
Abstract
Here, we present a rare case of middle ear adenoma in a 58-year-old female, which uniquely presented as an unstable open cavity after an endaural atticoantrotomy. Immunohistochemistry confirmed that the tumor produced endocrine and exocrine secretions. The tumor was radically surgically removed.
Introduction
Middle ear adenoma (MEA) is a benign tumor, which originates from the mucosa in any part of the middle ear. It is very rarely diagnosed: to date, only 50 cases in adults and 4 in children have been reported.1,2 Middle ear adenomas typically occur in patients between 20 and 50 years of age. There is no significant sex predominance. 3 Here, we present a case of MEA, which uniquely resembled a late surgical complication.
Case Report
A 58-year-old female was referred to the Department of Otorhinolaryngology and Head and Neck Surgery of our tertiary referral hospital. She complained of recurrent otorrhea and persistent granulated tissue in the cavity of the right ear, which had lasted for 5 months. The condition was considered a late surgical complication. The patient had undergone an endaural atticoantrotomy 17 years prior, due to chronic otitis media with a cholesteatoma. After the atticoantrotomy, the cavity had healed and was stable, except one uncomplicated acute infection, which was treated with antibiotic ear drops. However, after the surgery, she developed severe conductive hearing loss on the right side. She retained normal hearing on the left side.
