
Abstract
Background:
To study the endoscopic trans-lateral molar (ETLM) approach to infratemporal fossa (ITF) lesions and analyze the advantages and disadvantages of this method.
Methods:
Four cases of ITF lesions were analyzed retrospectively. The clinical features, diagnosis and treatments, the operative process, and clinical applications of this surgical approach were discussed.
Results:
Postoperative pathologies were 2 pleomorphic adenomas, 1 schwannoma, and 1 inflammatory lesion. All patients had self-resolving cheek swelling and pharyngalgia in the short term, but 2 patients had numbness in the long term. There was no infection or bleeding in the postoperative period, and no difficulty in chewing after disease recovery. There was no tumor recurrence during the follow-up period.
Conclusion:
The ETLM approach is convenient, minimally invasive, and allows complete excision of benign ITF lesions, posterior to the lateral pterygoid muscle and mainly below the level of the hard palate. It is a simple and direct access to the ITF, but it is a narrow access because of the limitations of bones and soft tissues. Appropriate patient selection is mandatory for successful surgery.
Introduction
The infratemporal fossa (ITF) is located lateral to the midline of the skull base. It is bordered superiorly by the greater wing of the sphenoid bone, laterally by the ascending ramus of the mandible, anteriorly by the maxilla, medially by the pterygoid processes, and posteriorly and inferiorly by soft tissues. This region is also adjacent to the parapharyngeal space. It has many important structures such as the lateral and medial pterygoid muscles, pterygoid plexus, maxillary artery, and branches of the mandibular nerve.1,2 It is a challenge for surgeons to perform operations in this area, and many approaches are used to get through the surface into this area.
Infratemporal fossa lesions may involve the pterygopalatine fossa, Eustachian tube, middle and inner ear, base of the skull, and even the intracranial area. As the soft tissues and the facial skeleton are easy to deal with, surgeons often use the transfacial and cervical approaches to operate in this area. There are many well-described methods for open surgery in this area. Such as the maxillary swing approach, 3 mandibular swing approach, 4 and the A, B, C, or D type ITF approach proposed by Fisch.5,6 These approaches allow wide vision, and complete excision of the tumors and the involved tissues. The incision can be extended to the neck, and the cervical masses can be treated synchronously. 7 However, postoperative complications are very common and severe, such as hearing loss and facial paralysis.
Recently, endoscopic techniques have developed rapidly owing to their minimally invasive nature and accessibility, especially in patients with tumors confined to a small area. The endonasal transpterygoid approach is a well-developed endoscopic approach that goes through the lateral nasal wall, maxillary sinus, and pterygopalatine fossa, and then outward into the ITF. This approach is suitable for the lesions mainly located above the level of hard palate. 8 It can be combined with the endoscopic-assisted transvestibular paramandibular approach, if the lesions extend beyond the visual field. 9 In the current study, we describe a simple and rapid endoscopic trans-lateral molar (ETLM) approach to lesions located below the level of the hard palate and posterior to the media and lateral pterygoid muscles.
Materials and Methods
This study was approved by the ethics committee of the Xijing Hospital of the Fourth Military Medical University.
We describe this surgical technique in 4 patients (Table 1). Among the female patients, one of them was aged 40 years, and she was diagnosed with a well-circumscribed mass in the left ITF before undergoing tonsillectomy. The other female patient was aged 60 years and she was diagnosed with isolated masses in the left ITF while undergoing an operation for intracranial meningioma 7 months prior to the current presentation. Among the male patients, one of them was aged 63 years and had a history of recurrent secretory otitis media. A mass in the left ITF was diagnosed on magnetic resonance imaging (MRI). The other male patient was aged 61 years, and he had pains on the right buccal region during mouth opening. A mass in the right ITF was diagnosed.
Demographics and Clinic Outcomes of 4 Patients.
