
Abstract
Nodular fasciitis (NF) is a benign, self-limiting, reactive soft tissue tumor that is composed of fibroblasts and myofibroblasts and is often misdiagnosed as a malignant lesion. Nodular fasciitis is often reported in adults but rarely seen in children. We report the case of a 3-year-old girl with a rapidly growing NF in the left nasal cavity. The initial biopsy suggested the possibility of a spindle cell tumor or low-grade malignant tumor, respectively. The child underwent complete excision of the tumor. With the help of immunohistochemistry and pathological consultation, the final diagnosis was confirmed as NF. There was no recurrence during an 18-month follow-up period.
Introduction
Nodular fasciitis (NF) is a benign, reactive mass composed of fibroblasts and myofibroblasts. 1 It was originally described by Konwaler et al in 1955 as a pseudosarcomatous fibromatosis with rapid growth. 2 The exact etiology of NF is unknown, but trauma or localized nonspecific inflammation has been considered as a possible trigger. 1 Histologically, NF is characterized by dense cellularity, abundant spindle-shaped cells, and prolific mitotic activity. 3 As a result, NF is commonly misdiagnosed as sarcoma. 3
In adults, NF usually occurs at the upper extremities, trunk, head, neck, and lower extremities 4 and may involve the superficial fascia, subcutaneous tissue, and/or muscle. 5 Both sexes are equally affected.6,7 The lesion typically occurs in adults aged 20 to 40 years. 6 The size of the tumor is usually less than 2 cm in diameter. 6 In infants and children, the head and neck regions are the most common sites. 8
Nodular fasciitis poses a great diagnostic challenge for both clinicians and pathologists. To prevent unnecessary treatment, quick and accurate diagnosis is important.
There is sparse information about NF in the nasal cavity of children. Harrison et al reported a case of NF in the right nasal cavity of a 19-month-old female in 1995. 6 As the biopsy report implied an inflammatory condition, oral steroids were prescribed for 3 days but had no effect. The lesion continued to enlarge and was removed 1 month later. Histologic examination later confirmed a diagnosis of NF. 6
We present the case of a 3-year-old girl with NF in the left nasal cavity. Initially, a biopsy of the lesion was performed in a local hospital, and histopathologic examination suggested a hemangiopericytoma-like tumor. After complete excision and subsequent pathological consultation, the diagnosis of NF was confirmed. Treatments for benign and malignant tumors are extremely different. To facilitate the most appropriate therapy, an accurate diagnosis is critical.
Case Report
A 3-year-old girl was sent to a local hospital for evaluation of a runny nose and rapidly growing mass in her left nasal cavity, which was noticed by her parents. At first, it was thought to be influenza or sinusitis. Later, the swelling became more significant and traces of blood were found in her nasal discharge after 10 days. Biopsy of the lesion was performed under general anesthesia. The pathologic report described a hemangiopericytoma-like tumor of the nasal cavity and excluded inflammatory myofibroblastic spindle-shaped cell tumors. The rapidly enlarged mass blocked the patient’s nasal passage, so she was transferred to our hospital. A specimen was sent to the pathology department of our hospital for analysis, and a low-grade myofibroblastic sarcoma (LGMFS) was suggested. The child had frequently upper respiratory infections. No history of trauma relating to the nose was found. The girl was born at full term without antenatal issues.
On physical examination, a palpable ivory-white mass in the left nasal cavity was observed through anterior rhinoscopy. The mass compressed the nasal septum to the right side and showed no ulceration. Mucopurulent discharge was observed in the left nasal passage. No cervical lymph node enlargement was found on palpation.
Computed tomography (CT) demonstrated abnormal soft tissue filling in her left nasal cavity, and the boundary between the tumor and nasal turbinate was unclear. Severe deviation of the nasal septum was seen toward the right side, and the adjacent ethmoid sinus and maxillary sinus were compressed. Bone destruction was not evident. The lesion measuring 2.0 × 2.3 × 5.6 cm extended from the nasal vestibule anteriorly to the nasopharyngeal cavity posteriorly. On enhanced CT scanning, the lesion was shown as a well-defined, inhomogeneous, dense mass with an obvious rim or peripheral enhancement (Figures 1 and 2). On magnetic resonance imaging (MRI), the mass appeared as slightly inhomogeneous hyperintense signal on both T1-weighted imaging and T2-weighted imaging.
