
Abstract
Objective:
To identify factors influencing time-to-operating room and time-to-airway intervention in urgent tracheotomy and synthesize strategies to reduce delays in airway emergencies.
Methods:
A scoping review was conducted following the Joanna Briggs Institute framework and reported according to PRISMA-ScR guidelines. MEDLINE, Embase, Scopus, Web of Science, and Google Scholar were searched from inception to June 2024. Eligible studies involved adults (≥18 years) undergoing urgent tracheotomy for airway obstruction due to malignancy or infection. Trauma, angioedema, laryngotracheal stenosis, post-radiation edema, and vocal fold paralysis were excluded to reduce heterogeneity and focus on institutional/system-level factors.
Results:
Of 1339 records identified, 3 studies (n = 531 patients) met the inclusion criteria. Dyspnea and stridor were the most common presenting symptoms. Malignancy and deep neck infection accounted for most indications. Reported delays were related to operating room access, staffing shortages, and coordination challenges. Complication rates ranged from 8% to 28%, with hemorrhage and infection most frequent; no deaths were directly attributed to tracheotomy. Decannulation rates were higher in non-malignant than in malignant cases.
Conclusions:
Urgent tracheotomy for airway obstruction due to malignancy or infection is time-sensitive, with delays shaped by institutional barriers. Standardized protocols, improved staffing, simulation-based training, and rapid-response teams represent actionable strategies to enhance airway emergency readiness and outcomes.
Keywords
Introduction
Acute airway obstruction is a common scenario in clinical otolaryngology, requiring timely surgical intervention and a multidisciplinary approach. In such scenarios, collaboration between otolaryngologists, anesthesiologists, trauma surgeons, and emergency physicians is crucial to optimize patient outcomes.1 -4
Acute airway obstruction is a life-threatening situation that can rapidly worsen and result in death if a surgical airway is not obtained in a timely manner.5 -7
In emergency airway management, securing a surgical airway is critical, with front-of-neck access options including tracheostomy, cricothyrotomy, and needle airway techniques. Among these, tracheostomy is the preferred option in scenarios requiring prolonged airway control due to its superior long-term safety and effectiveness.8,9 While cricothyrotomy is often recommended for rapid airway access in “can’t intubate, can’t oxygenate” (CICO) situations, it is associated with a high rate of complications, including subglottic stenosis, tube misplacement, and airway obstruction, making it unsuitable for prolonged use.10,11 Furthermore, needle cricothyrotomy, although minimally invasive, provides inadequate ventilation over extended periods, often leading to barotrauma, failed oxygenation, and eventual conversion to a more definitive airway.9,12 These advantages highlight the need for prompt decision-making, with tracheostomy prioritized when prolonged airway support is required. 8
Timely airway management is critical for optimizing outcomes in patients requiring urgent tracheotomy. Studies show that delays in these metrics are associated with higher ICU mortality, prolonged ventilation, and increased complications.13 -15
Delays in securing a surgical airway, particularly tracheostomy, have been associated with catastrophic outcomes such as hypoxia and mortality, though causality remains uncertain due to potential confounding factors. For otolaryngologists managing airway emergencies, this gap hinders timely care. This scoping review examines factors influencing time-to-operating room (time-to-OR) in urgent airway cases to identify actionable strategies that improve decision-making, logistics, and patient outcomes.
Methods
This scoping review followed the Joanna Briggs Institute methodological framework, which includes 5 stages: (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, and (5) collating and reporting results. 16 The PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) checklist guided reporting, which does not require PROSPERO protocol registry.
Research Question
Using the PICO framework, the guiding question was: What factors, patient survival rates, and clinical outcomes (O) are associated with early (I) versus delayed (C) tracheotomy in adults with airway obstruction due to malignancies or infections (Population), regardless of setting (ICU, bedside, OR)?
Search Strategy
A comprehensive search was conducted on June 1, 2024, across MEDLINE/PubMed, Embase, Web of Science, and Scopus. Google Scholar was used for gray literature. A McGill University medical librarian developed the strategy using MeSH and free-text terms related to “emergency,” “tracheotomy,” “surgical airway,” and “urgent” (Supplemental Table 1). All studies from inception to the search date were considered.
