
Abstract
Objectives:
Obstructive sleep apnea syndrome (OSAS) is an increasing health problem, the diagnosis of which is generally delayed due to long waiting lists for the tests used to identify it. Therefore, tools that help on classifying patients at higher risk of suffering this syndrome have been developed.
Methods:
One hundred ninety-three consecutive patients, with and without OSAS, filled in the Spanish version of the STOP-Bang questionnaire in Hospital Universitario de Torrejón (Spain). Polysomnographies were performed to diagnose the presence and severity of the OSAS. Statistics analysis of the demographic characteristics of the sample and the questionnaire results was performed.
Results:
Most patients were male (73%) and the mean age was 50.4 years (ranging from 19-77 years). Cronbach α coefficient in the sample was 0.8072. A statistically significant difference was noted in the questionnaire scores between patients with OSAS and those without the syndrome.
Conclusions:
The Spanish version of the STOP-Bang questionnaire possess a good internal consistency that allows us to rely on it as a screening tool for patients with OSAS. In our sample, a difference in the questionnaire score was appreciated between patients with and without the syndrome, which strongly supports the utility of the questionnaire for its purpose.
Introduction
Obstructive sleep apnea syndrome (OSAS) is a health problem that has increased its prevalence in the last years. Current studies demonstrates that the prevalence of moderate-to-severe-disordered breathing among general population in adults is as high as 23.4% in females and 49.7% in males. 1 This sleep disorder is consequence of the repetitive interruption of the airflow during sleep caused by an upper airway closure. 2 One of the main causes that underlies this greater prevalence is the higher incidence of obesity in developed countries. 3
Obstructive sleep apnea syndrome implies a higher risk for circulatory,4-6 cardiovascular,7-9 and metabolic 10 diseases, as well as other endocrine, nutritional, and respiratory conditions. 11 This syndrome is underdiagnosed nowadays, and it is estimated that almost 80% of males and 93% of females suffering from a moderate to severe OSAS are not yet fully diagnosed. 12 Since this syndrome is associated with an increased morbidity 13 and mortality, 14 it is very important to establish an accurate and fast diagnosis, as simplest as possible, in order to prevent the negative consequences of an untreated syndrome.
The gold standard test used in the OSAS diagnosis is polysomnography (PSG), but this test is a time-consuming and expensive tool. The lack of enough sleep medicine specialists, in combination with the delay between the first consultation and the definitive diagnosis, worsen the scenario for these patients. 15 Cardiorespiratory monitoring (CRM) is also an accurate test to diagnose OSAS. Even though this test does not record neurophysiological variables, it has been demonstrated that CRM may serve as a substitute of PSG as the initial diagnostic approach for patients with a clinical diagnosis of sleep apnea. 16
Therefore, there is a need to improve the screening of OSAS in order to enhance the prescription of the PSG and CRM in those cases with a higher suspicion of OSAS. In that sense, different questionnaires have been probed to be useful as screening instruments. Questionnaires such as the Berlin Questionnaire,17,18 the Wisconsin Sleep Questionnaire, 19 or the STOP-Bang Questionnaire 20 have been validated for that purpose and they possess different positive and negative predictive values.
STOP-Bang Questionnaire has demonstrated to possess the highest sensitivity for OSAS, and is the one recommended in the systematic review by Abrishami et al. 21 It consists of 8 questions regarding observed snoring, tiredness, observed apnea, blood pressure, body mass index (BMI), age, neck size, and gender. Each question is weighted equally, and each “yes” response equals 1 point. Depending on the obtained score, the risk for suffering OSAS is different. Therefore, patients with 2 points or less in the questionnaire present a low risk for OSAS, those with 3 or 4 points in the questionnaire present an intermediate risk for OSAS, and those with 5 points or more present a high risk for OSAS. The main objective of this article was to validate the translated version of the STOP-Bang Questionnaire in order to use it as a screening tool in Spanish-speaking patients with a moderate-high risk for OSAS.
Methods
This study was conducted according to the principles stated in the Declaration of Helsinki of 1983. The presented study was approved by the Ethics Committee of Hospital Universitario de Torrejón in Madrid. Before the inclusion of the patients into the study, a written informed consent was signed by each patient.