Computed tomography scans of the temporal bones showed a soft tissue mass, which completely filled the space of the former tympanic cavity. The remaining ossicles were embedded in the mass. The mastoid cell on the right side is completely blurry. There was no bone erosion (Figure 1).
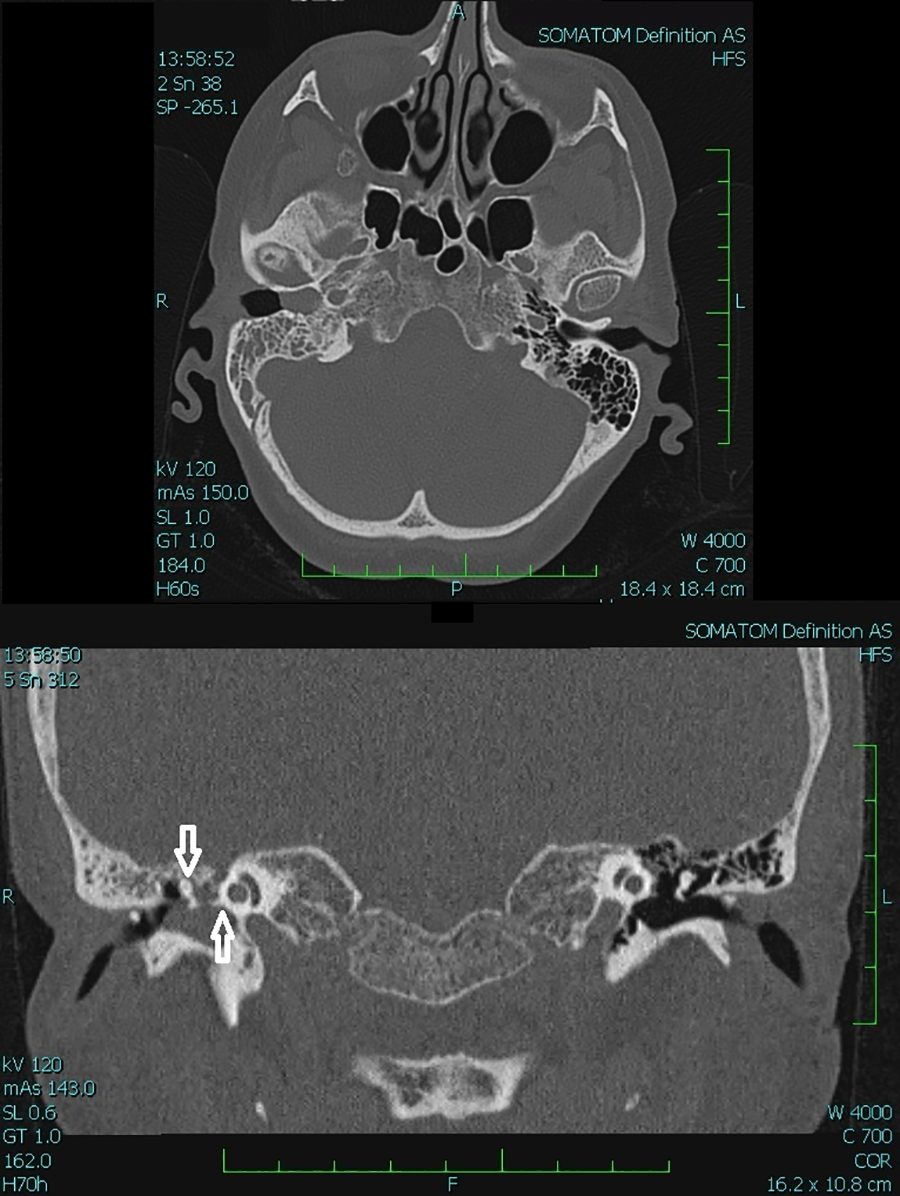
Axial (upper image) and frontal (lower image) computed tomography (CT) scan of the middle ear adenoma (MEA). A soft tissue mass completely fills the space of the former tympanic cavity and the medial part of the external auditory canal on the right. The mastoid cell on the right side is completely blurry, but there is no bone erosion. A soft tissue mass completely encases the remaining ossicles (arrows) on the right side (R).
An otomicroscopic examination showed mucous secretion in the external auditory canal, thickened vascularized tissue in the place of the tympanoplasty, and atypical granulated tissue at the base of the cavity (Figure 2), suggestive of inflammatory granulated tissue. After a month of local antibiotic therapy, the symptoms were alleviated, and the otorrhea disappeared, but the granulation-like tissue persisted without changing size. To exclude a tumor, a biopsy was performed, and a histopathological examination indicated an adenoma with high proliferative activity. Microscopically, solid and glandular growth patterns were observed (Figure 3). Immunohistochemistry showed positive staining for synaptophysin and chromogranin (Figure 4).
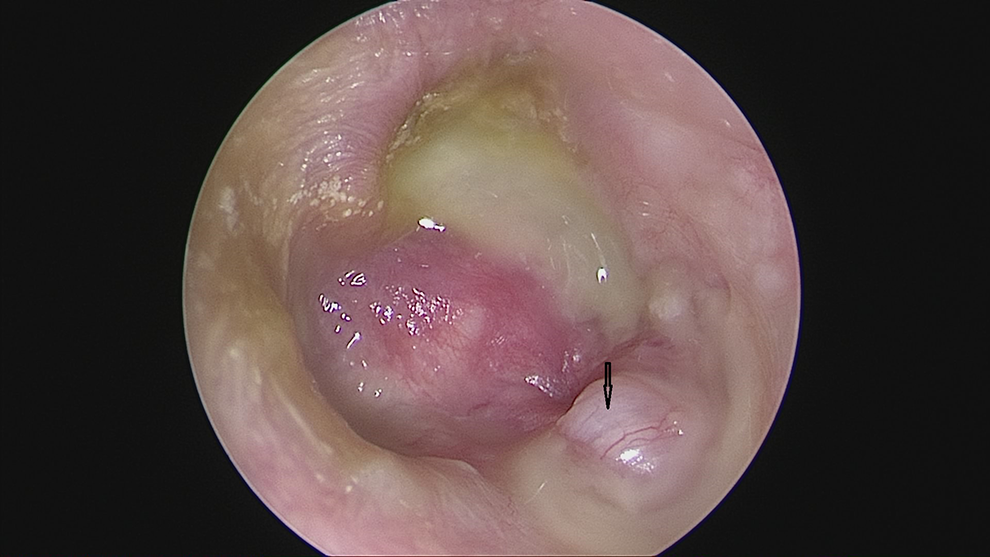
Preoperative endoscopy of the right ear. Note the mucous secretion, thickened vascularized tissue at the location of a tympanoplasty, and atypical granulated tissue at the base of the trepanation cavity (arrow).
