
Abstract
Objective:
This study aimed to investigate and analyze the anatomic characteristics of the retromaxillary cell (RMC) by using computed tomography (CT) images of paranasal sinuses and to improve its identification with ethmomaxillary sinus (EMS).
Methods:
The paranasal sinus CT scans of 441 outpatients or inpatients in our hospital from January 2018 to October 2018 were analyzed. The incidence of RMC, EMS, Haller cell, imaging anatomical characteristics, and morphological manifestations were observed via sinus CTs. The relationship of RMC and ipsilateral maxillary sinusitis was analyzed.
Results:
The incidence of RMC is 83.90% (740/882). The incidence of males and females was 83.81% (414/494) and 84.02% (326/388), respectively. The incidence of bilateral (72.79%, 321/441) was much higher than that of unilateral (22.22%, 98/441). The lateral extension of the RMC ranged from 1.18 to 13.31 mm, with an average of 6.10 ± 2.03 mm. The incidence of ipsilateral maxillary sinus opacification on the RMC sides and non-RMC sides has no significance difference (χ2 = .054, P = .459). The incidence of Haller cell and EMS decreased significantly in the presence of RMC (P < .01).
Conclusion:
The RMC is an anatomical variation originating from posterior ethmoid cells, which is commonly encountered in the clinic. The pneumatization of RMC is highly variable, and a bilateral is common. During endoscopic sinus surgery, it is necessary to carefully identify such an air cell to ensure the complete opening of the paranasal sinus during surgery.
Introduction
Endoscopic sinus surgery (ESS) is the most common surgical procedures applied in patients with chronic rhinosinusitis (CRS), for whom appropriate maximal medical therapy has failed. The efficacy and safety of surgery are influenced by many factors, such as the type of inflammation, intraoperative hemorrhage, surgical skills, mucosal protection, and perioperative management. 1 However, the surgeon’s understanding of paranasal anatomy, including various variant air cells, may play a crucial role in the success of surgery.2-4 A radiographical study by Gore et al 5 revealed that undissected ethmoid cells presented in 75% of patients who underwent revision ESS, and incomplete ethmoid sinus opening was an important reason for CRS recurrence after surgery.
The paranasal sinuses are a complex set of anatomical structures with marked individual differences. The numerous variation makes it a challenge for surgeon to identify and open all the cells precisely. 6 Of the 4 groups of paranasal sinuses, the ethmoid cells had the greatest variation. 7 There are many kinds of variation from the anterior ethmoid cells such as the agger nasi cells expanding forward, 8 the supraorbital ethmoidal cells9-10 expanding toward the supraorbit, and the Haller cells 11 beneath the orbit and above the maxillary sinus (MS) ostium. Similarly, the posterior ethmoid (PE) cells can also pneumatize spreading to surrounding areas. One of the most famous variation cells is the sphenoethmoidal air cells (Onodi cells), which is pneumatized superiorly and laterally to the sphenoid sinus. 12 When there is a PE cell occupying the superior part of the MS through the maxillary hiatus while draining to the superior meatus, located between the posterior part of the MS and the orbital floor, it is called the ethmomaxillary sinus (EMS). 13 Similarly, when a PE cell extends into the posterior part of the MS and the orbital floor, while spreading from outside the MS, it is called the retromaxillary air cells (RMCs). 14 It can also be called retromaxillary pneumatization of posterior ethmoid cells, 15 retromaxillary posterior ethmoid, 16 or retroantral ethmoid cells. 17 We find the name of RMC is most appropriate, which emphasizes the particular location of this cell.
Retromaxillary cell is an important anatomy variation that yet to be poorly recognized and frequently missed during ESS, especially for surgeons with less experience. Kuan et al 14 observed 69 patients with recurrent CRS who underwent repeated ESS, up to 73% of them had incomplete or no resection of the RMC. To our knowledge, few studies about RMC have been reported.14-17 The exact anatomic characteristics was still unclear and it is often confused to some other anatomical structure that is located between the MS and orbit such as EMS, Haler cell, and anterior extension of the sphenoid sinus. The distinction of EMS and RMC is ambiguous and vague particularly. Therefore, the anatomic characteristics of RMC and the more accurate distinction between RMC and EMS need to be further studied. In this study, we conducted an extensive work to observe and analyze the imaging anatomy of the RMC and improve the identification between RMC and EMS. We also investigate the correlation between RMC and ipsilateral maxillary sinusitis; since RMC is located on the posterior superior part of the MS, its excessive pneumatization may affect the MS drainage channel.
Materials and Methods
Materials
We conducted a retrospective analysis of paranasal sinus computed tomography (CT) scans that were obtained from outpatients or inpatients encountered in our hospital from January 2018 to October 2018. The CT scans were performed at the radiological department of the same hospital. A total of 441 cases were included. Of them, 247 were male and 194 were female, aged 40.52 ± 0.45 years (range: 18-85 years). The exclusion criteria were as follows: (1) age less than 18 years; (2) a history of sinus surgery, sinus trauma, or sinus tumors; and (3) invasive fungal sinusitis or craniofacial abnormalities (including craniofacial cleft, orbital hypertelorism, and craniostenosis). This study was approved by the institutional ethics committee of our hospital.
Spiral CT examination, Reconstruction, and Observation
The CT scan was performed using a Light Speed GE 64 slice spiral CT (GE Healthcare). The scanning range was from the superior margin of the frontal sinuses to the inferior margin of the maxillary alveolar process. The scanning layer thickness was 0.5 mm. The CT scans were obtained at 0.625-mm section thickness, a 2.5-mm interval, and the pitch was 0.969 mm. Viewing was performed using the GE Centricity Enterprise Web 3 (GE Healthcare) imaging system. The window width was adjusted to 2000 HU, the window position was 350 HU.