Since the Questionnaire is property of the leading authors, we contacted them and obtained the license to use it on an academic purpose. We found the STOP-Bang Questionnaire already translated into Spanish (Figure 1) on the official website of the tool (http://www.stopbang.ca/translation/translation.php); therefore no new translation, back-translation to English, nor harmonization of the translated version was needed.
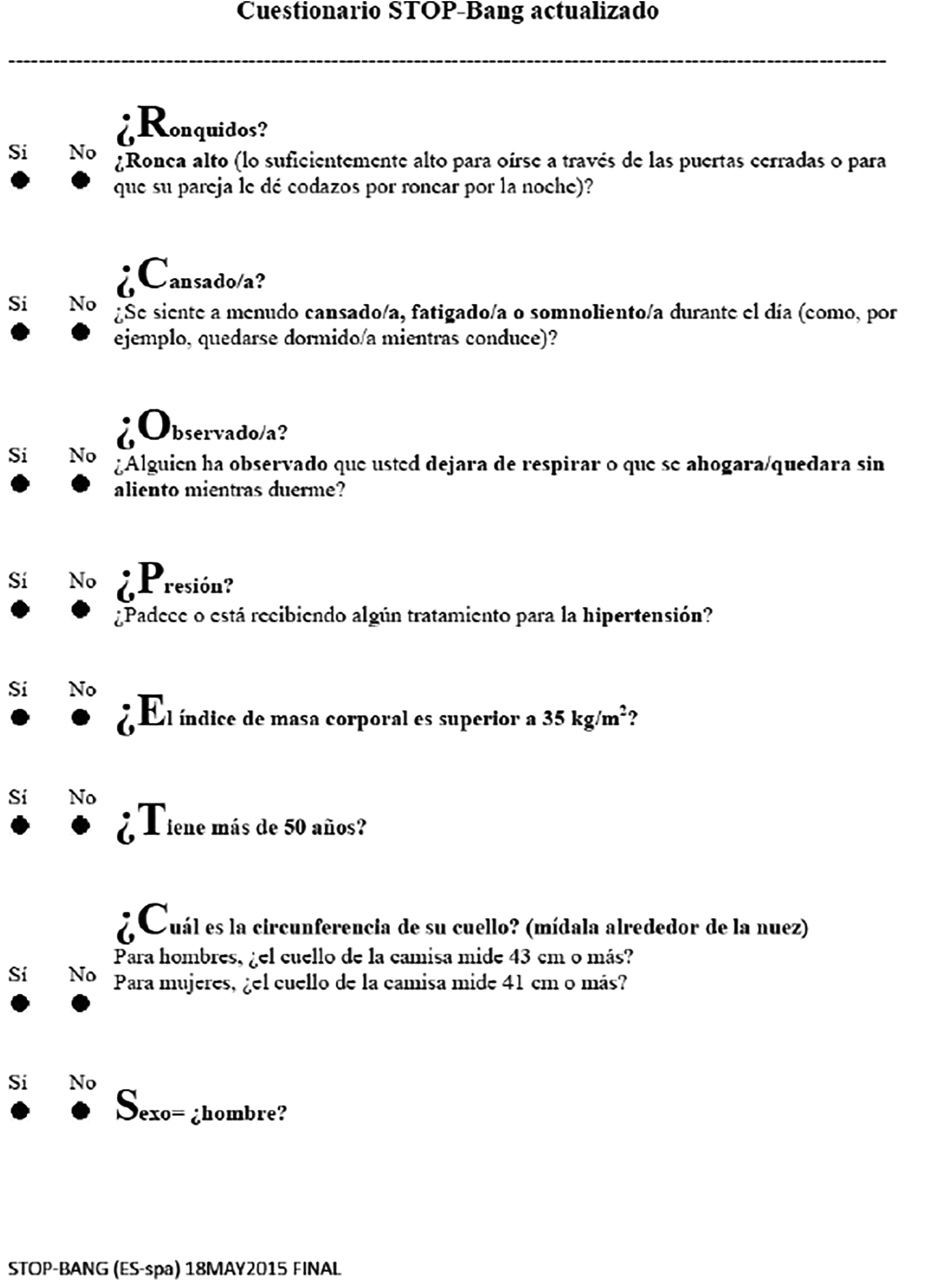
Spanish version of the STOP-Bang questionnaire.
