
Abstract
Background:
It is believed that carrying out laryngectomy in tracheotomized patients leads to higher postoperative complications and stomal recurrence compared to carrying out the procedure upfront without prior tracheotomy. We believe that emergency laryngectomy is a feasible procedure in most cancer centers and can be carried out for indications beyond acute airway obstruction as well and complex reconstruction procedures can be also carried out simultaneously. We hereby describe our experience with emergency laryngectomy with or without pharyngectomy.
Methods:
Retrospective analysis of prospectively maintained data base was carried out. Patients who had undergone emergency laryngectomy in our department, from 2014 to 2018, were analyzed, and their clinicodemographic and histopathological features were noted. The indications for surgery and postoperative complications were charted down. Survival data of patients were also noted.
Results:
Seven patients have undergone emergency laryngectomy, 5 for acute airway obstruction and 2 for acute bleeding. Five patients were chemoradiotherapy failures, whereas 2 patients were operated upfront. Two out of 7 patients had pyriform fossa carcinoma, whereas rest of the patients had carcinoma of glottis. Reconstruction with pectoralis myocutaneous/pectoralis muscle only flap was carried out in 4 patients. Minor salivary leak was noted in 4 patients at varying time intervals from second week onward. Two patients had post radiotherapy chondroradionecrosis, without any residual/recurrent tumor. Three out of 7 patients developed recurrence which was salvageable in only 1 patient.
Conclusion:
Emergency laryngectomy can be safely carried out in emergency setting in most cancer centers, more so over it can be carried out for indications beyond acute airway obstruction and combined with complex reconstruction procedures.
Introduction
Total laryngectomy (TL) is a standard surgical procedure, which is being done for advanced laryngeal cancers, although of late definitive chemoradiotherapy (CTRT) has been established as a standard of care for T3 and select T4 laryngeal lesions, as a part of organ preservation strategy. 1 However, even in present era of organ preservation, TL is reserved for patients with cartilage invasion, dysfunctional larynx, and as a salvage for CTRT failure. There is a debate about carrying out this definitive procedure in emergency setup in patients with life-threatening compromised airway, who otherwise undergo tracheotomy (as a measure to secure airway) before undergoing definitive surgery in a planned manner. There are few old reports of emergency TL as it was believed that carrying out laryngectomy in previously tracheotomized patients leads to higher postoperative complications and stomal recurrence compared to carrying out the procedure upfront without prior tracheotomy.2,3 Emergency TL has been primarily described in few case series primarily for acute airway obstruction.4-6 Moreover, these series lack homogenous sample structure, and emergency TL was carried out for both T3 and T4 lesions. We hereby describe our experience with emergency laryngectomy with or without pharyngectomy and complex reconstruction procedures.
Materials and Methods
This study was carried out at Regional Cancer Centre of Sher-i-Kashmir Institute of Medical Sciences, which is a tertiary care referral centre with dedicated oncologic services. We have a prospectively maintained data base for all operated patients and retrospective analysis of this data base was carried out after obtaining permission from institute’s Ethics committee. Patients who had undergone emergency laryngectomy TL in our department, from 2014 to 2018, were analyzed. All the patients who underwent emergency laryngectomy had been evaluated prior to their surgery, through a standard protocol consisting of history/examination, office laryngoscopy, and contrast-enhanced computed tomography (CT) of neck and chest, magnetic resonance imaging of neck (if indicated), and/or positron emission tomography (PET). All the patients had biopsy documented laryngeal malignancy, except in patients with dysfunctional larynx, in whom biopsy was not deemed necessary. “Dysfunctional larynx” was defined as one causing complete airway obstruction and/or hemorrhage, with or without chondroradionecrosis. All of these patients had PET-CT done, which read as weekly positive. Post-surgery patients were discussed in multidisciplinary joint tumour board meet for further treatment. Patients were followed every 6 weeks initially for 6 months, followed by every 3 months from 6 month onward. The data related to patient’s demographic profile, clinical presentation, surgical procedure, postoperative course, and surveillance were retrieved from the database and analyzed.