Standard of the RMC
According to Herzallah et al, 15 RMC was identified as follow: first, on the coronal plane, the PE air cells start was identified behind the basal lamella of middle turbinate (MT) by following the MT laterally attachment. Then, we identified the basal lamella of superior turbinate (ST). When the PE air cells behind the ST formed an inferolateral extension below the orbit following the lamina papyracea (LP) slope and in relation to the posterosuperior corner of the MS, it can be diagnosed as an RMC. Here, there is a septum between the posterior superior part of the MS and the posterior ethmoid sinus combine, which called the maxillary sinus-ethmoid septum (MES; Figure 1). On the coronal plane, a vertical line that passes along the innermost point of the MES was drawn (Figure 1). The part outside this line, which is located between the orbital floor and the MS, occupying the posterior superior part of the MS was exactly the RMC.
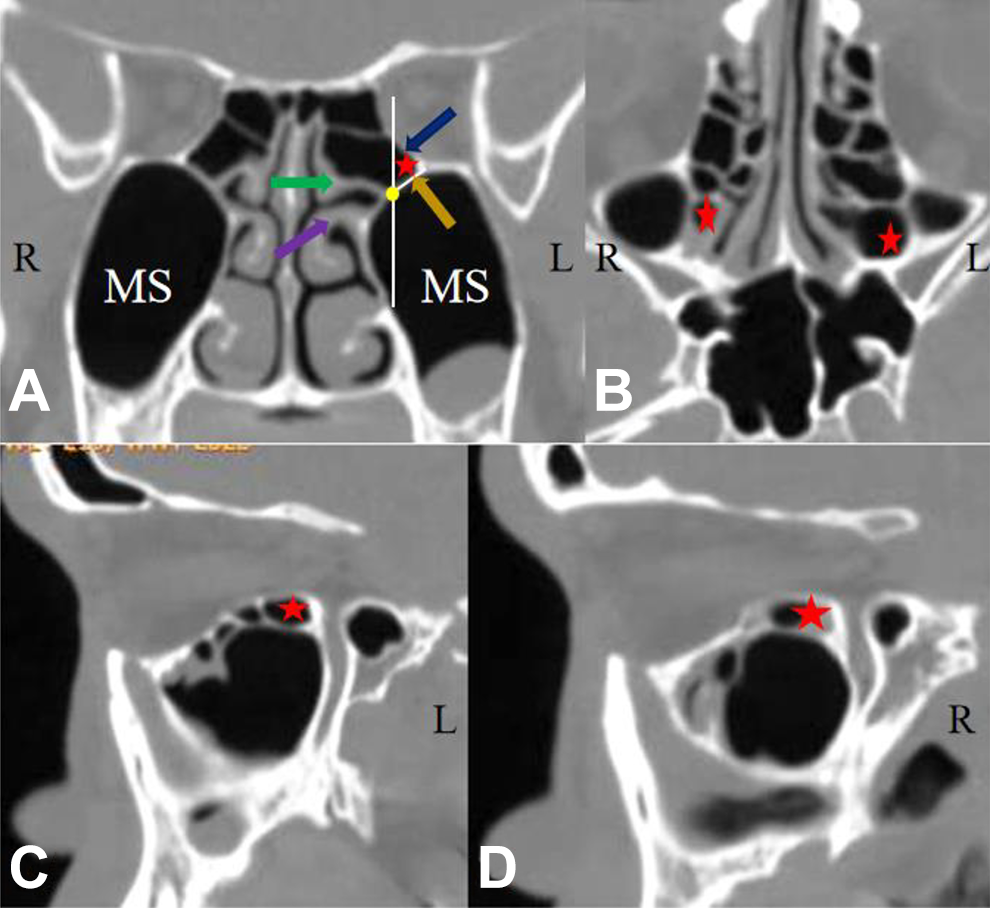
The determination standard of RMC. A, On the coronal plane, the PEs start was identified behind the basal lamella of MT (purple arrow) by following the MT laterally attachment. Then, we identified the basal lamella of ST (green arrow). When the PEs behind the ST formed an inferolateral extension below the orbit following the LP (blue arrow) slope and in relation to the posterosuperior corner of the MS, it can be diagnosed as an RMC (red star). Here, there is a septum between the posterior superior part of the MS and the PEs combine, which called the MES (orange arrow). On the coronal plane, a vertical line that passes along the innermost point (yellow point) of the MES (white line) was drawn. The part outside this line, which is located between the orbital floor and the MS, occupying the posterior superior part of the MS was exactly the RMC. B, On the coronal plane, bilateral RMC (red star); (C-D) left RMC and right RMC respectively (red star). LP indicates lamina papyracea; MES, maxillary sinus-ethmoid septum; MS, maxillary sinus; MT, middle turbinate; PEs, posterior ethmoid cells; RMC, retromaxillary cell; ST, superior turbinate.