To verify the questionnaire, 193 consecutive patients referred to the Ear, Nose and Throat Department with a suspected OSAS were enrolled. Of these, 150 patients had a PSG confirmed OSAS, and they were derived afterward to evaluate options on their treatment. The remaining 43 patients presented no OSAS.
Each patient answered questions regarding categorical data, and were asked about the clarity of each one. None of the 193 patients had difficulties understanding the questions, and when they were inquired about what they think the question was relating to, their explanation matched with the original question itself.
The results of the PSG determined the diagnosis of OSAS in these patients referred from the Respiratory Department. Every PSG was performed by certified technicians following the 2007 American Academy of Sleep Medicine (AASM) recommended setup specifications. 22 Each study was assessed and scored by one of the neurophysiologists at our center using Nicolet vEEG Reader software (version 5.94.1.534, Cephalon), as it is the usual practice at our Hospital. Results of the PSG are shown by means of the Apnoea Hypopnoea Index (AHI); an AHI of 5 to 14 is considered as a mild OSAS, AHI between 15 and 29 is considered as an intermediate OSAS, and values greater than 30 is considered a severe OSAS.
Statistical analysis was performed with XLSTAT program (version 2017.1, Addinsoft). Descriptive statistics of the sample were obtained. Continuous data were summarized as mean ± 95% confidence interval. Categorical data were presented as percentages. Reliability of the Spanish version of the STOP-Bang questionnaire was assessed by means of Cronbach α. Student t test was used to determine whether there was a statistically difference in STOP-Bang scores between patients presenting OSAS and those without the syndrome. A partial least square regression was performed to explore the relationship between the different items included in the STOP-Bang Questionnaire (SBQ) and the presence of OSAS. Values of P below .05 were considered significant.
Results
A total of 193 patients completed the questionnaire between June 2017 and June 2019. In order to assess the proper comprehension of the questionnaire, patients were asked to point out whether they found difficult to understand what the question referred to. None of the patients had trouble on understanding the meaning of the question and, hence, they easily answered the questionnaire.
Of the 193 patients enrolled in the present study, 141 patients were males and 52 were females. The mean age of the patients was 50.4 years, ranging from 19 to 77 years. The mean BMI of the sample was 29.83 ± 6.12 kg/m2, ranging from 19.4 to 55.5 kg/m2. The mean AHI of patients presenting OSAS was 43.96 ± 24.91 events per hour, ranging from 5.7 to 146 events per hour. Patient baseline characteristics are summarized in Table 1.
Characteristics of the Sample of Patients (n = 193) That Were Enrolled in the Present Study.
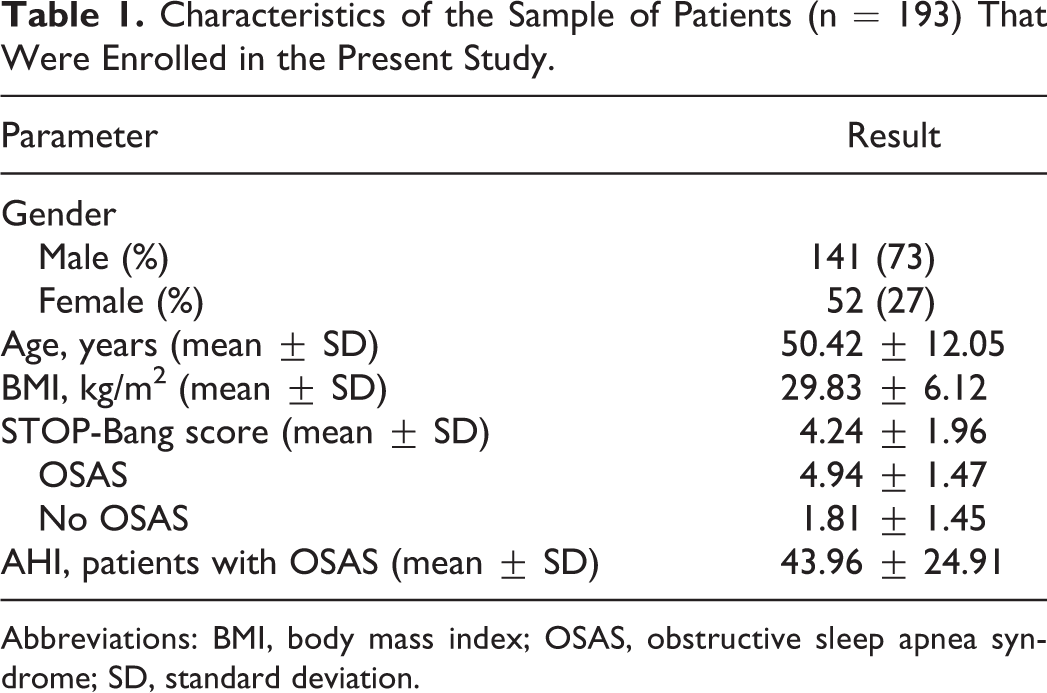
Abbreviations: BMI, body mass index; OSAS, obstructive sleep apnea syndrome; SD, standard deviation.