Eligibility Criteria
Inclusion
Studies involving adults (≥18 years) undergoing urgent tracheotomy for airway obstruction due to malignancies or infections, across all care settings.
Exclusion
Studies not in English, lacking data on procedural timing or outcomes, or involving trauma-related obstruction. Non-peer-reviewed formats (eg, book chapters, conference abstracts, and letters) were also excluded. We also excluded cases of angioedema, laryngotracheal stenosis, post-radiation edema, and bilateral vocal fold paralysis. These conditions were excluded because their pathophysiology, urgency, and management differ substantially from malignancy- and infection-related obstructions. Including them would have introduced considerable heterogeneity and confounded the assessment of institutional/system-level factors influencing time-to-OR.
Study Selection
Two reviewers (R.C. and J.G.J.W.) independently screened titles and abstracts, followed by full-text review. Disagreements were resolved by consensus or third-party adjudication (Y.C.). Reference lists of included studies were hand-searched to identify additional relevant articles.
Data Extraction and Analysis
Data extracted included author, year, presenting symptoms, time-to-OR factors, type of airway intervention, and clinical outcomes. To ensure consistency in assessing procedural efficiency, we standardized terminology across included studies. Key time-to measures were defined as follows (Table 1): time-to-tracheotomy, time-to-airway intervention, time-to-OR, and time-to-secured airway. Data were organized in spreadsheets and analyzed using SPSS statistics version 29.0 for macOS to identify patterns related to delay in urgent tracheotomy. 17
Definitions of Time Metrics in Emergency Airway Management.
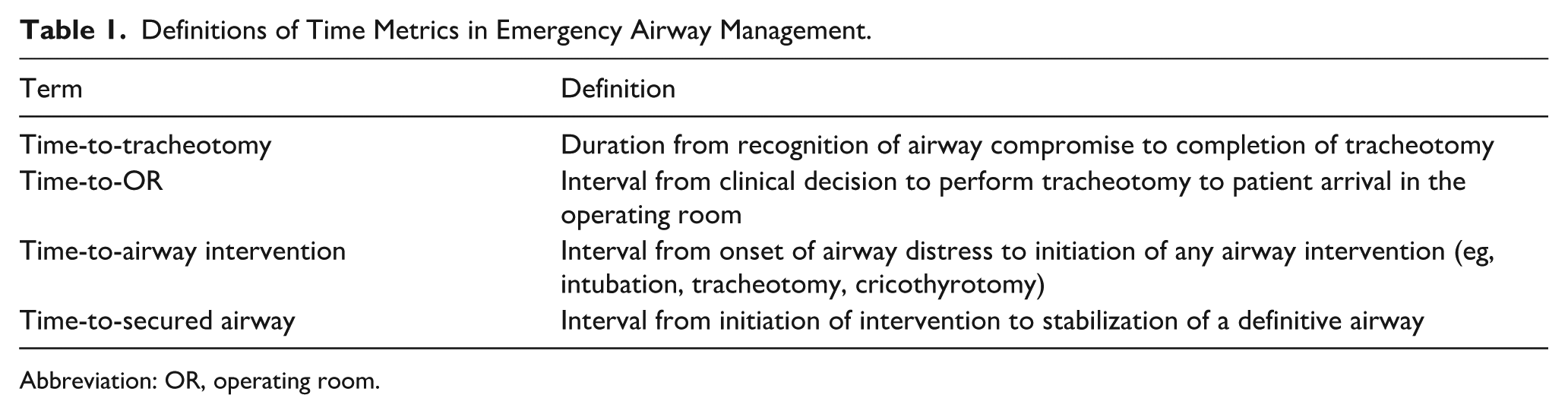
Abbreviation: OR, operating room.
Risk of Bias Assessment
The 3 included studies were evaluated using standard tools for selection, performance, detection, reporting, and other biases.
Results
Overview
The search identified 1339 articles across all databases. After removing 543 duplicates, 836 studies were screened. Twenty-six underwent full-text review, with 23 excluded for reasons such as elective tracheotomy (n = 1), irrelevant outcomes (n = 9), non-aligned interventions (n = 2), unsuitable study design (n = 8), out-of-scope populations (n = 2), or unavailable full-text (n = 1). Three studies met the inclusion criteria and were analyzed8,18,19 (Figure 1).