Determination Standard of EMS
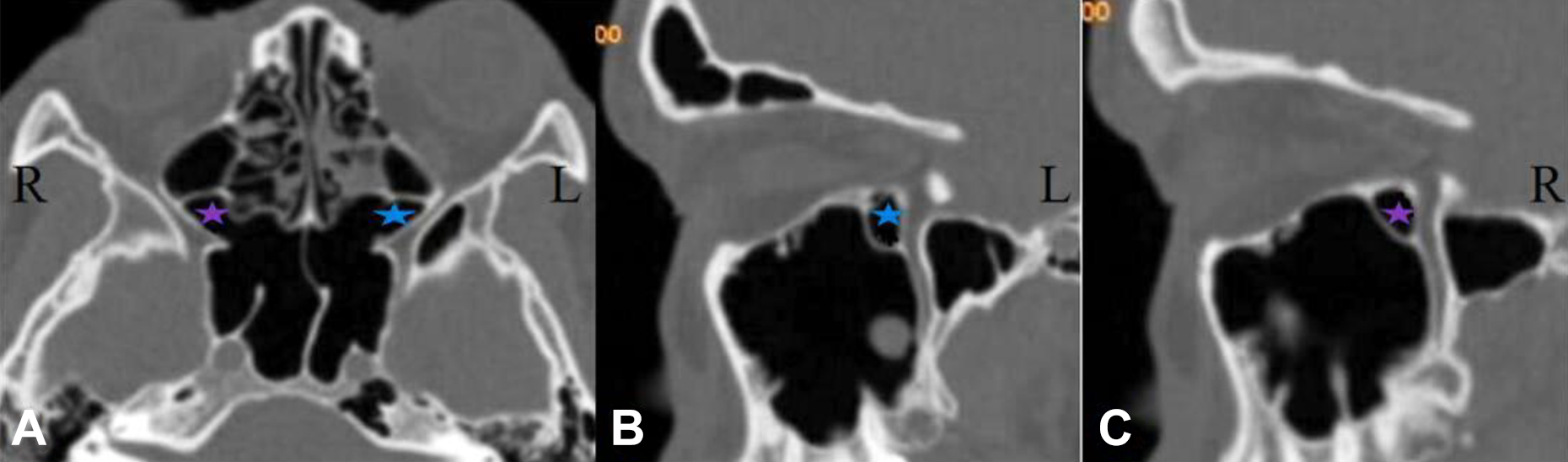
According to Sirikçi et al 13 and our observation, the diagnosis of EMS was made when the distinct pneumatization of the superior nasal meatus into MS through the maxillary hiatus, and occupying the superior part of MS. Its location was between the posterior part of the MS and the orbital floor (Figure 2).
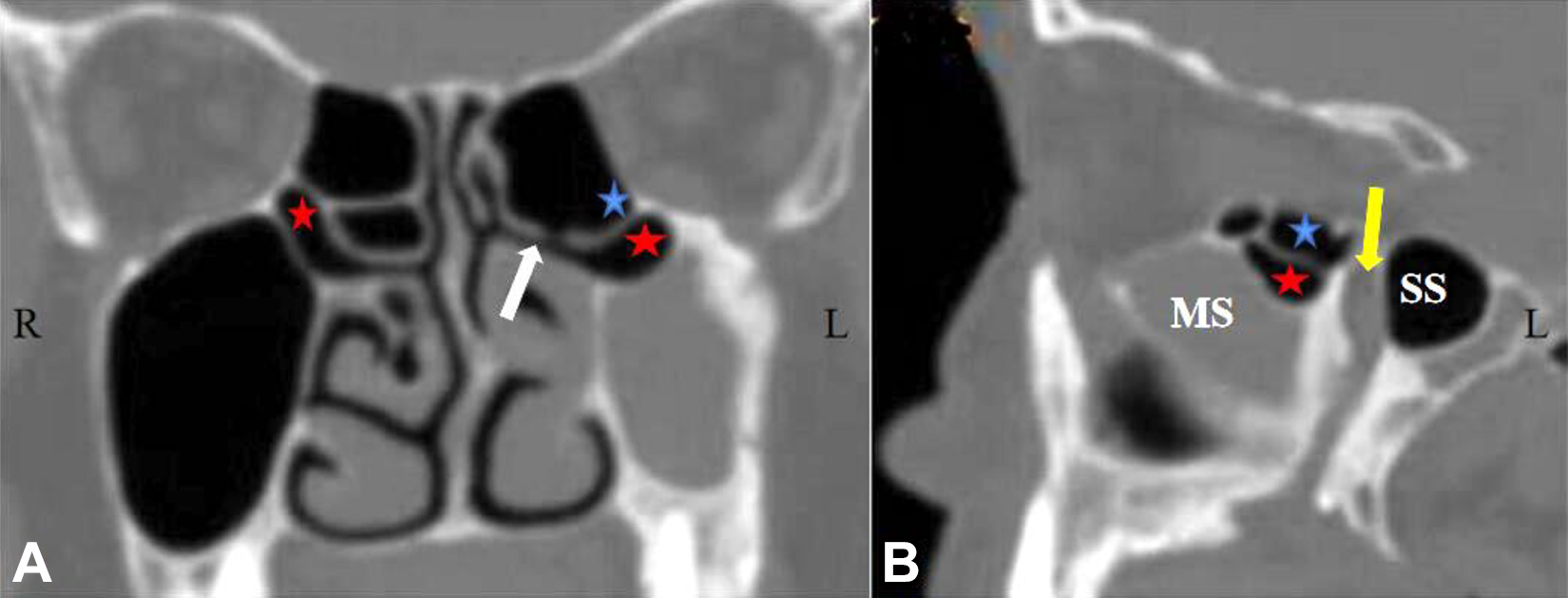
Ethmomaxillary sinus (EMS) and retromaxillary cell (RMC). A, On the coronal plane, there are 2 types of variant cells. Bilateral EMS (red star) and RMC (blue star) on the left. The drainage channel of EMS is clear (to superior nasal meatus), the drainage channel of RMC is not clear. B, On the sagittal plane, EMS (red star) and RMC (blue star), respectively, compared with RMC, the position of EMS is relatively ahead. White arrow: superior nasal meatus; yellow arrow: pterygopalatine fossa.