Mean value of the STOP-Bang questionnaire in the total sample was 1.87 ± 1.96. In those patients with an OSAS diagnosis, mean score of the STOP-Bang Questionnaire was 4.94 ± 1.47, while the mean score of the patients that did not present OSAS was 1.81 ± 1.45. There is a statistically difference between mean scores on the different groups (P <.0001). Figures 2 and 3 show questionnaire scores and its distribution in patients with and without OSAS, respectively.
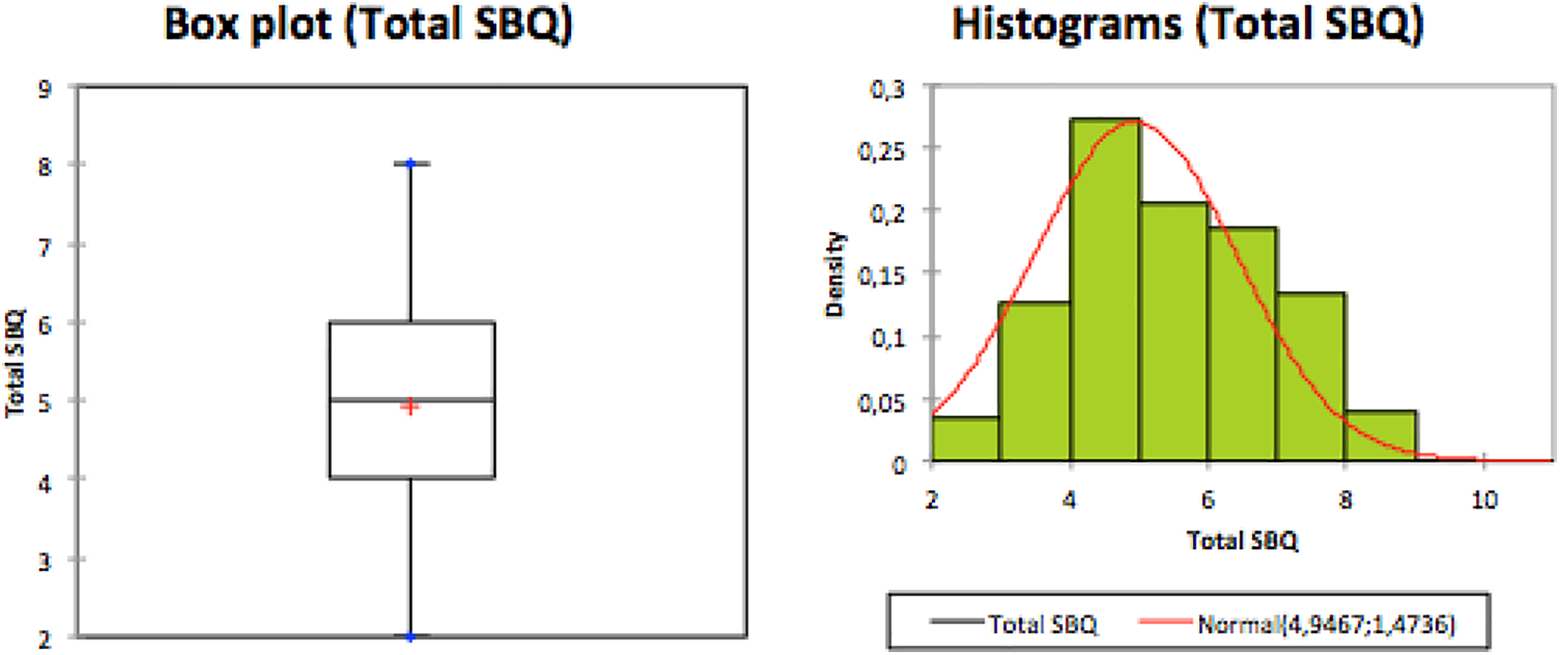
Questionnaire scores and its distribution in patients with OSAS. OSAS indicates obstructive sleep apnea syndrome.
