
Abstract
With the broad indications for dental implantation, complications rates have increased. Dental implant displacement into the maxillary sinus, although rare, can occur during the restoration of maxillary posterior teeth. We performed a 6-year retrospective review and found 3 cases with displaced implants in the maxillary sinus. Detailed information, including surgical indications and dental implant removal methods, is provided. Dental implants can be dislocated to the maxillary sinus perioperatively or postoperatively. Endoscopic sinus surgery can be performed to remove the implant and restore sinus patency. If the implant is displaced to deeper areas (commonly anterior and inferior) of the maxillary sinus, a prelacrimal recess approach can provide a panoramic view of the maxillary sinus and is a good alternative to the Caldwell-Luc operation in terms of mucosal preservation and postoperative complications.
Introduction
Dental implants have been used for oral rehabilitation in edentulous areas. However, posterior edentulous alveolar ridges may not be a suitable area for implant placement since rhinosinusitis or implant displacement is possible. Displacement of a dental implant may occur under conditions of insufficient stability during implantation or a lack of osseointegration after the procedure. 1 Currently, bone lift is a common procedure in patients with inadequate bone height. Nevertheless, the migration of dental implants remains possible.
For patients with displaced dental implants, even though infection does not always occur, removal of the foreign body is suggested. 1 Intraoral approaches have the advantages of concurrent closure of oroantral fistulas. Endoscopic sinus surgery (ESS), performed by an otolaryngologist, can provide foreign body removal, treatment of rhinosinusitis, and establishment of a patent maxillary ostium. 2 Endoscopic sinus surgery (ESS) has been proposed as the preferred procedure for the removal of dislodged dental implants. 3
Between December 2013 and December 2019, 3 cases with dental implant displacement to the maxillary sinus underwent ESS with an uneventful recovery. We adopted a prelacrimal recess (PLR) approach for the third case when the implant was located in the anterior and inferior part of the maxillary sinus. In this report, we also discuss different techniques to remove the maxillary displaced dental implant with a brief literature review.
Case Series
This study was approved by the institutional review board of the Chang Gung Memorial Hospital. We treated 3 patients with dental implant dislocation to the maxillary sinus between December 2013 and December 2019. Two patients were referred from dentists. All 3 patients received ESS with endoscopic maxillary antrostomy. Two dental implants were removed from the widened maxillary ostium, and case 3 was retrieved via an additional PLR approach. The PLR approach, initially described by Zhou et al, 4 provides the advantage of an excellent surgical field and access to the maxillary sinus, as well as handling of intrasinus lesions mostly with a 0° endoscope by creation of an inferior turbinate and nasolacrimal duct flap.
Three patients were followed up for 4 to 12 months (mean 7.3 months). No complication was noted during the follow-up period.
Case 1
A 55-year-old female with a history of left second molar dental implantation 2 years ago had nasal foul odor for 1 month. Oral examination showed a loose left upper second molar. Due to a lack of response to medical therapy, a computed tomography (CT) examination was performed. A high-density foreign body was noted in the center of the left maxillary sinus with total opacification (Figure 1A). Endoscopic sinus surgery was then performed several days later. A dental implant was visualized after wide maxillary antrostomy and was removed without incident (Figure 2A).
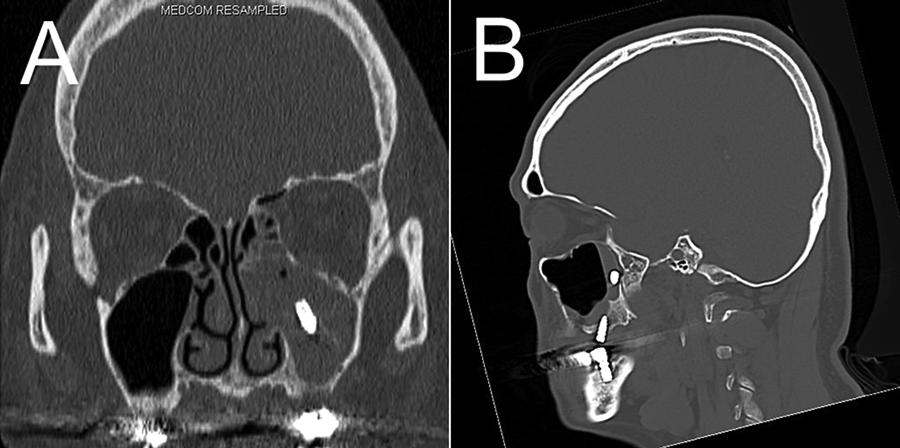
Computed tomography scans showing a metallic foreign body in the center of the left maxillary sinus in case 1 (A) and on the left maxillary posterior wall in case 3 (B), 362 × 180 mm (300 × 300 dpi).