Degrees of RMC Lateral Extension
In the previous literatures, Herzallah et al 15 termed the vertical line that passes along the medial wall of the MS (MMS line) as the medial boundary of RMC. However, the medial wall of the MS is irregular, the MMS line is difficult to determine. So the vertical line that passes along the innermost point of the MES line was used as the medial boundary of RMC in this study. For the most obvious layer of pneumatization of the RMC on the coronal plane, the degree of lateral extension of RMC beyond the sagittal vertical line that passes along the innermost point of the MES line was then measured (Figure 3A-C). According to Herzallah et al, 15 the lateral extension of the RMC can be classified as 3 types: type I: <3 mm, type II: 3 to 6 mm, and type III: >6 mm.
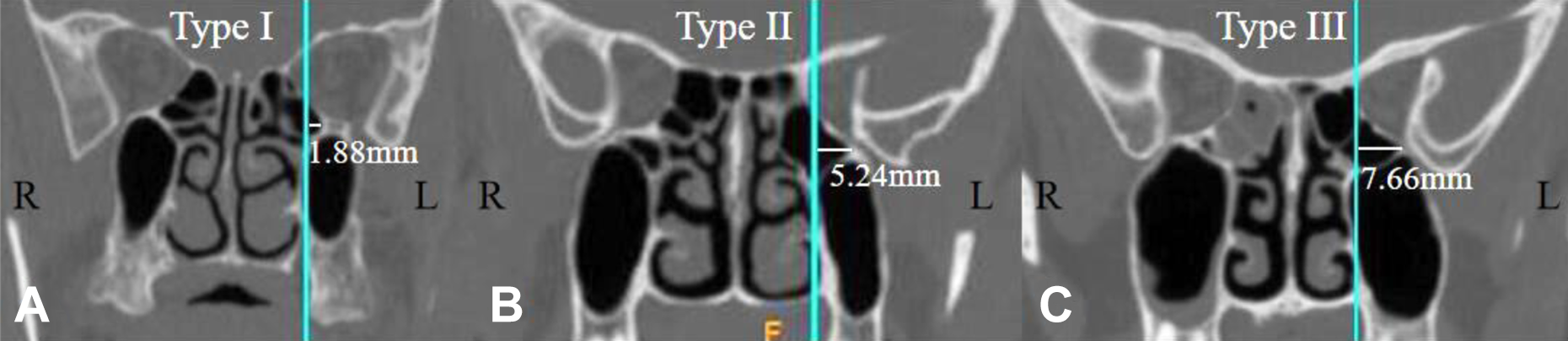
Degrees of retromaxillary cell (RMC) lateral extension. A-C, Type I, type II, and type III, respectively. C, The RMC on left was well pneumatization, and its lateral wall reached the lateral wall of maxillary sinus.
Coexisting Anatomical Variations of Paranasal Sinuses
Haller cell, EMS, and RMC are all the infraorbital cells that are originated from ethmoid cells. We observed the correlation between the appearance of RMC and the ipsilateral Haller cells and EMS (Figure 2).
Incidence of MS Opacification and RMC Opacification
Since the RMC is located on the posterior superior part of the MS, its excessive pneumatization may affect the MS drainage channel. Therefore, we observed and analyzed the correlation between the appearance of the RMC and the incidence of ipsilateral MS opacification. We also observed the incidence of RMC opacification. The degree of opacification was assessed using the Lund-Mackay (LM) score 18 : 0 grade = no abnormality, 1 grade = partial opacification, and 2 grade = total opacification (Figure 2).
Statistical Analyses
Statistical analysis was performed using SPSS version 22 (IBM Corp). Continuous variable data are presented as the mean ± SD. The Kruskal-Wallis test was used for comparisons between non-normal distributed data among groups, and the χ2 test was used for counting data. A significance level of .05 was used for all comparisons.
Results
Incidence of RMC
Of the 441 (882 sides) patients, 740 (419 cases) sides had an RMC, with an incidence of 83.90% (740/882). There were 414 (238 cases) sides with RMC among males and 326 (181 cases) sides among females. The incidence was 83.81% (414/494) and 84.02% (326/388), respectively. Of the 419 cases of RMC, 321 were bilateral and 98 were unilateral. The incidence of bilateral RMC (72.79%, 321/441) was much higher than that of unilateral RMC (22.22%, 98/441).
Distinction Between RMC and EMS
The most important distinction point between RMC and EMS (Table 1) is the drainage channel; on the coronal plane of the CT scan, the EMS has clear drainage channel, whereas RMC do not (Figure 2A). Other differentiations are as follows: (1) Source: RMC originated from PEs, whereas EMS is from the distinct pneumatization of the superior nasal meatus into MS. So RMC is always behind the ST basal lamella, and the EMS is anterior to the ST basal lamella but behind the MT basal lamella; (2) location: Both EMS and RMC are located on the posterior part of the MS, but the position of EMS is relatively ahead (Figure 2B). Compared with EMS, the position of RMC is relatively concealed; (3) relation with the MS: EMS enters into the MS whereas RMC is out of the MS, so the septum between EMS and orbit is the superior wall of maxillary while that between RMC and orbit is the wall of RMC, but this point sometime is difficult to be distinguished on CT scans; (4) pneumatization range: The pneumatization range of RMC is often limited to the infraorbital region and behind the MS, but the pneumatization range of EMS shows great variability, which can expand downward, even extending to the entire posterior wall of the MS, the inferior wall of the EMS can also appeared in the alveolar process. 19
Differences Between EMS and RMC.