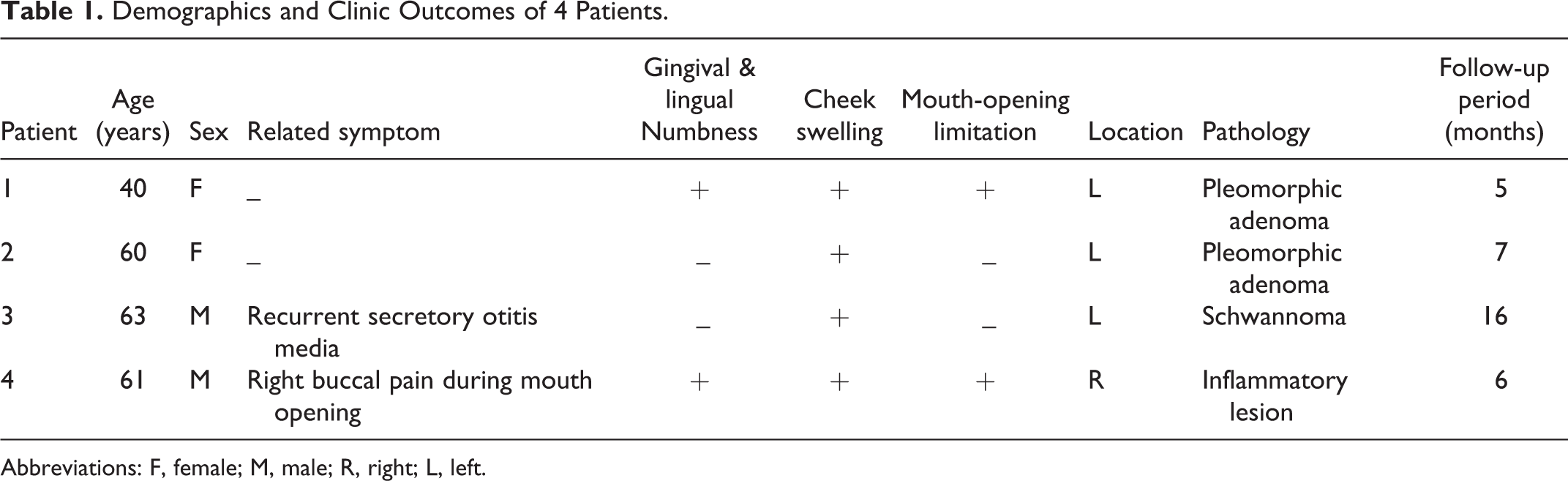
Abbreviations: F, female; M, male; R, right; L, left.
Surgical Method
All patients underwent general anesthesia by tracheal intubation; extreme mouth opening was achieved using a Davis mouth gag. On the side of the operation, we made an incision lateral to the gingivobuccal sulcus. The incision was 3 to 4 cm long from the maxillary tuberosity down to the mandibular ramus. We dissected the buccal muscle carefully, identified the temporalis attachment on the medial surface of the mandible, identified the buccal nerve, and pulled them away laterally using a retractor. After excising the excessive buccal pad, we exposed the pterygomandibular space. We identified the medial and lateral pterygoid muscles and dissected the lingual nerve anteromedially and inferior alveolar nerve posterolaterally. Through the space between these 2 nerves and 3 muscles (temporalis, medial, and lateral pterygoid muscles), we approached the posterior region of the ITF. This helped create a separate potential space between the medial and the lateral pterygoid muscles, exposing the capsule of the tumor in the ITF. We separated the capsule from the surrounding tissues, completely resecting the tumor piece by piece if it was solid, or did a liquid suction before excision if it was cystic, because of the narrow space. After this, the styloid process, the stylohyoid tendon, could be partly seen in a clear surgical field, and the internal carotid artery was in the posteromedial direction of this field (Figure 1). We controlled the hemorrhage and exposed the deep lobe of the parotid gland by bipolar coagulation, if necessary. We then placed hemostatic material (Surgicel Fibrillar, Johnson & Johnson) in the operative cavity and sutured the mucosal incision after ensuring complete hemostasis. We left a drainage strip at the incision site for 3 days after the procedure.