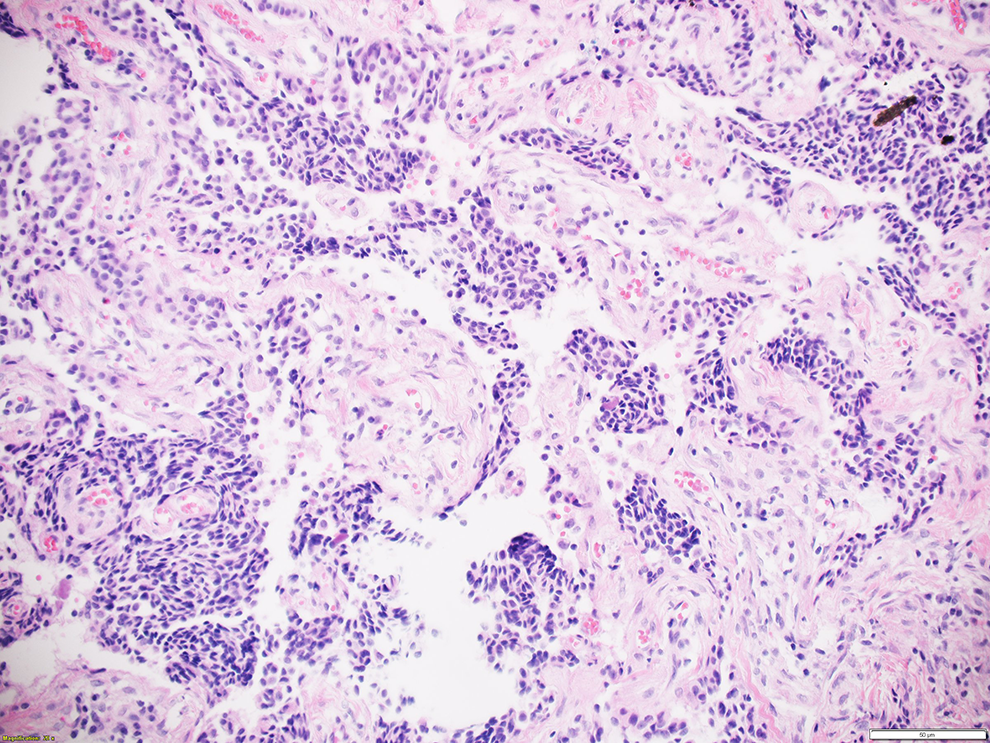
Histochemistry image of a middle ear adenoma (MEA) section. Hematoxylin-eosin stain; magnification ×200.