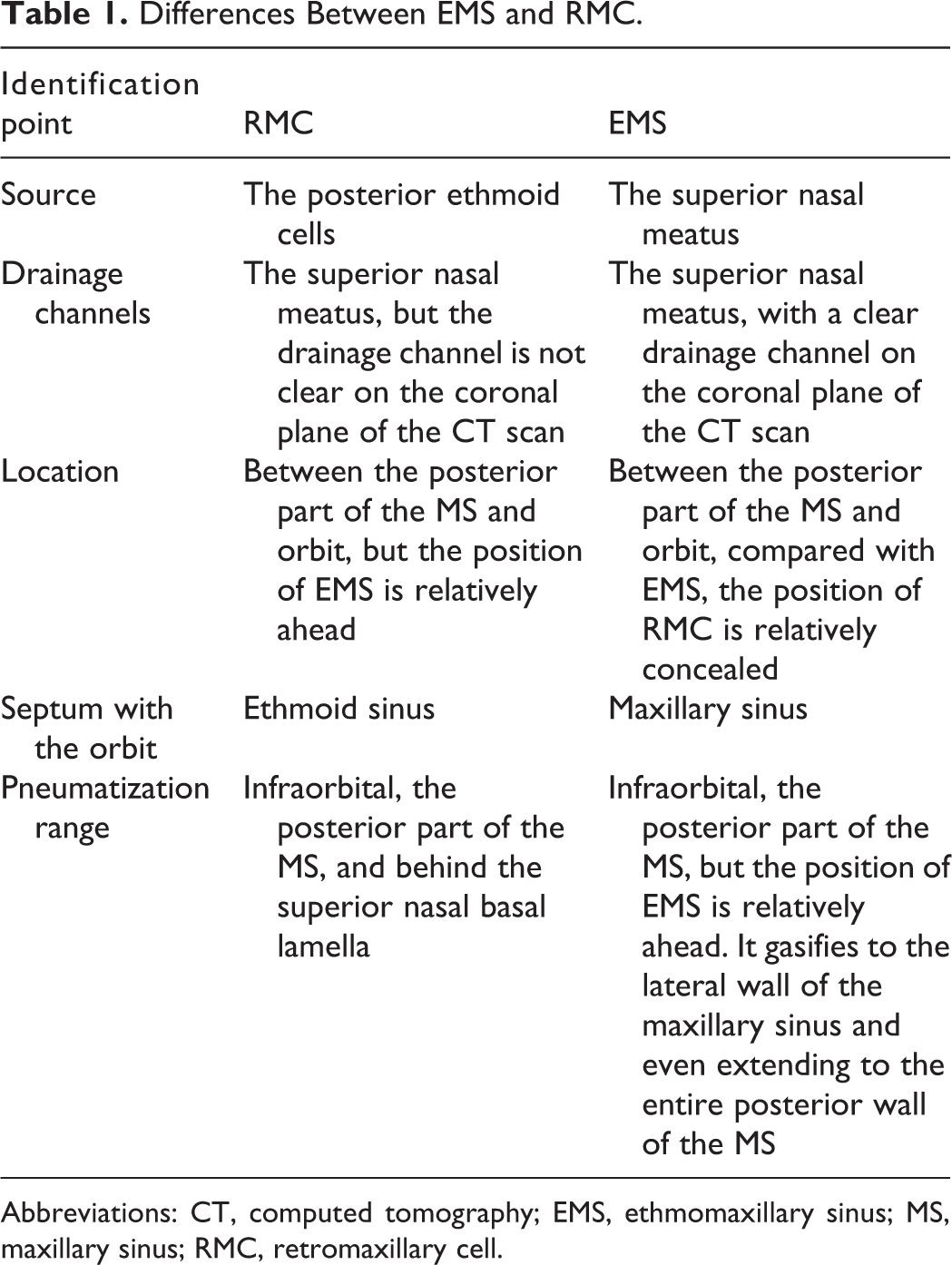
Abbreviations: CT, computed tomography; EMS, ethmomaxillary sinus; MS, maxillary sinus; RMC, retromaxillary cell.
Anatomical Characteristics of RMC
According to Herzallah et al 15 and our observation, the anatomical characteristics of an RMC are as follows: (1) It originates from the PEs; (2) it is on the extramaxillary sinus area, not entering the MS; (3) on the coronal plane, its upper anatomical boundary is the orbital floor, and the lower boundary is the MES, the lateral boundary is the LP. When it undergoes well pneumatization, its lateral wall may reach the lateral wall of MS (Figure 3C); (4) on the sagittal plane, we can see it is located between the posterior superior part of the MS and the orbital floor but outside the MS. It is also abutted to the pterygopalatine fossa and the superior part of the MS, and the pterygopalatine fossa are separated by RMC; on the axial plane, we can see it is abutted to sphenoid sinus; therefore, it sometime need to be distinguished with the anterior extension of the sphenoid sinus (Figure 4).
Anterior extension of the sphenoid sinus. A, On the axial plane, there exist bilateral anterior extension of the sphenoid sinus (blue star and purple star); (B-C) on the sagittal plane, anterior extension of the sphenoid sinus is on the left (blue star) and right (purple star), respectively. Sometimes, it is easy to mistake the anterior extension of the sphenoid sinus as retromaxillary cell on the coronal and sagittal plane. In this case, observation on the axial plane is necessary.
Degrees of RMC Lateral Extension
The degrees of lateral extension of the RMC ranged from 1.18 to 13.31 mm, with an average of 6.10 ± 2.03 mm. Of them, the degree of lateral extension for males ranged from 1.18 to 13.31 mm, with an average of 6.21 ± 2.12 mm, and that for females ranged from 2.42 to 12.30 mm, with an average of 6.00 ± 1.93 mm. Of the 740 sides of RMC, 38 (5.14%) sides were classified as type I, 355 (47.97%) as type II, and 347 (46.89%) as type III (Table 2).
