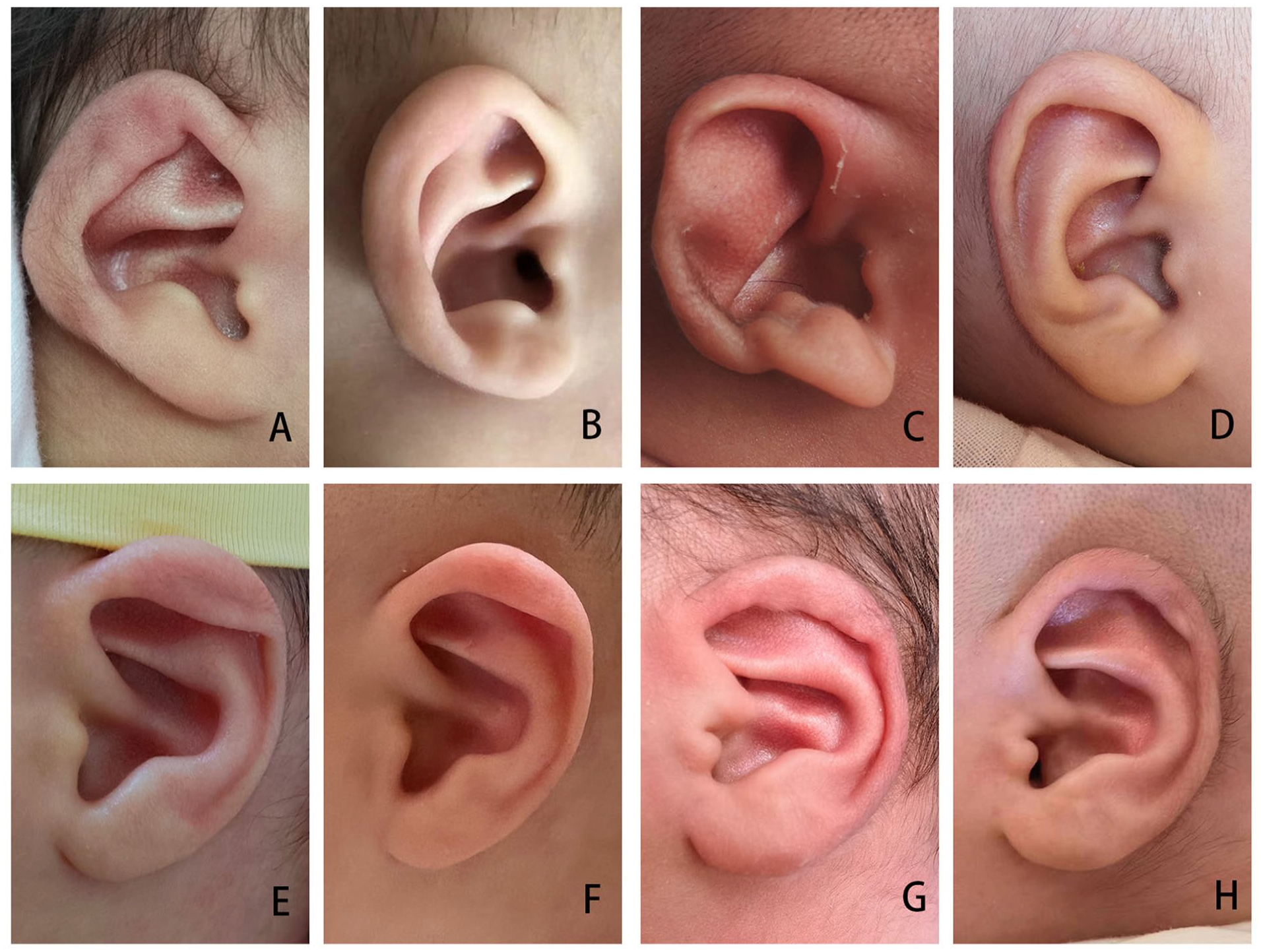
Examples of successful correction of different types of ear deformations. (A) and (B), Before and after treatment for cup ear. (C) and (D), Before and after treatment for Stahl’s ear. (E) and (F), Before and after treatment for lop ear. (G) and (H), Before and after treatment for a conchal crus deformity.