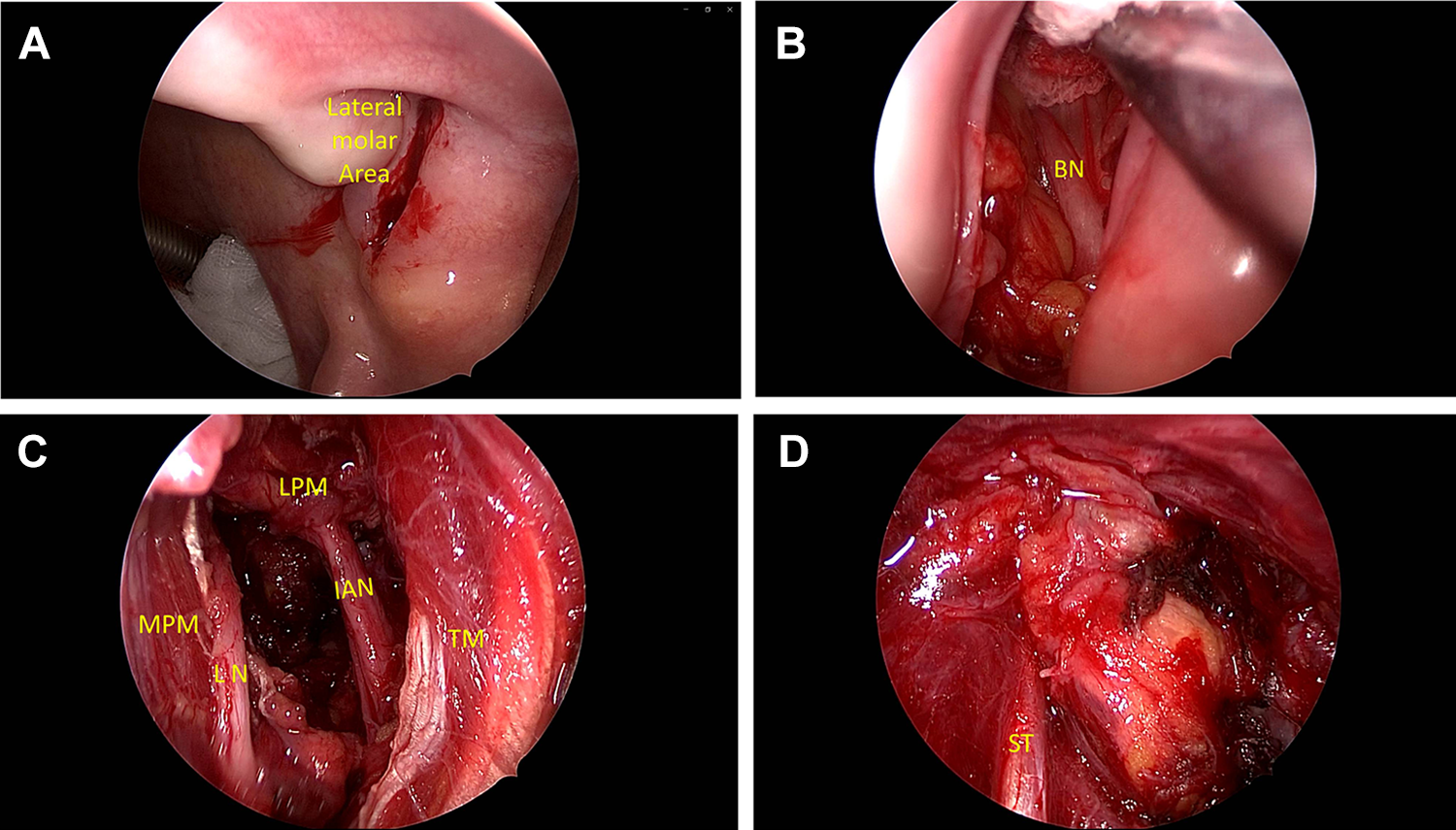
Surgical anatomy in endoscopic trans-lateral molar approach (all operations were performed by Professor Fu-quan Chen.). A, Incision on lateral molar mucosa on the left side. B, Pull away buccal pad, buccal nerve (BN) can be seen. C, Land marks in the procedure: lateral pterygoid muscle (LPM), medial pterygoid muscle (MPM), temporalis (TM), lingual nerve (LN), inferior alveolar nerve (IAN). D, Stylohyoid tendon (ST) in surgical field after tumor excision.
Results
Postoperative Pathology
All excised masses were benign. A pleomorphic adenoma was diagnosed in 2 patients (Figure 2), and a schwannoma (Figure 3) and an inflammatory lesion (Figure 4) were diagnosed in one patient each.