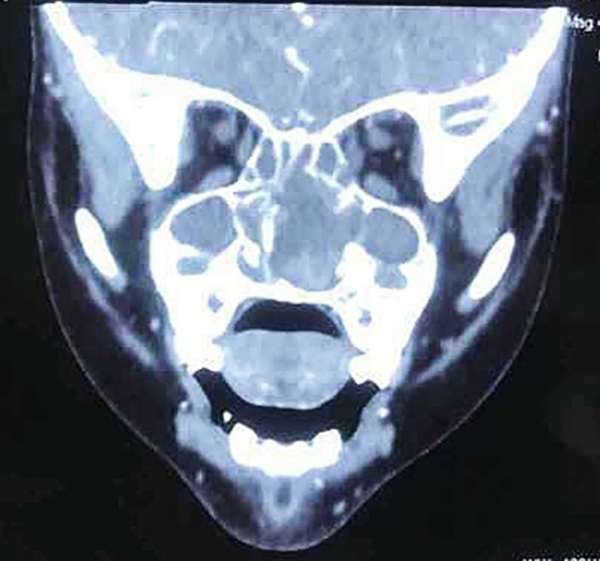
Coronal computed tomography. The mass filled in her left nasal cavity and the boundary between the tumor and the nasal turbinate was unclear. The nasal septum was pushed to the right side.

Axial computed tomography. The lesion was shown as a well-defined, inhomogeneous, dense mass with an obvious rim or peripheral enhancement, measuring 2.0 cm × 2.3 cm × 5.6 cm extended from the nasal vestibule anteriorly to the nasopharyngeal cavity posteriorly.
A comprehensive preoperative examination was performed to exclude surgical contraindications. During the operation, the mass was found to arise from the middle turbinate, which was well circumscribed and expanded into the right nasal cavity by compressing the nasal septum. The ethmoid sinus and maxillary sinus were not involved in the tumor, which meant that the soft tissue density noted on CT was actually obstructive inflammation. These were not pathognomonic of NF but suggested that this mass was more likely to be a benign tumor. We proceeded with complete removal of the lesion and submitted the specimen to our pathology department for further examination (Figure 3). Microscopy results indicated an arrangement of spindle fibroblasts in bundles or a whorled pattern, under the background of myxoid changes. The fibroblasts appeared as small fissures and at times expanded into the small sacs which contained some extravascular erythrocytes (Figure 4). Immunohistochemical staining showed that the specimen was positive for SMA, STAT6, and CD34 and negative for ALK-D5F3, AE1/AE3, EMA, desmin, CD68, S-100, and SOX10. These findings were suggestive of NF. After the third pathological consultation, the lesion was finally diagnosed as NF.

Clinical photograph of the nasal cavity lesion.
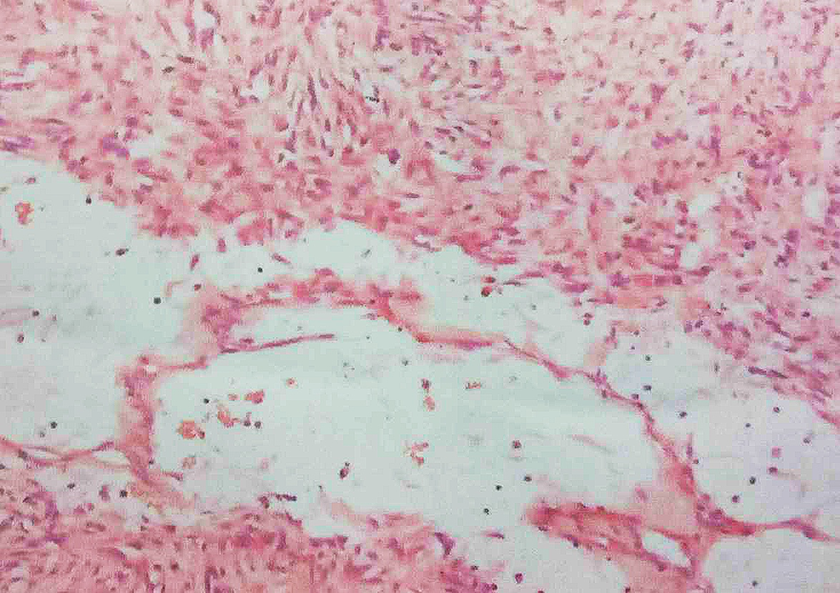
Microscopic view of the specimen. Myxoid area with spindle cells and pseudovascular slits.