Coexisting Anatomical Variations.
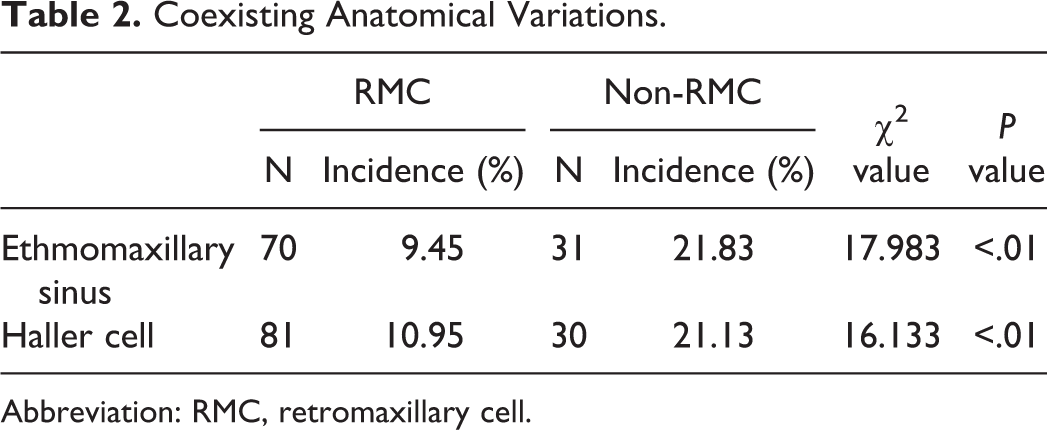
Abbreviation: RMC, retromaxillary cell.
Coexisting Anatomical Variations
Ethmomaxillary sinus
Of the 740 sides with RMC, 70 coexisted with EMS, giving an incidence of 9.45% (70/740). For the 142 sides without an RMC, 31 had EMS (21.83%, 31/142). The incidence of EMS on the non-RMC sides is higher than RMC sides (χ2 = 17.983, P < .01).
Haller cell
Of the 740 sides with RMC, 81 coexisted with Haller cells, giving an incidence of 10.95% (81/740). For the 142 sides without an RMC, 30 had Haller cells (21.13%, 30/142). The incidence of Haller cell on the non-RMC sides is higher than RMC sides (χ2 = 16.133, P < .01; Table 3).
Condition of Ipsilateral Maxillary Sinus Opacification.
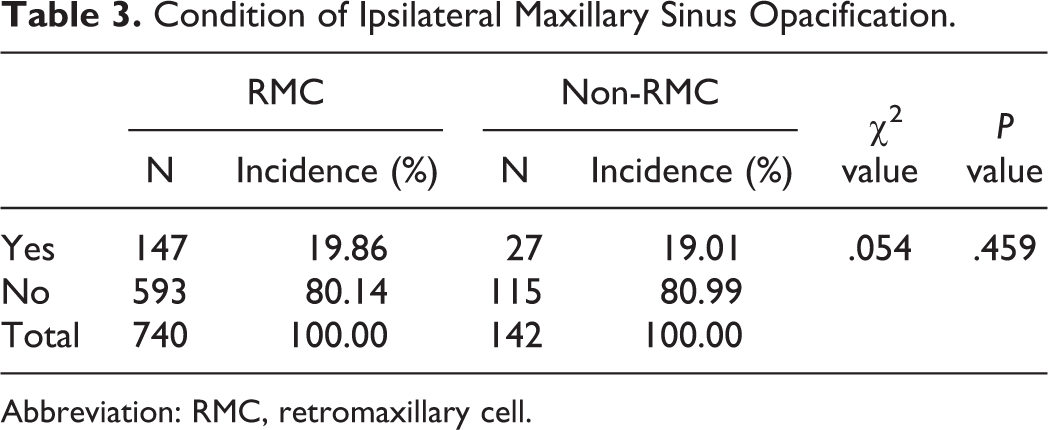
Abbreviation: RMC, retromaxillary cell.
Incidence of MS Opacification
Of the 740 sides of RMC, 147 coexisted with ipsilateral MS opacification, giving an incidence of 19.86% (147/740). For the 142 sides without the RMC, 27 sides had MS opacification, giving an incidence of 19.01% (27/142). The incidence of ipsilateral MS opacification on the RMC sides and non-RMC sides has no significance difference (χ2 = .054, P = .459). According to the LM score, 593 sides had a score of 0, 128 had a score of 1 and 19, and had a score of 2. The lateral extension had no difference between 0 score, 1 score, and 2 score (H = 2.867, P = .238).
Incidence of RMC Opacification
Of the 740 sides of RMC, 98 sides had RMC opacification, giving an incidence of 13.24% (98/740). According to the LM score, 642 sides had a score of 0, 83 had a score of 1 and 15, and had a score of 2. There has no difference between RMC opacification and MS opacification (χ2 = .129, P = .419).