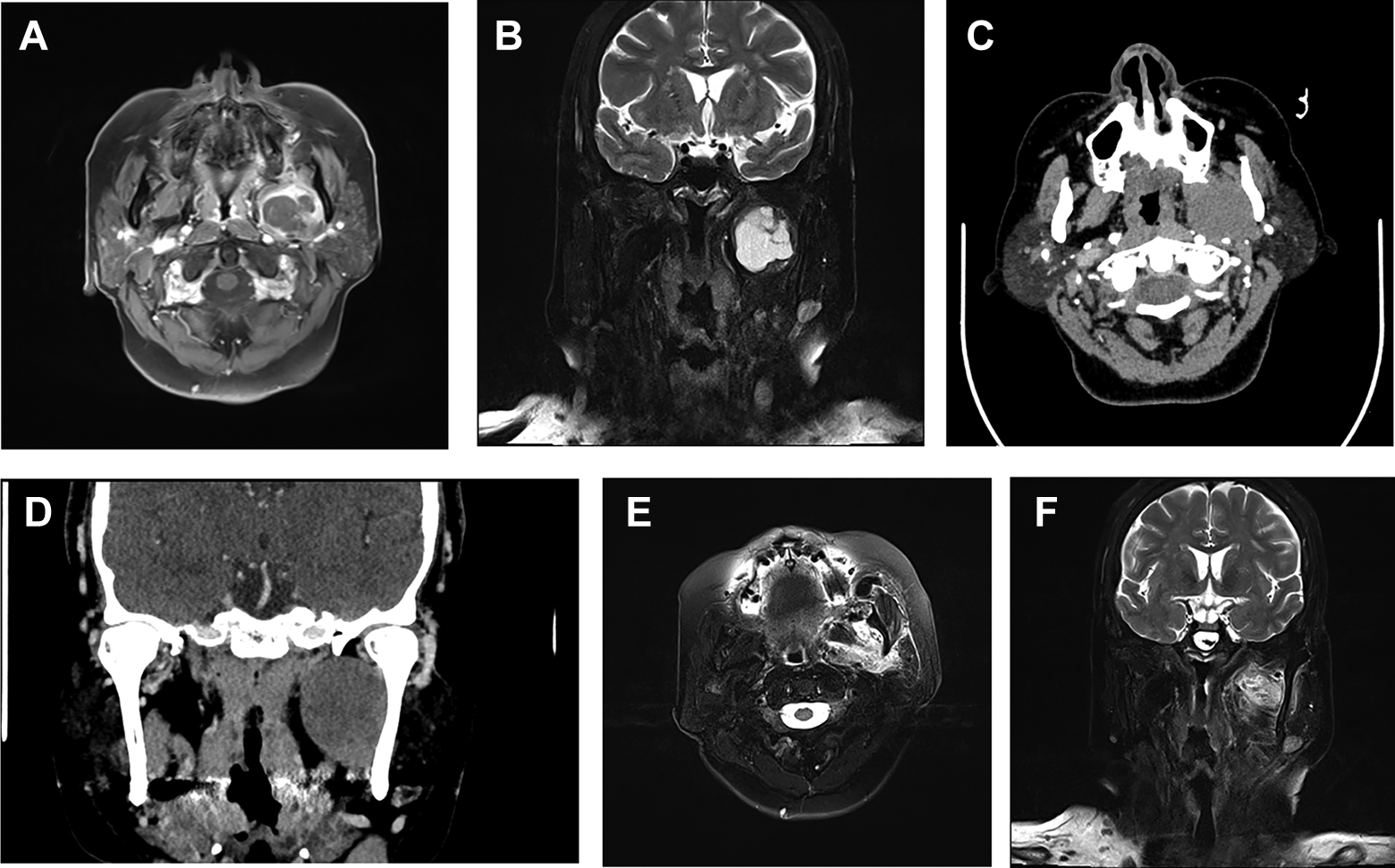
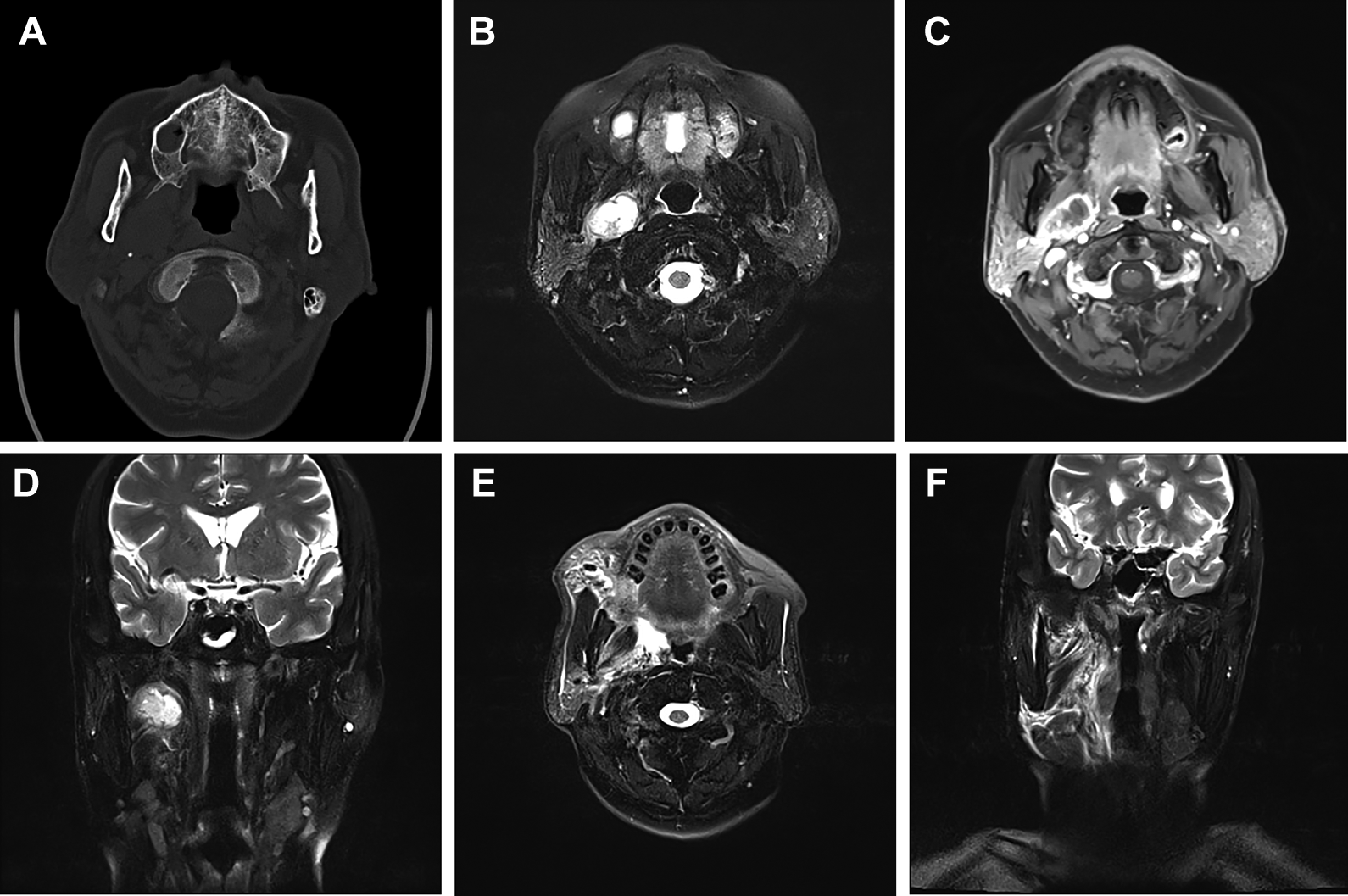
Radiological examination of patient No. 2 (Pleomorphic adenoma). (Endoscopic anatomy of this case is in Figure 1.) A and B, Preoperative MRI. C and D, Preoperative CT. E and F, Postoperative MRI. MRI indicates magnetic resonance imaging.