Results
Seven patients underwent emergency TL during the study period (2014-2018). Clinicodemographical details of patients are shown in Table 1. Five patients were radiotherapy/CTRT failures, whereas 2 patients were operated upfront, without prior treatment. Two out of 7 patients had carcinoma of pyriform fossa whereas rest of the patients had glottic tumors. Five patients were operated for acute airway obstruction and 2 for severe acute bleeding. One of the patients who was operated for bleeding was found to have eroded superior thyroid artery and necrotic thyroid lamina-chondroradionecrosis (Figure 1 and Figure 2). Reconstruction with pectoralis myocutaneous (PMMC)/pectoralis muscle only flap was carried out in 4 patients; 1 patient underwent total laryngopharyngectomy and reconstruction with tubed PMMC flap. Minor salivary leak was noted in 4 patients at varying time intervals from second week onward, which settled with conservative management. Two patients who received upfront surgery also underwent neck dissection. Pathological parameters of patients are shown in Table 2. Two patients had post radiotherapy chondroradionecrosis, without any residual/recurrent tumour, one of these patients was operated for acute bleeding and other for airway obstruction. Three out of 7 patients developed recurrence which was salvageable in only 1 patient. Recurrence pattern and current status of study patients in detailed in Table 3.
Clinicodemographic Details of Patients Undergoing Emergency Laryngectomy.
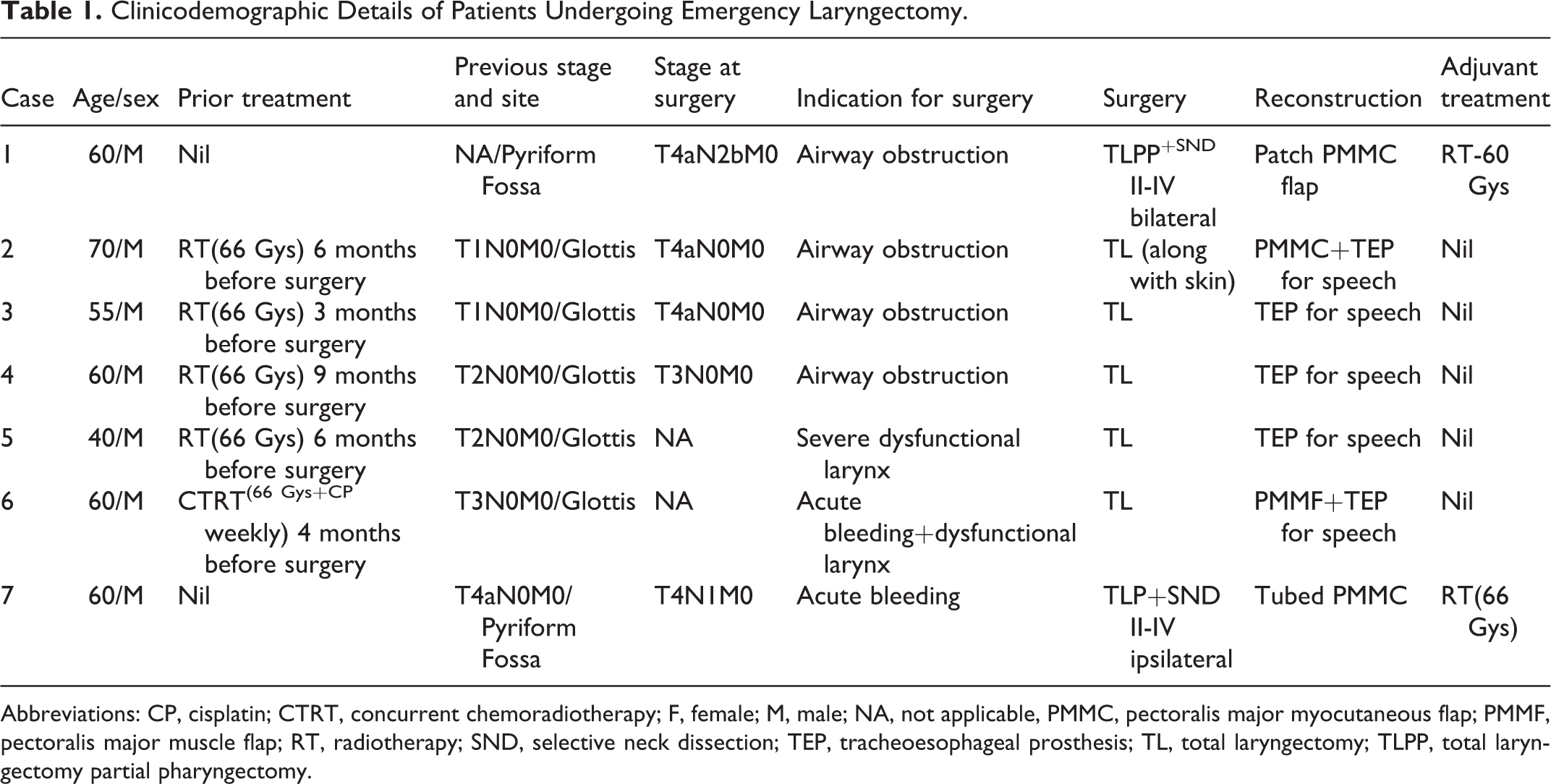
Abbreviations: CP, cisplatin; CTRT, concurrent chemoradiotherapy; F, female; M, male; NA, not applicable, PMMC, pectoralis major myocutaneous flap; PMMF, pectoralis major muscle flap; RT, radiotherapy; SND, selective neck dissection; TEP, tracheoesophageal prosthesis; TL, total laryngectomy; TLPP, total laryngectomy partial pharyngectomy.
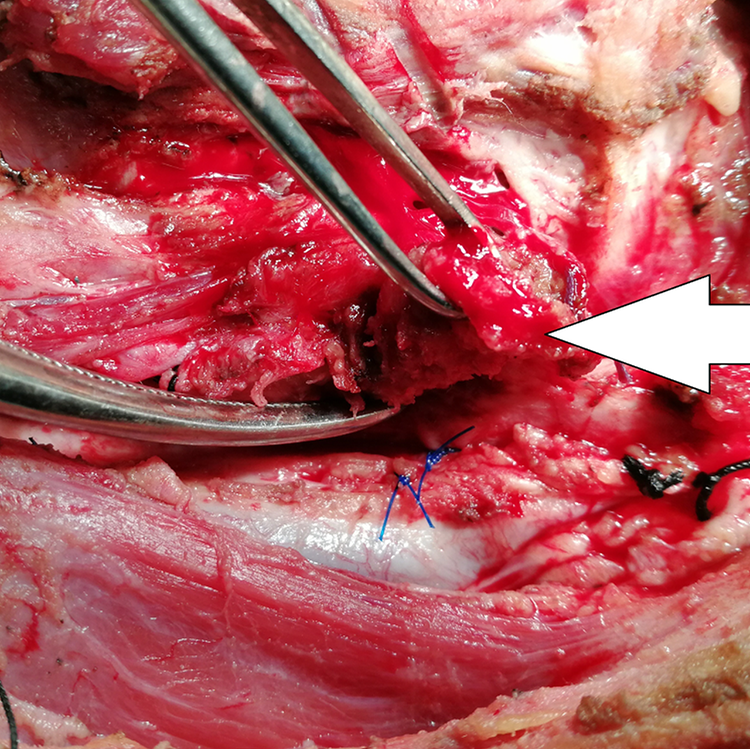
Figure showing eroded superior thyroid artery (white arrow).