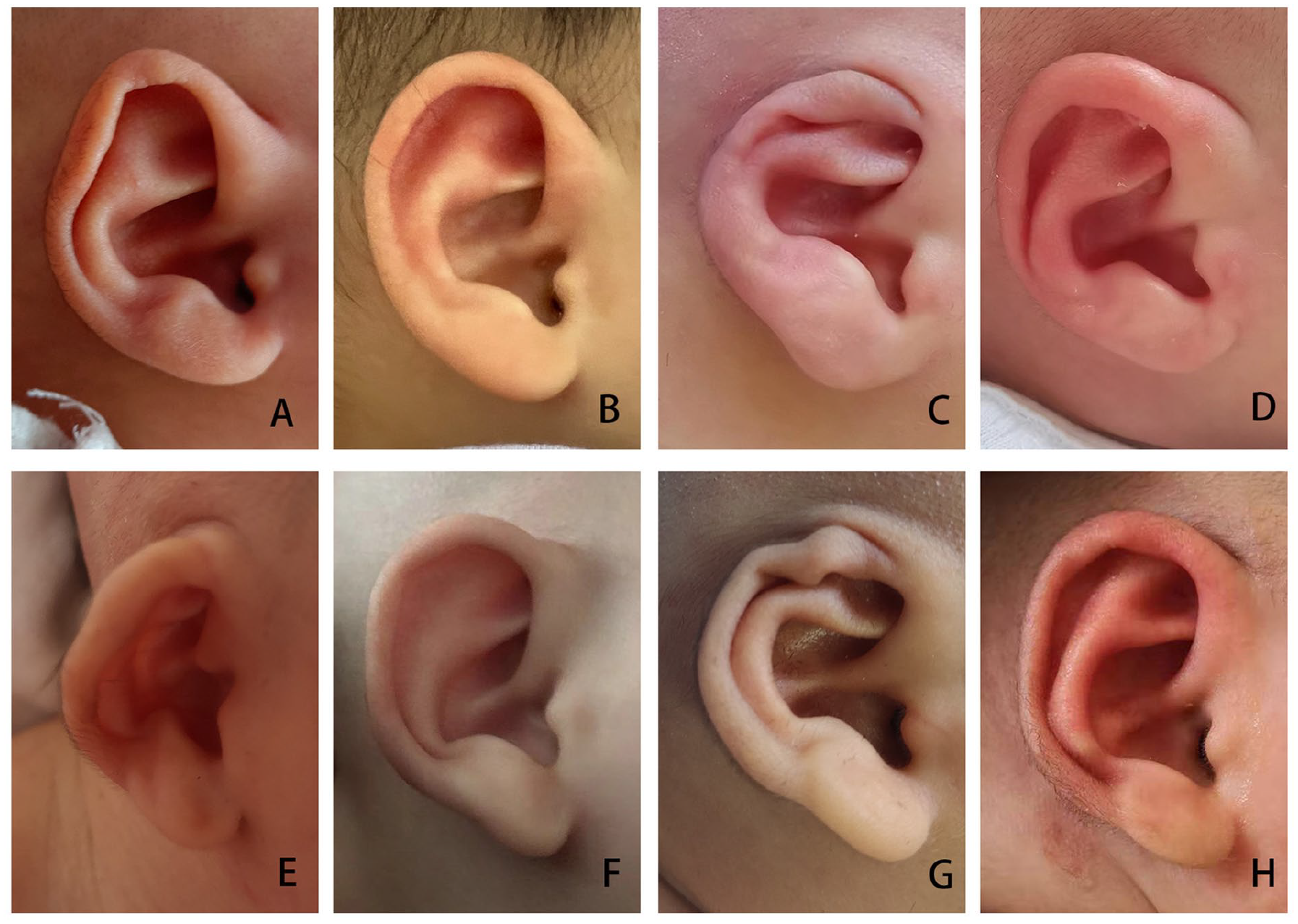
Examples of successful correction of different types of ear deformations. (A) and (B), Before and after treatment for helical rim deformity. (C) and (D), Before and after treatment for cryptotia. (E) and (F), Before and after treatment for protruding ear. (G) and (H), Before and after treatment for a mixed auricular deformity.