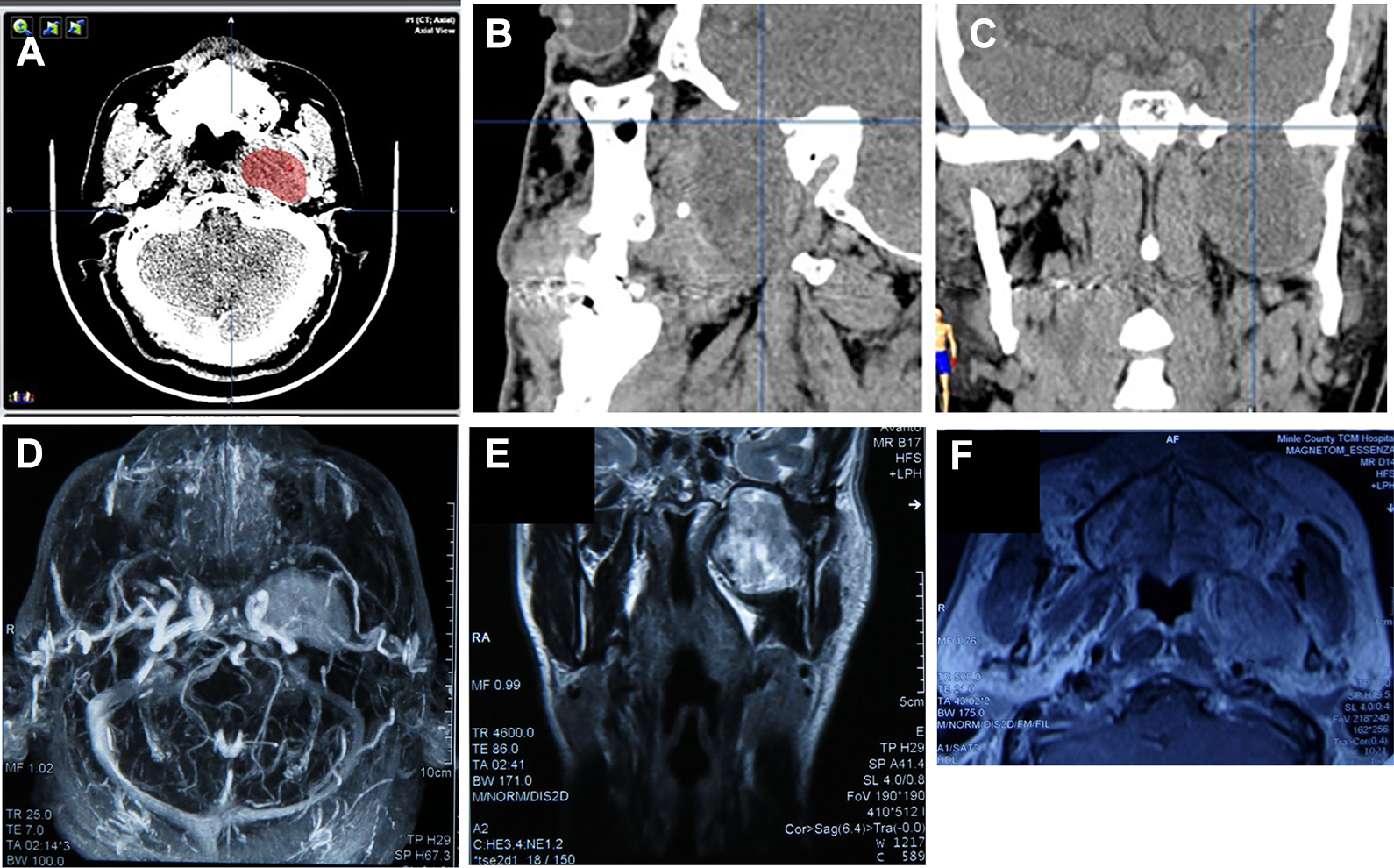
Radiological examination of patient No. 3 (Schwannoma). A-C, Preoperative CT. D and E, Preoperative MRI. F, Postoperative MRI. MRI indicates magnetic resonance imaging.
Radiological examination of patient No. 4 (Inflammatory lesion). A, Preoperative CT. B-D, Preoperative MRI. E and F, Postoperative MRI. MRI indicates magnetic resonance imaging.
Postoperative Complications
Postoperative follow-up ranged from 5 months to 16 months. All patients had a liquid diet for 3 days via a feeding tube and then switched to oral feeds later. Two patients developed numbness around the lip, gingival, and lingual areas on the affected side with no significant improvement after 3 months of operation, and gradual relief of mouth-opening limitation within 3 months after surgery. There was some resolution of numbness at the follow-up visit at 12 months. All patients had self-resolving cheek swelling and pharyngalgia within 7 days after the operation. This pain was mild (vasal analogue scale pain score ∼3 to 5), appeared after the procedure. There was no infection, bleeding in the postoperative period, and no difficulty in chewing after the disease recovery.
Postoperative Follow-Up
An MRI examination, on postoperative day 3, suggested a moderately swollen operative cavity with no residual tumor.