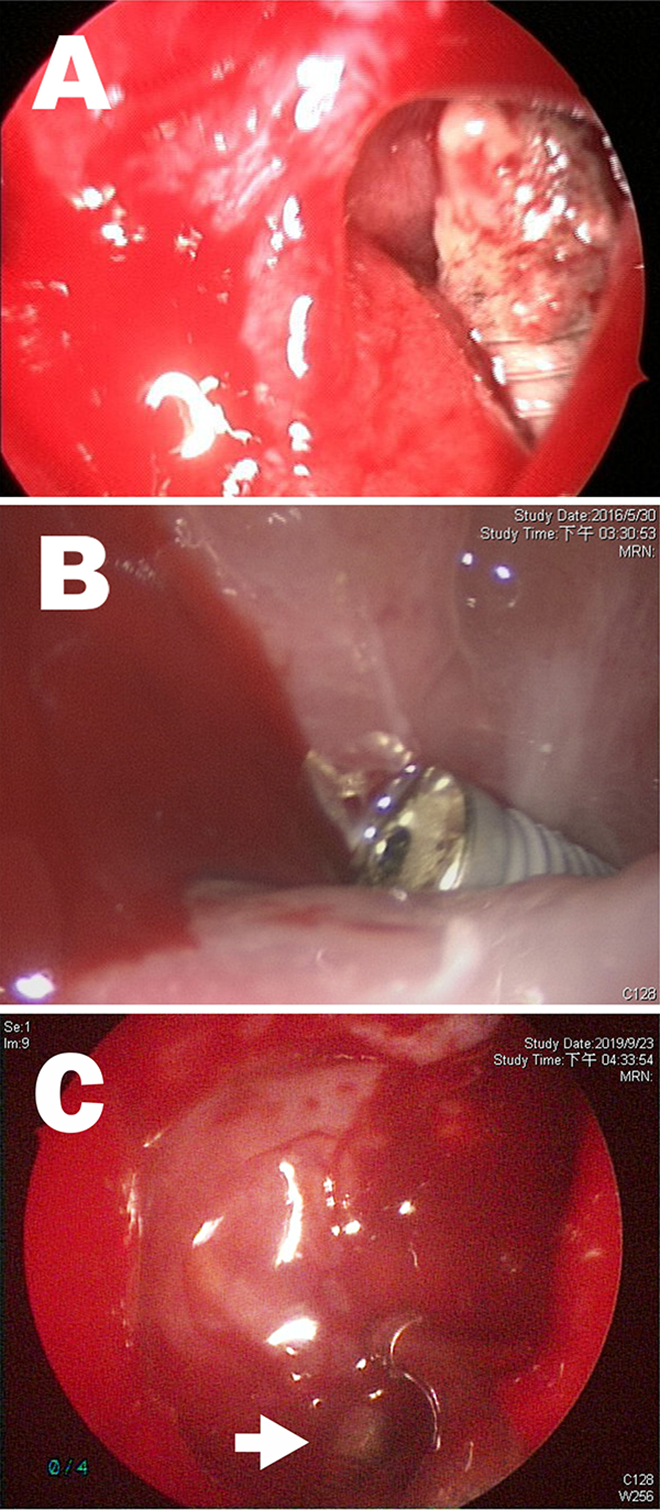
A, A displaced dental implant was visualized after maxillary antrostomy. B, The dental implant was observed with a 45° endoscope through a previously created antrostomy. C, The endoscopic prelacrimal recess approach provided a good surgical field in the anterior and inferior maxillary sinus, and the dental implant was clearly visualized (arrow).
Case 2
A 50-year-old female was originally referred from the dentist due to refractory rhinosinusitis after a sinus lift. Left ESS was performed and a wide maxillary antrostomy was made. Two years later, dental implantation was performed, but the prosthesis dislocated to the maxillary sinus perioperatively, and the patient was referred to our department. Under general anesthesia, the implant was removed via a previously created maxillary antrostomy (Figure 2B). Swollen maxillary sinus mucosa was observed.