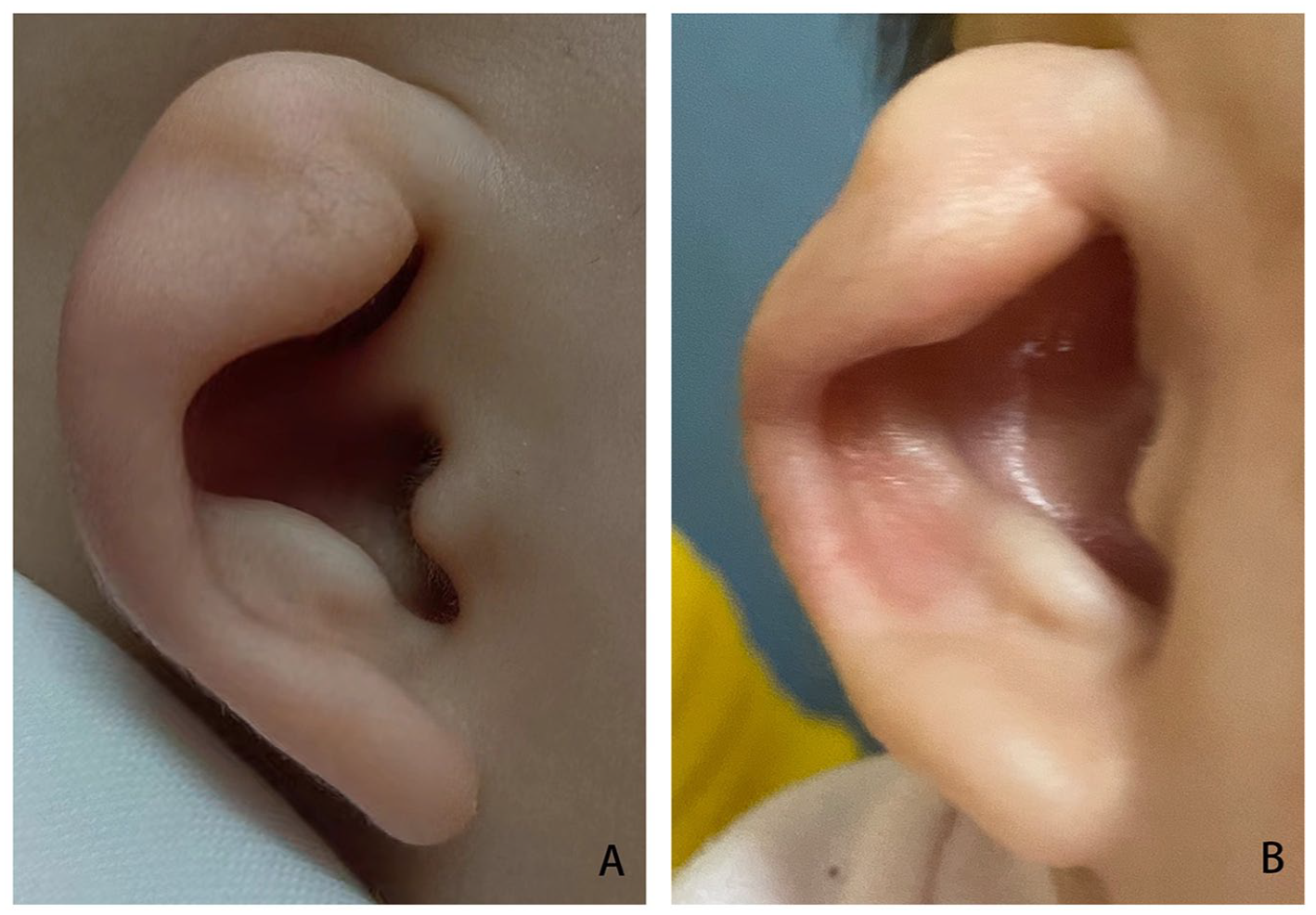
Example of a fair outcome in a 6-month-old baby with a cup ear. (A) and (B), Before and after treatment.