Discussion
The ETLM approach described in our study bypasses the maxilla, makes the best use of the natural space between the maxillary tuberosity and the mandibular ramus, eliminates the obstruction from the buccal muscle and the fat pad, and provides straight access to the anterior, inferior, and lateral areas of the ITF. Because of the unique movement of the temporomandibular joint, the horizontal distance between the maxillary tuberosity and mandibular ramus is approximately 10.1 to 14.3 mm with maximum opening of the mandible, and increases to 13.9 to 19.1 mm with the mandible deviated ipsilaterally. 10 This space is gaining recognition in trauma, oral surgery,11,12 and anatomical research, 13 but is not widely used in clinical practice.
In this approach, after excising the buccal fat pad, the lingual and inferior alveolar nerves could be seen in the anteromedial and posterolateral directions, respectively. These 2 nerves run to the distal organs and are far away from each other at this location. Moving the lingual nerve medially and inferior alveolar nerve laterally creates a gap through which the muscle fibers from the medial and lateral pterygoid muscles pass. Blunt separation (depending on the location and exposure of the tumor) is performed along these muscle fibers. This helps minimize injury to the medial and lateral pterygoid muscles and the branches of the mandibular nerve, which helps decrease gingival numbness and mouth-opening limitation after the surgery. Furthermore, this procedure takes advantage of natural anatomic spaces, avoids handling of the maxilla, incision of the skin, and fulfillment of cosmetic desires.
Several endoscopic approaches, such as the transnasal, endoscopic-assisted Denker’s approach, transoral soft palatal approach were described in many articles.14,15 Earlier approaches to enter the ITF included partial removal of the lateral nasal cavity, anterior wall of the maxillary sinus, or hard palate and then taking advantage of the enlarged natural sinuses to remove the posterior wall of the maxillary sinus and the pterygoid process, amputating the attached muscles, getting through the barrier between the pterygopalatine fossa and the ITF, and then exposing the lesion.16,17 Some surgeons proposed an endoscopic transoral approach, which involved removing the maxillary molar and moving a small part of the lateral maxilla, followed by dissection of the pterygopalatine fossa and the ITF lesion. 18 These approaches all go through the maxillary sinus and pterygopalatine fossa. 11 Extending the incision posterolateral to the medial and the lateral pterygoid muscles is often not required for benign lesions since this leads to more injury after the loss of bones and muscles. Furthermore, for patients with extremely undeveloped maxillary sinuses, this approach makes the operation longer and more difficult, and may also result in residual lesions.