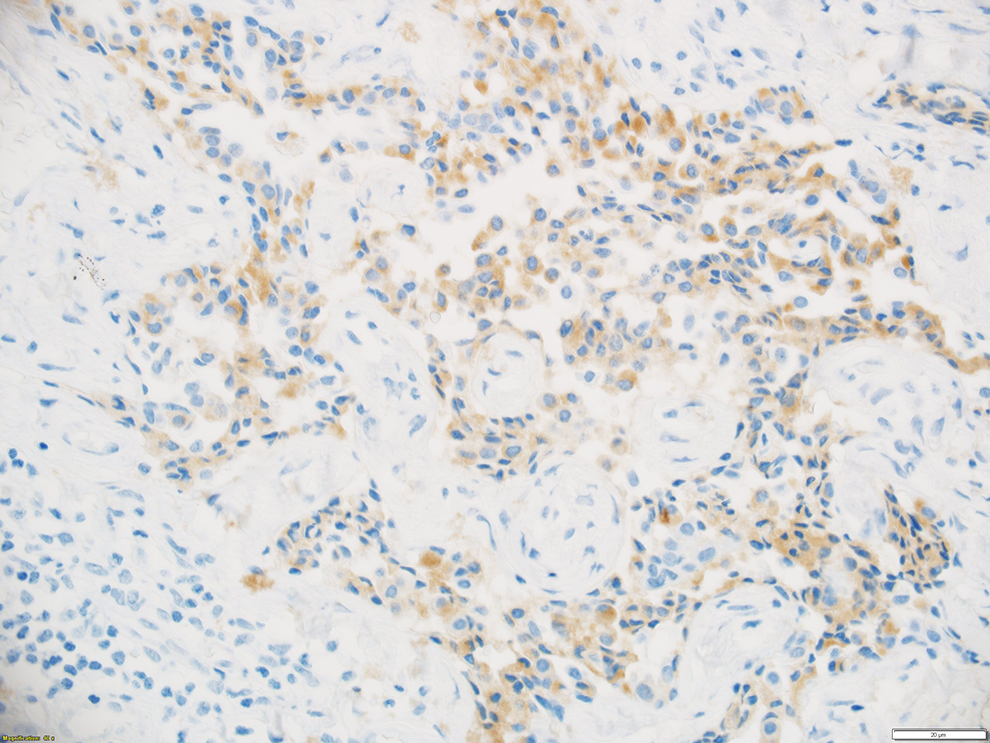
Immunohistochemistry image of an MEA tissue section. Synaptophysin stained positive (light brown); magnification ×400.
Surgery was indicated, with the aim of completely removing the tumor. After a discussion with the patient, we performed a tumor removal and a radical tympanomastoidectomy. Perioperative findings revealed soft, bleeding tissue limited to the tympanic cavity (Figure 5). The facial nerve canal remained intact. The surgery achieved complete tumor removal without any peri or postoperative complications. A definitive histopathological examination confirmed the presence of an MEA with exocrine and endocrine differentiation. Postoperative severe conductive hearing loss was successfully compensated with a hearing aid. The patient was followed up for 2 years, with no evidence of recurrence.
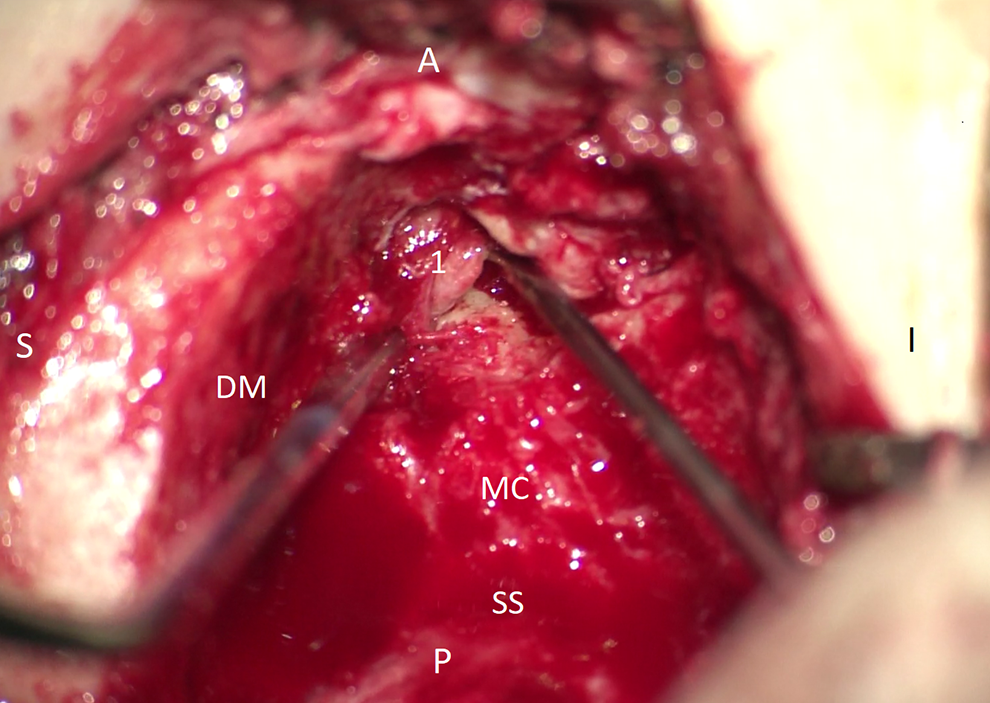
Perioperative microscopic image of the middle ear adenoma (MEA). A canal wall down mastoidectomy was performed to remove the adenoma. A, anterior; DM, dura mater; I, inferior; 1, adenoma; MC, mastoid cavity; P, posterior; S, superior; SS, sigmoid sinus.