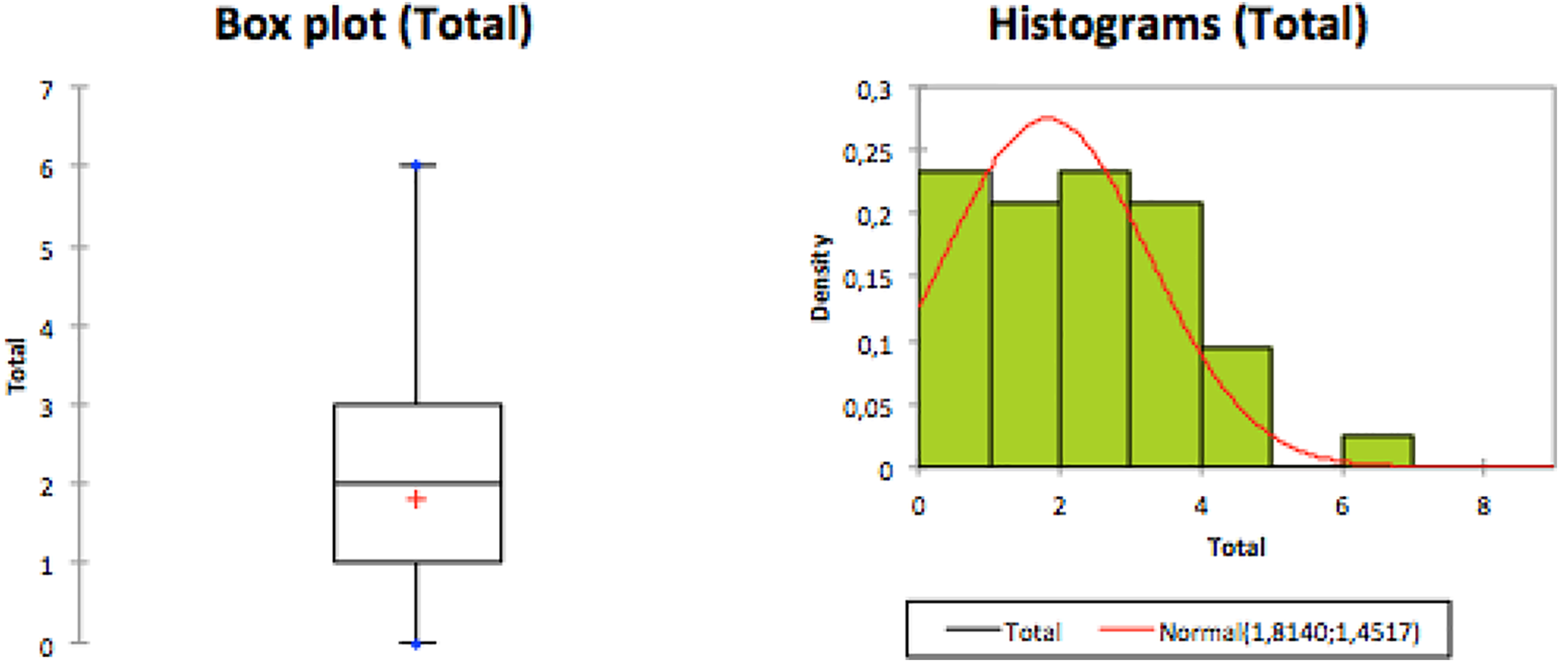
Questionnaire scores and its distribution in patients without OSAS. OSAS indicates obstructive sleep apnea syndrome.