Discussion
The anatomical structures of paranasal sinuses are complex and encompass various types of anatomical variations. The ethmoid cells are highly variable in form and structure, as well as in number. 7 Retromaxillary cell is one of the variant air cells, which originates from the excessive pneumatization of the PEs and appears in the region of retromaxillary and orbital floor. In our study, 441 (882 sides) cases of sinus CTs were observed and analyzed, and a total of 740 (419 cases) sides were found to have an RMC, giving an incidence of 83.90% (740/882). Herzallah et al 15 reported that the incidence of RMC was 79.40%. Liu et al 16 analyzed 103 sinus CTs and found that the incidence of RMC was 74.30%. Chapurin et al 17 indicated that the incidence of RMC was 16%, but the CT pictures provided in his paper show the EMS. The difference may be due to the ethnicities, the number of samples, and the different criteria of identifying the RMC. In our study, we used the vertical line that passes along the innermost point of the MES line as the medial boundary of RMC (Figure 1).
There are 3 kinds of variant cells formed by ethmoid cells pneumatizating along the LP to the orbit, namely, Haller cell, EMS, and RMC. An RMC can coexist with Haller cell and EMS (Figure 2), the incidence of Haller cell and EMS decreased significantly in the presence of RMC. These 3 types of cells are often dedifferentiated in identification, especially when excessive pneumatization. Haller cell can usually be easily distinguished from RMC because it is originated from anterior ethmoids while RMC from posterior ethmoid. But the definition of EMS and RMC was indistinct and ambiguous. Several points on the differentiation of EMS and RMC had been presented by Liu et al 19 : (1) drainage channel: On the coronal plane of the CT scan, the EMS has clear drainage channel, whereas RMC do not. This is the most important identification point (Figure 2A); (2) relation with the MS: EMS enters into the MS, whereas RMC is out of the MS, so the septum between EMS and orbit is the superior wall of maxillary while that between RMC and orbit is the wall of RMC, but this point sometime is difficult to be distinguished on CT scans; (3) pneumatization range: The pneumatization range of RMC is often limited to the infraorbital region and behind the MS, but the pneumatization range of EMS shows great variability, which can expand downward, even extending to the entire posterior wall of the MS, the inferior wall of the EMS can also appeared in the alveolar process. Other than these criterion, in this article, we tried to distinguish the 2 types of cell based on the source of the cells, which may be a more clearly standard and can be more easy in practice. The RMC originated from PEs, whereas EMS is from the distinct pneumatization of the superior nasal meatus into MS. So the RMC is always behind the ST basal lamella, and the EMS is anterior to the ST basal lamella but behind the MT basal lamella. The EMS and RMC are located on the posterior part of the MS, but the position of EMS is relatively ahead (Figure 2B). Compared with EMS, the position of RMC is relatively concealed and is easy to be ignored during ESS.
It has been described that the anterior extension of the sphenoid sinus formed retromaxillary pneumatization (Figure 4).20-23 In such cases, the intervening wall between the maxillary and sphenoid sinuses was termed the sphenomaxillary plate, and the occurrence of this variation was 11% to 16% of cases20,22-23 and 12.34% in our study. This result shows that RMC is, by far, more common than the sphenoid one (83.90% vs 12.34%). This differentiation is important since sphenoid retromaxillary extension can be spared in cases of PE disease. It also has to be mentioned that retromaxillary pneumatization should also be differentiated from the lateral sphenoid recess, which is rather a pneumatization in the pterygoid base behind the upper part of the pterygopalatine fossa. 15
An RMC can coexist with an EMS and Haller cell. The incidence of Haller cell and EMS decreased significantly in the presence of RMC. In other words, the existence of RMC affects the pneumatization of EMS and Haller cell. This may imply that the variations of the ethmoid sinuses have influence on each other.