Microtia pre- (A) and posttreatment (B) with ear molding.

Microtia pre- (A) and posttreatment (B) with ear molding.
Factors Influencing the Time of Treatment Initiation
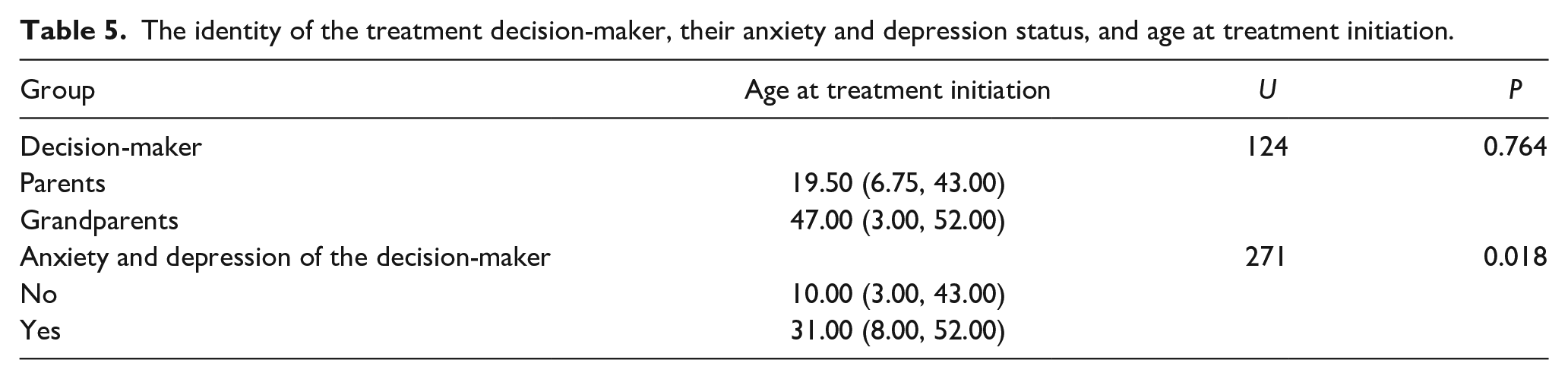
The effect of the treatment decision-makers and their anxiety and depression scores on the age at treatment initiation is shown in Table 5. The identity of the treatment decision-maker had no effect on the age at initial treatment (P > 0.05), but the anxiety and depression scores of the decision-maker had a significant effect (P < 0.05). Specifically, the greater the anxiety and depression scores of the decision-maker, the lower the treatment initiation age was.
The identity of the treatment decision-maker, their anxiety and depression status, and age at treatment initiation.