The sensitivity of STOP-Bang score ≥ 3 to detect moderate–severe OSAS and severe OSAS is 98%, while the specificity is 60% and 34%, respectively. Negative predictive value is also 94% and 97%, respectively. STOP-Bang scores ≥ 5 present a sensitivity to detect moderate–severe OSAS and severe OSAS of 58% and 63%, and a specificity of 92% and 74%, respectively. Accuracy of the test is around 70% in every scenario. Predictive values of moderate risk and high risk STOP-Bang scores for moderate–severe OSAS and severe OSAS are shown in Table 2.
Predictive Values of Moderate Risk and High Risk STOP-Bang Scores for Moderate–Severe OSAS and Severe OSAS.

Abbreviations: NPV, negative predictive value; PPV, positive predictive value.
Cronbach α coefficient was used to assess the reliability of the Spanish version of the test. Values over 0.8 prove a good internal consistency of the questionnaire. The Cronbach α coefficient in our sample was 0.8072, demonstrating therefore, the reliability of the Spanish version of the questionnaire.
The partial least square regression shows the weight of every item of the SBQ related to the AHI and their global weight. The presented Q2 cumulative index is of 0.42, measuring the goodness of fit and the predictive quality of the model, which ideally should be close to 1. The cumulated R2Y obtained is of 0.45. A value between 0.33 and 0.67 indicates a moderate predictive accuracy. We also present the parameters of the model corresponding to each dependent variable in order to show the weight of every variable in the equation of the model.
Variable importance for the projection for each explanatory variable is shown in Figure 4. This allows to identify which are the variables that contributes the most in presenting OSAS.
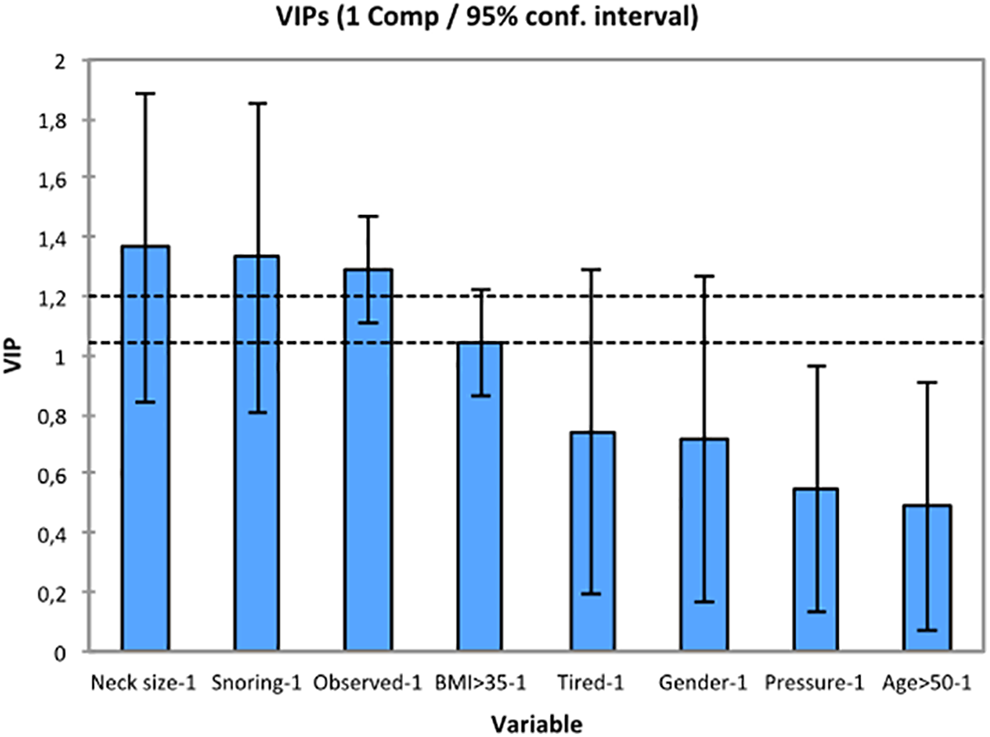
Variable importance for the projection for each explanatory variable.