Case 3
A 60-year-old male was referred from the dentist due to displacement of a dental implant perioperatively into the left maxillary sinus. Sinus CT was performed and a metallic foreign body was found abutting the left maxillary sinus posterior wall (Figure 1B). Removal of the dental implant was performed 3 days later. After wide maxillary antrostomy, we did not observe the implant even with a 90° endoscope. A PLR approach was then performed. After creating an inferior turbinate and nasolacrimal duct flap, the medial bony wall of the maxillary sinus could be fully exposed. After removing the medial wall, a panoramic view of the maxillary sinus could be obtained. The implant was located in the lacrimal recess of the maxillary sinus (Figure 2C) and was removed without incident.
Discussion
The causes of dental implant displacement to the maxillary sinus can be classified according to the time dislocation occurs, which is most common during the operation. In our cases, 2 dislocations occurred perioperatively, while the other occurred 2 years postoperatively. Perioperative displacement is often associated with incorrect surgical planning, including placement of implants in sites with inadequate bone height and volume, surgical inexperience, improper surgical procedures such as overpreparation of the recipient site, applying a heavy force during implant insertion, or sinus membrane perforation during the drilling procedure.1,5 Late displacement is rare and usually occurs within 6 months of implantation. 6
Computed tomography is a useful tool for identifying the presence and location of dental implants in the maxillary sinus. Ramotar et al 7 described the application of image-guided endoscopic removal of a dental implant from the maxillary sinus. However, the implant can migrate and may not be present at the same location as seen on CT, as demonstrated in case 3. Detailed endoscopic inspection of the maxillary sinus should be performed if the implant is not identified at the expected location. In case 3, the PLR procedure provided a good anterior and inferior endoscopic view and was used to localize the foreign body.
It has been suggested that displaced dental implants should be removed as soon as possible. However, foreign bodies do not always cause rhinosinusitis. Chiapasco et al 8 showed that 14 of 27 patients did not have relevant foreign body reaction/infection in the affected maxillary sinus. However, late sinusitis could develop years after implant displacement. 9 In addition, displaced foreign bodies may migrate to other anatomic sites such as the ethmoid sinus, orbital floor, sphenoid sinus, and cranial fossa.8,10-12 Thus, timely removal is mandatory.
Displaced dental implants can be removed using intraoral and intranasal approaches. The intranasal approach is often referred to as ESS or the modified endoscopic procedure. Intraoral approaches may include the Caldwell-Luc operation, suction of the foreign body from the oroantral fistula, or the lateral window approach. 13 The intraoral approach has the advantage of facilitating foreign body removal as well as closing the oroantral fistula. However, it does not provide effective treatment to the obstructed sinus ostium and accompanying sinusitis. ESS may necessitate interdisciplinary cooperation and additional oroantral fistula closure. 13 ESS is considered an effective and minimally invasive method to retrieve the implant, but it may be difficult to remove implants located in the anterior and inferior parts of the maxillary sinus. In difficult areas that cannot be approached with an endoscope, the Caldwell-Luc operation is a reasonable alternative. 1 However, the Caldwell-Luc operation may cause postoperative complications such as facial swelling, dysesthesia of the infraorbital region, numbness of the maxillary teeth, and injury to the orbital floor.3,14 Jin et al described a modified endoscopic procedure to remove the displaced implant by creating a small hole in the inferior nasal meatus. 13 However, the endoscopic view from the widened maxillary sinus ostium may be limited due to extensive pneumatization of the maxillary sinus or swollen mucosa. Since the introduction of PLR by Zhou et al, 4 it has been commonly used to treat various lesions in the maxillary sinus, including inverted papilloma, pterygopalatine or intratemporal fossa schwannoma, and recurrent antrochoanal polyps.7,15,16 In a multicenter study, where inverted papilloma was resected using the PLR approach, a rate of 7.04% (5 of 71) was noted for facial numbness, much lower than that with the Caldwell-Luc approach. 17 In case 3, this approach offered benefits both in foreign body localization and removal, without subsequent postoperative complications.
Conclusion
ESS is an effective and minimally invasive method to remove displaced dental implants and restore sinus health. Computed tomography can be used to localize a foreign body, but it may migrate prior to the operation. The PLR approach offers a direct and panoramic view of the maxillary sinus and can assist with the removal of difficult-to-reach foreign bodies. Multidisciplinary cooperation between otolaryngologists and oral surgeons can improve treatment results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.