Discussion
Middle ear adenoma was first described by Hyams and Michaels in 1976.2,4 Later, in 1980, Murphy et al described a similar middle ear tumor, which they called a carcinoid, and it showed ultrastructural and histochemical neuroendocrine features. 2 The detection of neuroendocrine markers revealed the bidirectional (neuroendocrine and epithelial) differentiation of this tumor. 5 The common phenotype and the similar characteristics of adenomas and carcinoids suggested that they could represent a spectrum of one entity; however, no consensus has been reached on this point. 6
The pathogenesis of MEA remains unknown. Hyams and Michaels postulated that the tumor might originate from middle ear mucosal cells.2,4 Another hypothesis, proposed by Torske and Thompson, was that MEAs might originate from an undifferentiated pluripotent endodermal stem cell with neuroendocrine differentiation. 5 This hypothesis was based on the fact that a neuroendocrine epithelial cell tumor origin was unlikely, because these cells are not typically present in the middle ear mucosa.7-9
Middle ear adenomas commonly encase or erode the ossicular chain; however, destruction of the surrounding compact bone has only rarely been reported. 5 Facial nerve involvement and compact bone destruction indicate a worse prognosis. 10 To date, only one case of distant metastasis has been reported. 11
Patients with MEAs commonly experience progressive unilateral conductive hearing loss, tinnitus, and a feeling of fullness in the ear.5,12 Headache and vertigo are not typical. We observed somewhat similar symptoms. However, in our patient, the symptoms were masked by postsurgical changes. In addition, we observed otorrhea, probably due to the presence of an MEA in an open trepanation cavity. These findings contributed to the fact that the adenoma was mistaken for a late surgical complication.
The radiologic findings for MEAs are typically nonspecific. Computed tomographies show a well-demarcated soft tissue mass without bony erosion, which commonly encases the ossicular chain. 13 The definitive diagnosis is based only on the histopathologic examination. The differential diagnosis must include infection, paraganglioma, and adenocarcinoma. 14 Microscopically, the MEA growth patterns are mainly glandular, less trabecular, and solid.7,9,15 Immunohistochemistry typically shows positive staining for cytokeratin, synaptophysin, chromogranin pancreatic polypeptides, neuron-specific enolase, and vimentin.8,9,16-19
The treatment of choice for an MEA is complete tumor resection and ossicular chain removal.7,12,20 Primary radiotherapy is not indicated, due to the relative radioresistance of MEAs. Radiotherapy is recommended as an adjuvant therapy in some cases, when the lesion is extensive.8,12,17,21 To date, only 6 patients with advanced disease have been described in the literature that received postoperative radiation therapy. The treatment demonstrated little success. 11 Middle ear adenoma recurrence or persistence was observed in 15% of patients, typically associated with insufficient radical resection (eg, when the ossicular chain was preserved).5,22 In the present case study, the tumor was limited to the tympanic cavity, and it was radically removed. Therefore, radiotherapy was not indicated.
Conclusion
Middle ear adenoma is a very rare pathology, but it should be considered in a differential diagnosis. It can resemble many other processes, and thus, it presents a diagnostic challenge; particularly when it resembles a late surgical complication, as in the present case study. Radical surgical removal is the treatment of choice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Health, Czech Republic—conceptual development of research organization (FNOs/2018).