The frequency of each item response is presented in Table 3 with their corresponding model parameter.
Frequency of Each Item Response and Their Corresponding Model Parameter.
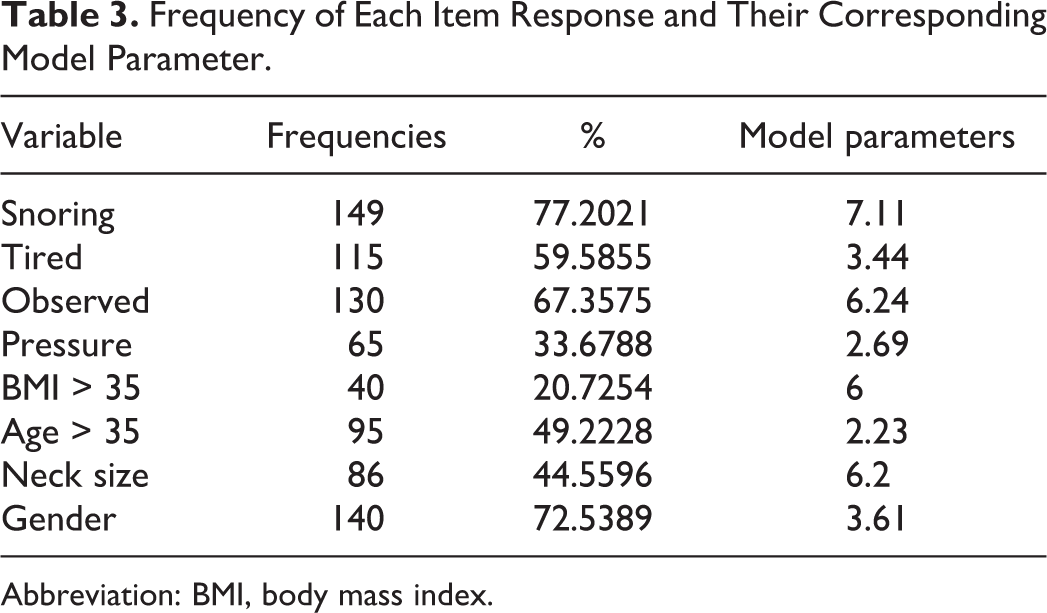
Abbreviation: BMI, body mass index.
Discussion
Obstructive sleep apnea syndrome is a health problem that has increased its prevalence in developed countries in a very notorious way in the last few years. This higher prevalence may be due to higher obesity rates in general population, but it may also be consequence of the greater clinical suspicion by practitioners, and also due to an improvement in diagnosis tests. Since the gold standard for OSAS diagnosis is PSG, waiting lists for this test have risen exponentially, which causes a delay in both the diagnosis and the treatment of patients with OSAS.
Early treatment of OSAS has shown to diminish comorbidities and mortality.23-25 Treatment of choice is the Continuous Positive Airway Pressure (CPAP) Therapy, 26 but it presents a poor adherence. 27 Therefore, alternatives to this treatment has been proposed, such as the upper airway surgery or oral appliances that have demonstrated to be as effective as CPAP in mild and moderate OSAS28-30 in selected patients.
In order to fasten the diagnosis and the treatment of patients suffering of OSAS, other tests that may replace and ease the diagnosis has been described, such as CRM or respiratory polygraph, but even though they help to fasten the diagnosis of these patients, they have not yet totally solved the waiting lists problem.
In this regard, a better screening of patients with a higher probability OSAS would help to optimize our clinical resources. Accordingly, screening questionnaires, such as the Berlin Questionnaire, the Wisconsin Sleep Questionnaire, or the STOP-Bang Questionnaire, have been developed.