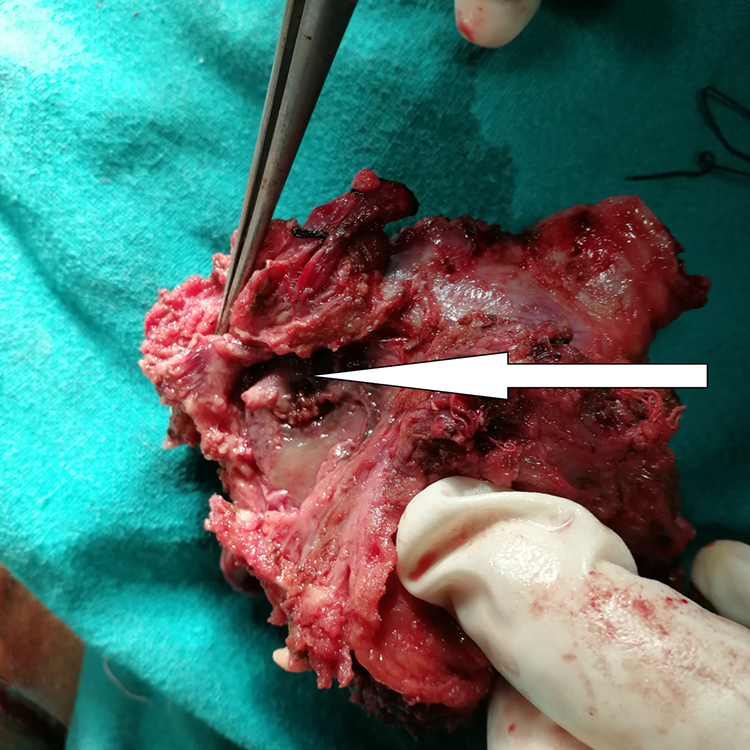
Figure showing necrotic thyroid cartilage lamina (white arrow).
Histopathological Features and Lymph Node Levels Involved in Patients Undergoing Surgery.
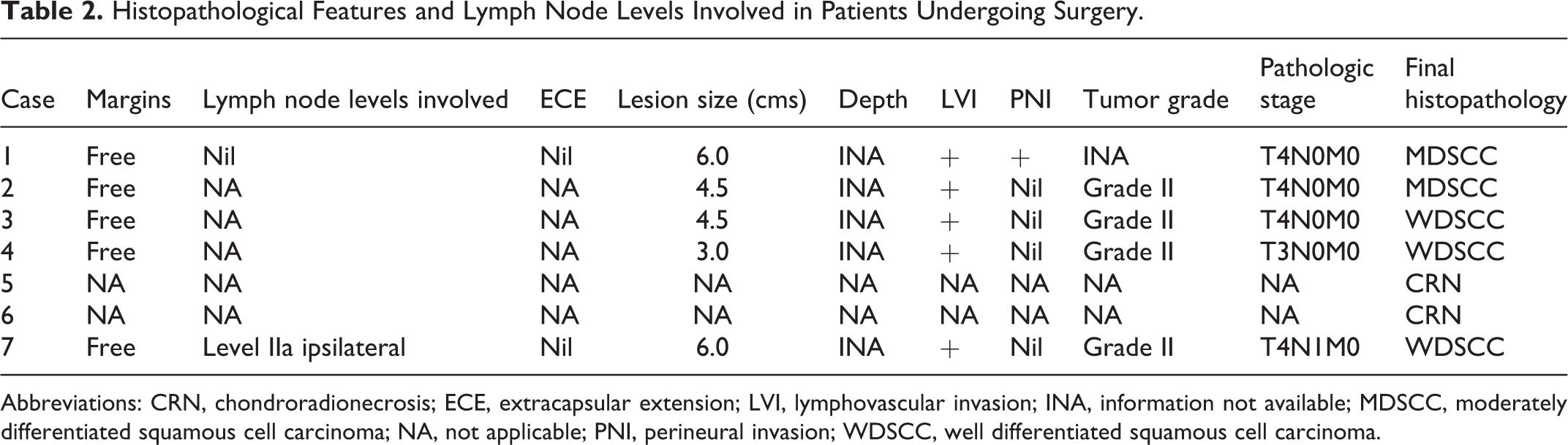
Abbreviations: CRN, chondroradionecrosis; ECE, extracapsular extension; LVI, lymphovascular invasion; INA, information not available; MDSCC, moderately differentiated squamous cell carcinoma; NA, not applicable; PNI, perineural invasion; WDSCC, well differentiated squamous cell carcinoma.
Patterns of Recurrence Before and After Surgery, and Current Patient Status.