The endoscopic-assisted transoral-transpharyngeal approach is another recently developed minimally invasive approach for ITF tumors. 19 It involves an incision on the soft palate, medial to the maxillary molar, and is suitable for tumors located close to the medial pterygoid muscle in the parapharyngeal space. The transnasal transpterygoid approach, as compared to this approach, is more suitable for tumors above the bottom of the maxillary sinus. The advantages and limitations of these approaches are listed in Table 2.
Endoscopic Approaches.
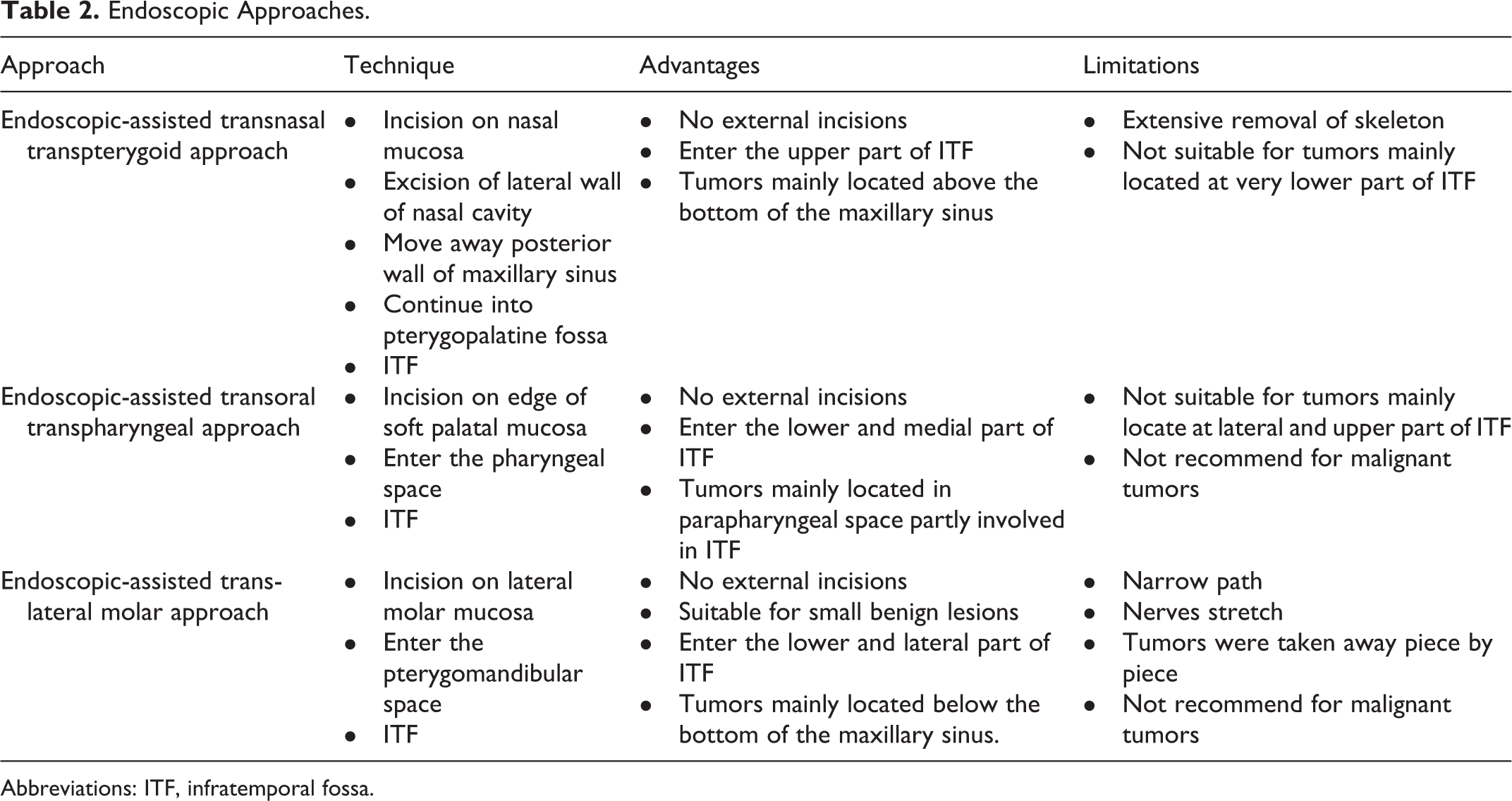
Abbreviations: ITF, infratemporal fossa.
Another approach did small double incisions on the facial skin, and used an endoscopic procedure to reach the ITF through the posterior area of the zygomatic arch. 20 However, this is an anatomical study and has not been applied clinically.
The ETLM approach described in this study is convenient and direct; however, it has several limitations. The operative vision is limited because of the narrow space between the maxilla and mandibular ramus. 13 Although it reduces the time required to deal with the maxilla, assistants are required to hold retractors to expose the lateral and anterior sides of the operative field because soft tissues collapse due to a lack of support from the hard bone. This often makes hemostasis difficult. We used a plasma knife and attracted electrocoagulation to control bleeding. Detailed imaging assessment is also required before the operation to know the vascular branches. Three-dimensional computed tomography helps to demonstrate the peritumoral vessels. Although the important structures remain intact during the operation, there are several short-term complications. Numbness and pharyngalgiaon the affected side are common. Pharyngalgia and mouth-opening limitation resolve completely in a short time, while numbness can last for more than 1 year. This may be due to intraoperative traction in the limited space during the procedure. Our study lacks long-term follow-up data. Large tumors should be taken out piece by piece because of the limited space, which may lead to a risk of relapse, especially for pleomorphic adenomas. We must irrigate the operative cavity adequately after resection.
Conclusion
The ETLM approach has a high demand in selected cases and can be applied to benign tumors confined to the region posterior to the medial and lateral pterygoid muscles, and anterior to the styloid process. However because of many limitations, appropriate patient selection is important for a successful operation. It also requires further studies for prognosis because of the lack of long-term follow-up.
Footnotes
Authors’ Note
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Ethics Committee of the First Affiliated Hospital of the Fourth Military Medical University, KY20192133-F-2) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this retrospective study, formal consent is not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been supported by National Natural Science Foundation of China (NSFC; grant No. 81670925 to Fu-quan Chen).