Discussion
The aesthetics of the auricle are composed of the location, size, and subanatomical structure. Any change in the auricle can cause auricular deformities, which can occur in one or both ears. Auricular deformities can be divided into deformations and malformations according to the absence of ear skin or cartilage tissue. 15 Some studies have suggested that weeks 5 to 9 of embryonic development are a critical period for the development of branchial arches. If embryonic development is affected by genetic factors or exogenous factors (drugs, radiation, viruses, etc.), auricle structural deformities may occur. Abnormal external forces on the auricle of the fetus in late pregnancy or during childbirth, as well as abnormal development and function of endogenous and exogenous muscles or cartilage, may cause morphological deformities of the auricle. Auricle morphology can be reshaped by external force in the neonatal period. The main reason is that the blood circulation of the newborn contains estrogen from the mother after birth. Estrogen can increase the amount of hyaluronic acid in the extracellular matrix, which gives the newborn cartilage a certain degree of extensibility and plasticity. 16
Since the 1980s, the concept of the nonsurgical correction of congenital auricular deformities has been widely recognized. Scholars have studied various materials and shapes of ear molding appliances and have achieved different results. Since the invention of the EarWell Infant Ear Correction System, many newborns with congenital auricular deformities have been treated, allowing pain from surgery and potential feelings of self-consciousness to be avoided. Ten years ago, nonsurgical correction of neonatal auricles was not widely performed in China. Many people may have been reluctant to attempt this treatment due to the traditional thinking that neonatal auricle deformities can heal on their own or be improved by the “pull and pull” method. As society continues to develop, congenital auricle deformities have gradually attracted the attention of parents and doctors. 17 Early auricle correction is also in line with the needs of parents. The convenience, safety, and effectiveness of nonsurgical correction have been recognized.
This study describes the application, therapeutic effect, and factors influencing ear molding in neonates with auricle deformities. In this study, the factors affecting the outcomes were analyzed, and the type of deformity, the age at treatment initiation, and the treatment period were shown to affect treatment efficacy.
Some studies have shown that breastfeeding can increase maternal estrogen level in breast milk, which can make ossification of the auricle cartilage difficult, and the correction effect is better. 18 In this study, there was no correlation between feeding patterns and treatment effects, which is similar to the study by Chan et al The results of these studies were consistent. 10
Some researchers have suggested that the age at treatment initiation and the duration of treatment are not related to treatment efficacy, 10 which contradicts the results of this study. This may be due to the selection of infants who were younger than 15 days in the other study, which is a smaller age range than that used in the current study (3-180 days), and the longer treatment period in the current study.
Previous studies have suggested that stable and permanent results can be obtained if the ear cartilage of the neonate is corrected before 6 months of age, 4 so follow-up until 6 months of age is recommended. However, some of the older infants in this study started treatment late, so they were followed up for 6 months after treatment; a hook or tape was fixed for 2 to 4 weeks after the end of treatment.
The finding that the type of ear deformity was associated with the treatment effect in this study is consistent with some previous studies, 3,10 but the present study also showed that noninvasive treatment has therapeutic value for mild microtia. After early noninvasive correction, although a normal auricle could not be achieved, these babies nevertheless demonstrated large improvements, and parental satisfaction was still very high. Additionally, future plastic surgery could provide a better skin and cartilage basis for further improvements.
Due to fetal tolerance to maternal antigens, the innate immune system of the newborn is suppressed, thus resulting in an enhanced response to neoantigens as the child ages. The immune system may play a role in the development of dermatitis, and older infants are more likely to develop comorbidity reactions. 19,20 However, the incidence of complications was low and did not affect treatment efficacy.
In this study, the psychological status of treatment decision-makers was evaluated to see if their psychological status led to early treatment, which has not been addressed in the previous literature. The more anxious the decision-makers were, the sooner treatment was initiated.
Due to ethical concerns, children with auricular deformities who did not receive noninvasive treatment were not included as a normal control group, so the self-healing rate of auricular deformities was not evaluated, and thus there was judgment bias in the treatment effect. An increase in the sample size and the inclusion of a normal control group will be considered for the next clinical investigation.
Conclusion
Ear molding is an effective nonsurgical method for the treatment of congenital auricular deformities in neonates. The earlier the neonatal auricle deformity is treated, the shorter the treatment time and the more ideal the clinical effect is. Early noninvasive treatment is valuable for microtia deformities. Early detection and parental awareness and education can help children receive treatment earlier and improve the treatment success rate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Heilong Jiang Postdoctoral Funds for scientific research initiation (Project No.: LBH-Q21119).