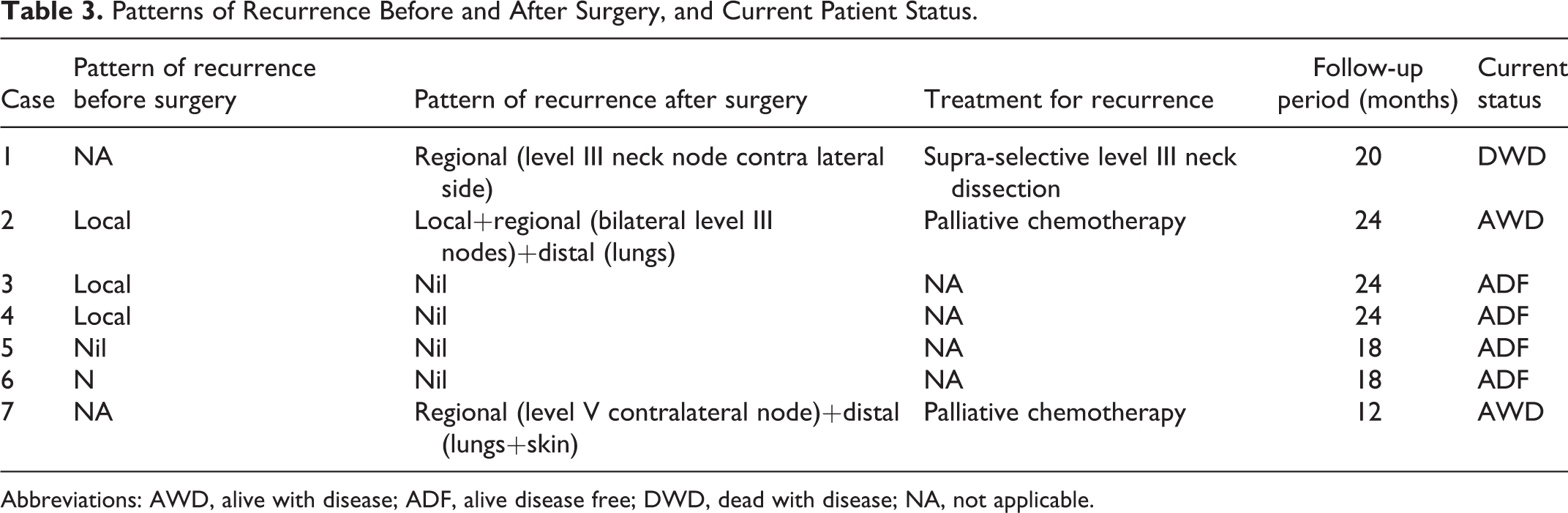
Abbreviations: AWD, alive with disease; ADF, alive disease free; DWD, dead with disease; NA, not applicable.
Discussion
Emergency TL has been reported previously, but has not been prevalent in more recent medical literature. One of the potential advantages of this treatment philosophy is that it reduces stomal recurrence rate and postoperative complications. We believe that the procedure can be safely carried out in emergency setting in most tertiary cancer referral centers, more so over it can be carried out for indications besides acute airway obstruction and combined with complex reconstruction procedures.
It is believed that preoperative tracheotomy is a risk factor for stomal recurrence. Preoperative tracheotomy favors the implantation of the viable desquamated tumor cells in the stomal area and the risk of stomal recurrence after carrying out a tracheotomy prior to definitive treatment varies between 8% 2 and 41%. 3 Zhao et al 7 reported on 548 patients who had undergone laryngectomy to identify the risk factors associated with stomal recurrence. It is to be noted that 18% of these patients had T2 lesions. Emergency tracheostomy was done in 38.9% of patients, before embarking on definitive surgical procedure. After a median follow-up period of 6.3 years, stomal recurrence developed in 48 (8.8%) of 548 patients. The mean interval between the laryngectomy and stomal recurrence was 9.1 months and ranged from 52 days to 39 months. Although 8 of these stomal recurrence patients were operated, 44 died of disease, with median time to death of 9.2 months with a range of 2 to 11 month. In the preoperative tracheostomy group, 30 (14.1%) out of 213 patients developed stomal recurrence compared with 18 (5.4%) out of 335 in the operative tracheostomy group. On univariate analysis, preoperative tracheostomy was statistically significant factor for stomal recurrence. However, there were no stringent criteria for postoperative radiotherapy or chemoradiotherapy. Only 193 out of 288 patients with positive surgical margins or/and lymph node invasion received postoperative chemoradiotherapy. Imauchi et al 8 reported on risk factors associated with stomal recurrence and noted that patients with preoperative tracheostomy were at higher risk of getting stomal recurrence than patients who were not tracheotomised before surgery (33% vs 6%). The incidence of stomal recurrence was higher in the patients with paratracheal lymph node metastases (29% vs 6%). According to the correlation analysis, there was a significant correlation between paratracheal lymph lymphadenopathy and preoperative tracheotomy (P < .01). Yotakis et al 9 noted that 21 patients out of 352 patients who had undergone TL developed stomal recurrence. Emergency tracheotomy was performed in 7 of these patients. Similarly, Esteban et al 10 reported on 309 patients and noticed that stomal recurrence occurred in 25% (9 of the 36) patients with preoperative tracheotomy compared to 4.6% of patients who had intraoperative tracheotomy (Relative Risk = 5.38; CI = 2.22-12.99). On logistic regression analysis prior tracheotomy, pathological T-stage and site of primary tumor were found to be independently related to stomal recurrence. Rockley et al 11 analyzed primary T3N0M0 carcinoma glottis patients who had undergone TL without postoperative radiotherapy. Out of total 91 patients, 26 had undergone preoperative tracheotomy, with stomal recurrences being more frequent in preoperative tracheotomy