Discussion
Nodular fasciitis is typically presented as a rapidly growing, solitary, well-defined mass that reaches 2 to 3 cm in diameter within a few weeks. Trauma or inflammation has been associated with the occurrence of NF. Recently, a molecular cytogenetic study demonstrated recurrence of the MYH9-USP6 fusion gene, suggesting that NF is the first known self-limited “transient neoplasm.” 9 There are no sex differences with regard to morbidity. The peak onset age of NF is 20 to 40 years, with an average of 34 years. Nodular fasciitis is rarely seen in adults over 70 years or children. 4 Nodular fasciitis is most commonly located in the upper extremities. 4
Nodular fasciitis is an incidental benign lesion. It is difficult to distinguish NF from other benign and malignant lesions by its rapid growth, rich cellularity, active mitotic activity, and poor encapsulation. Clinically, NF tends to be misdiagnosed as sarcoma (eg, fibrosarcoma, rhabdomyosarcoma, leiomyosarcoma) and reactive lesion (eg, pyogenic granuloma). Nodular fasciitis can also be misdiagnosed as a rare variant of squamous cell carcinoma and myxoid hematologic malignancies.
In our case, the 3-year-old girl was first misdiagnosed as LGMFS. In contrast to NF, LGMFS is commonly located in the thigh, abdominal wall, and antebrachium. The 2 entities may be differentiated from each other by immunohistochemical features. Low-grade myofibroblastic sarcoma tends to be positive for vimentin and Ki-67 and negative for S-100, SMA, MSA, desmin, caldesmon, CD34, and bcl-2.
Radiologically, the appearance of NF is nonspecific. Most of the lesions appear as a solitary, hypoechoic tissue on sonography. On CT, NF acts as a fascia-based, oval-shaped, homogeneous, and low or isodensity mass. Most of the NF appears as a homogeneous mass with broad fascia bases, which are usually referred to as the “fascial tail sign.”10,11 This is regarded as a valuable sign for distinguishing NF from other superficial tumors. On MRI, NF is often demonstrated as a homogeneous and hypointense or isointense to muscle on T1-weighted sequences and heterogeneous with intermediate-to-high signal on T2-weighted sequences, with enhancement differences because of variable components and cellularity. 12
Pathologically, there are 3 different types of NF, namely, the mucous, cellular, and fibrous subtypes. 13 Classification is considered irrelevant for treatment, but the pathological characteristics can help in diagnosing NF. Nodular fasciitis is a benign pseudosarcoma that involves myofibroblastic proliferation and is similar to sarcoma. It can be differentiated by rich cellularity, as well as plump and immature-looking fibroblasts that are arranged in irregular bundles or fascicles. There are many small fissures around the fibroblasts, which are sometimes expanded into small sacs. 4 A small number of extravascular red corpuscles located in these small fissures can be easily mistaken for a newly formed vascular lumen system, but no endothelium is observed in immunohistochemical staining; thus, they are referred to as pseudohemangiomas. The spindle cells grow within a monoid matrix background, which is usually adjacent to the wide collagen bands. 4 Immunohistochemistry revealed that the spindle cells showed a diffused expression of smooth muscle actin. The immunohistochemical markers are positive for calponin and muscle-specific actin CD10. Intralesional histiocytes and small multinucleated giant cells are positive for CD8, but negative for other makers, including desmin, B-catenin, ALK, h-caldesmon, CD34, and S-100 proteins. 4
In summary, NF is a benign pseudosarcomatous myofibroblastic lesion with a rapid progression. 14 The rapid growth, rich cellularity, mitotic activity, and histological images of NF mimic those characteristics of sarcoma. It is often misdiagnosed, especially in children. Final diagnosis can only be confirmed after consultations with both clinicians and pathologists. Accurate diagnosis is critical in preventing unnecessary treatment. Nodular fasciitis is self-limiting and cases of spontaneous regression have not been reported. Partial or total surgical excision or an intralesional injection with triamcinolone is the most common treatment option for NF. It seldom relapses, but the diagnosis should be reviewed if that happens.14,15
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.