Though RMC is very common, the obscured position behind the MS and the close relationship with the LP make it potentially to be missed in the initial dissection. Attention should be paid to identify the cell during ESS and protecting the orbital during the removal and opening of such an air cell (Figure 5A-B). Kuan et al 14 observed 69 patients with recurrent CRS who underwent repeated functional endoscopic sinus surgery, up to 73% of them had incomplete or no resection of the RMC. Therefore, they suggested that when opening the ethmoid cells, such cell should be adequately and carefully removed to reduce the recurrence of CRS after surgery.
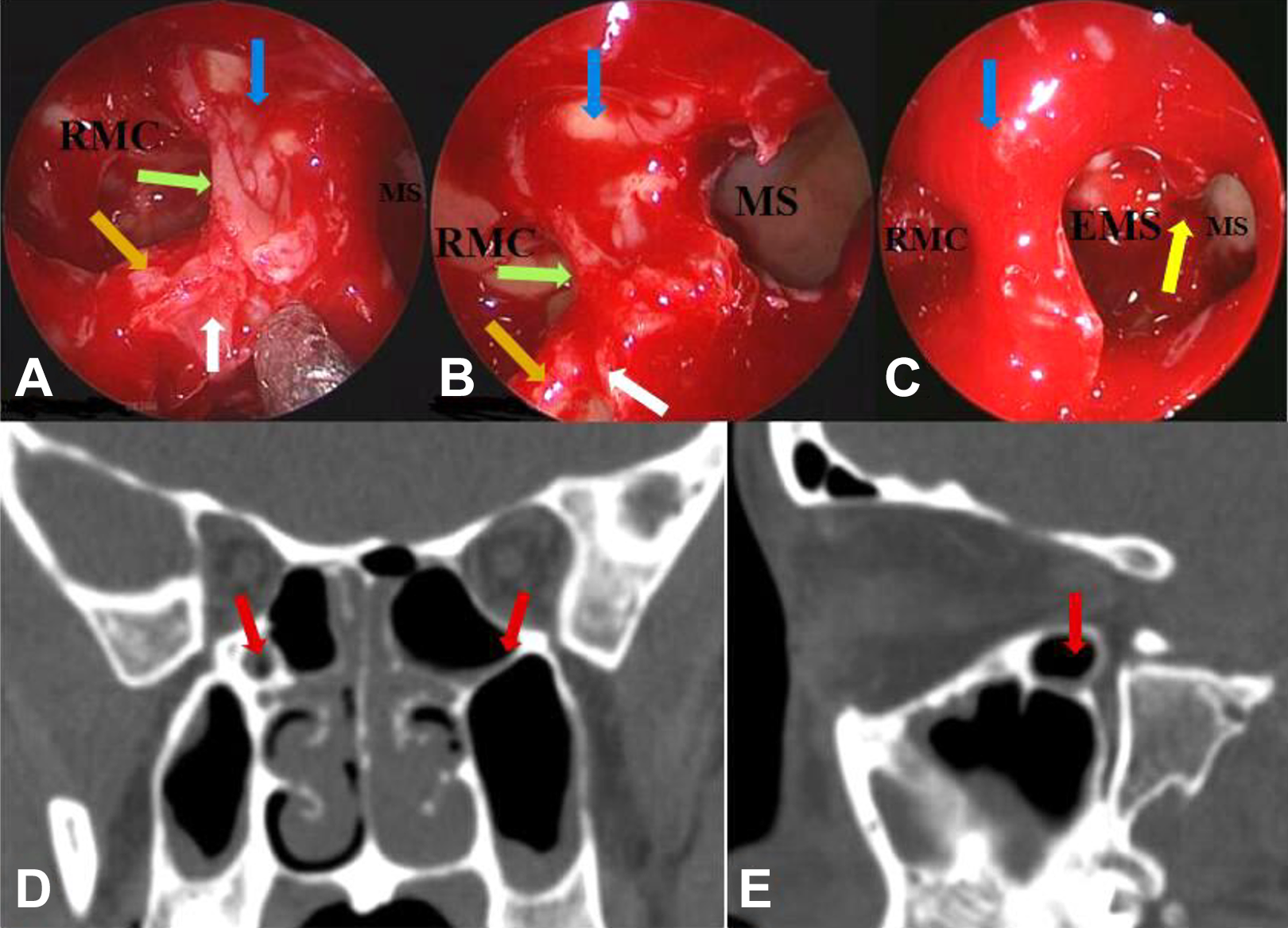
Endoscopic findings. A, B, D, and E, The same patient, with 0° endoscopic field of view and 70° endoscopic field of view, respectively; (C) another patient, left MS, EMS, and RMC. D and E, Left RMC (red arrow) seen on the coronal and sagittal plane, respectively. In ESS, when there is a well-pneumatization EMS, it is necessary to remove the EMP as much as possible to fuse the EMS and the MS and ensure the MS was completely opened. However, since RMC has no obviously effect on the drainage of MS, we usually do not need to completely remove MES, it just needs to open the RMC, and there is no need to fuse the RMC and MS into a large cavity. White arrow: middle turbinate basal lamella; orange arrow: superior turbinate basal lamella; blue arrow: lamina papyracea; green arrow: maxillary sinus-ethmoid septum (MES); yellow arrow: ethmomaxillary plate (EMP), it is the bony septum between the EMS and MS. EMS indicates ethmomaxillary sinus; RMC, retromaxillary cell; MS: maxillary sinus.
Retromaxillary cell can be classified into 3 types based on the lateral extension (Figure 3), type I: <3 mm, type II: 3 to 6 mm, and type III: >6 mm, which reflect the degree of RMC pneumatization. 15 In other words, type I is a relatively shallow pneumatization, type II is the median pneumatization, and type III is a deep RMC. Of the 740 sides of RMC of this study, the incidence of type I, type II, and type III were 5.14%, 47.97%, and 46.89%, respectively. In the study of Herzallah et al, 24% were type I, 49.5% were type II, and 26.5% were type III. It seemed that the median pneumatization is the most common, though the degree of pneumatization of RMC might be affected by ethnicities. For type I RMC, it is easy to identify and open during operation. It can be completely opened using regular sinus instruments under the 0° endoscopic field of view. Type III RMC is well pneumatization and not easy to be completely opened, especially when there exist opacification. Therefore, Kerrison nipper, curette, and angled bite forceps are generally required for opening. If necessary, other auxiliary equipment such as Chain forceps and angled grinding drills can be used to open this cell as possible as possible. Type II RMC is between type I and type III, and its opening skills depend on the condition during operation.
Existing studies had not explored the relationship between RMC and ipsilateral MS opacification. Previous study 13 on EMS had shown that the presence of EMS is related to the occurrence of maxillary sinusitis. Though RMC is also located on the posterior superior part of the MS, our results showed that the incidence of ipsilateral MS opacification did not change in the presence of RMC; moreover, there was no significance relationship between the degree of MS opacification and the pneumatization degree of RMC. These may indicated that the pneumatization of RMC will not affect the MS drainage channel. Our results also showed that there was no significant difference between RMC opacification and MS opacification. This may be because the source and location of these 2 types of air cells are different, and they do not affect each other’s drainage channels.
There are still some limitations of the study. In addition to the above 2 types of anatomical variations, RMC can also coexist with other anatomical variations, such as MS hypoplasia, nasal septal deviation, and concha bullosa, but we have not analyzed yet the correlation between them, which requires further research in the future to improve its anatomical characteristics. And a larger sample is also necessary.
Conclusion
Retromaxillary cell is an anatomical variation originating from posterior ethmoid cells, and it is commonly encountered in the clinic. The RMC is highly variable, and a bilateral RMC is common. During ESS, it is necessary to carefully identify such an air cell to ensure the complete opening of the paranasal sinus during surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This study was supported by grant from the National Natural Science Foundation of China (no. 81371070).