group (P <.01). Age-adjusted 5-year survival was statistically worse in preoperative tracheotomy group (20% vs ∼ 60%). Contrary to this, Mantravardi et al 12 did not find any correlation between the appearance of stomal recurrence and the practice of tracheotomies prior to radical surgery. They noted stomal recurrence in 26 patients out of 507 cases. Stomal recurrence rate was 6% in emergency tracheotomy group compared to ∼ 5% in peroperative tracheotomy group. Rubin et al 13 analyzed data from 444 carcinoma larynx patients who had undergone partial or TL, and noted stomal recurrence in 15 (3.4%) patients. In 46 patients with subglottic tumors, recurrence was noted in 4 out of 13 patients who had preoperative tracheotomy, compared to 8 out of 33 patients who had operative tracheotomy. The difference was not statistically significant. Although higher stomal recurrence in previously tracheotomized patients may not be statistically significant in all the reported articles, it is evident that published literature weighs in favor of higher stomal recurrence in preoperatively tracheotomized patients.
Emergency laryngectomy being a procedure carried out without previous tracheotomy can reduce the risk of stomal recurrence and reduce postoperative complications. Griebie et al 4 noted one stomal recurrence in 16 patients who had undergone emergency laryngectomy compared to 10 stomal recurrences in 281 patients who had elective laryngectomy. Wickham et al 5 performed 13 emergency laryngectomies and reported no stomal recurrences. McCombe et al 6 compared 2 groups of patients, group I who had undergone emergency laryngectomy (n = 31) and group II who had undergone elective laryngectomy (n = 202). They found no statistically significant difference between the 2 groups in early postoperative mortality (6.5% vs %), stomal recurrence rates (4.2% vs 4.8%), and survival (53% vs 55%). However, it is not mentioned as to how many patients in the elective laryngectomy group had preoperative tracheotomy. As can be deducted from the above quoted literature, sample composition of these studies has not been homogenous and emergency TL has been carried out for lesions which can been treated with CTRT in present day world, sparing the patient of laryngectomy contrary to this, in our study only patients with voluminous T4 lesions and post CTRT failures have been treated with emergency TL. In our reported case series, we did emergency laryngectomy for indications beyond acute airway obstruction and simultaneously complex reconstruction was also done when needed. Although we did not encounter any significant morbidity or any postoperative mortality, morbidity and mortality data of emergency laryngectomy patients were not compared with patients who had undergone elective laryngectomy with or without previous tracheotomy, because of limited number of patients in the former group. It is to be noted that historical data is dominated by reports of lower postoperative morbidity and mortality if preoperative tracheotomy can be avoided.
Conclusion
We believe that emergency laryngectomy is a safe and feasible procedure in most tertiary cancer referral institutes. Emergency TL can be carried out for indications besides acute airway obstruction and can be combined with complex reconstruction procedures. However more well-designed prospective studies need to be carried out to establish its purported advantages over elective pretracheotomized laryngectomy patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.