STOP-Bang questionnaire was developed and validated in Canada, as a reliable screening tool to predict OSAS, and it is already validated and used in many countries such as Denmark, 31 China, 32 Portugal, 33 or Brazil. 34 It was developed by anaesthesiologists 20 on preoperative surgical patients to avoid postoperative complications due to an undiagnosed OSAS, 35 and has proved to be useful as screening tool for perioperative risk stratification 36 on a recent meta-analysis. Even though it was first described to be used on preoperative patients, it has demonstrated its usefulness for OSA screening in general adult population. 37 Even though the Spanish translation of the test was already performed by the authors, and used in different studies,38-40 this version was not validated in a Spanish population; therefore the consistency of the translated version was not yet fully guaranteed.
The STOP-Bang Questionnaire is composed of 8 dichotomous (yes/no) questions related to symptoms and clinical features of OSAS (snoring, tiredness, observed apnea, high blood pressure, BMI, age, neck circumference, and male gender). Each positive answer scores 1, and the total score ranges from 0 to 8. It is an easy questionnaire to be filled, and it takes around 1 to 2 minutes to be completed. STOP-Bang questionnaire offers a sensitivity of 93% and 100% to detect moderate (AHI > 15) and severe (AHI > 30) OSAS, respectively, when a total score higher than 3 is found. 41
As a result of its efficiency, high sensitivity, and easiness, this questionnaire has been used and validated in other specific populations with different medical conditions, such as pregnant women 42 or patients with mental diseases 43 or epilepsy. 44
In the present study, we validated the Spanish version of the questionnaire that was already published on the official site of the STOP-Bang Questionnaire. We proved that the Spanish version of the STOP-Bang Questionnaire is a clear, comprehensible, and a reliable tool. Therefore, the original questionnaire and the translated version are consistently equivalent.
In our sample, a statistically significant difference (P < .0001) was found in the STOP-Bang scores between patients with OSAS and without this syndrome. Hence, the STOP-Bang Questionnaire demonstrates its usefulness as a screening tool for patients at higher risk of OSAS in our sample.
Predictive values were also calculated in our studied population, and our results are similar to those found in other studies. 20 STOP-Bang presents a high sensitivity to detect patients at high risk for moderate–severe OSAS when a score ≥3 is found, with a high negative predictive value. In those cases where a score ≥5 is found, a high sensitivity and specificity are also found, as well as a high positive predictive value.
Since our sample is different from the population in which the SBQ was developed, we theorized that perhaps some items included in the questionnaire may not have the same importance and frequency in our sample. Therefore we performed a partial least square regression that indicated a moderate predictive accuracy. We present the frequency of each response with their model parameter, which gives an impression of the relative importance of each item in presenting OSAS. Highest values are registered for the neck size (N), snoring (S), observed (O), and the BMI (B); the remaining 4 items present less weight in the equation, which implies that in our sample these last items play a less important role in the development of OSAS. A visual representation of this fact is shown by means of the variable importance for the projection of each explanatory variable in Figure 4, and in this case, the 4 items mentioned above present, as well, as the main variables contributing to OSAS development.
Therefore, we believe that the STOP-Bang Questionnaire has proved to be a reliable tool identifying patients at a moderate risk of presenting moderate–severe OSAS, and, on this basis, it might enhance the screening of patients at a higher risk for the disease. Ultimately, its use may help in speeding up the diagnosis and treatment of those patients, and, consequently diminish the comorbidities inherent in the untreated patient.
Spanish is the second most spoken language as a native language worldwide, with more than 400 million speakers mainly distributed in Spain and South and Central America, but also in North America; and it is increasing as a second language all over the world. 45 On this basis, validation of the Spanish version of the STOP-Bang Questionnaire will help to improve the OSAS screening on a large population spread out over more than 20 countries using Spanish as a native language.
Conclusion
We believe that the use of different questionnaires in order to enhance the resources on OSAS diagnosis is essential to expedite the screening and the treatment. STOP-Bang Questionnaire has proved to be an efficient tool in that sense, but was not yet validated into Spanish. Spanish translation of the questionnaire possess a high correlation value with the original questionnaire that confirms its reliability as a screening tool of OSAS for Spanish population.
Footnotes
Authors’ Note
Ethical approval was obtained from Ethics Committee of Hospital Universitario de Torrejón in Madrid. Before the inclusion of the patients into the study, a written informed consent was signed by each patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.