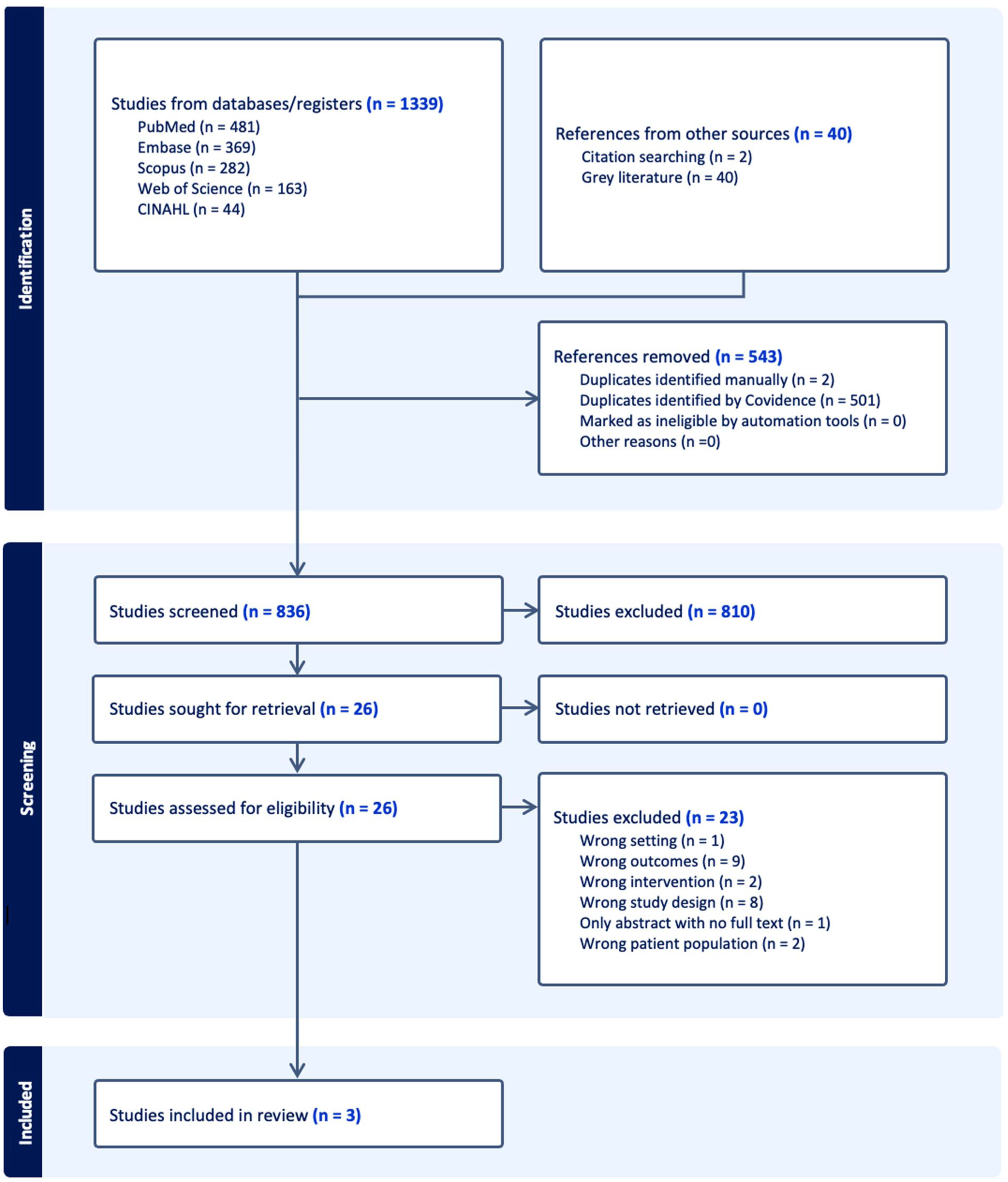
PRISMA flowchart of screening methodology to included studies.
Study Characteristics
The included studies (n = 3) examined urgent tracheotomy for acute airway obstruction across diverse contexts. Sample sizes ranged from 56 to 402 patients. The average age was 60 years, with most patients in their sixth to seventh decade of life (Table 2).
Characteristics and Key Findings of Included Studies on Urgent Tracheotomy.
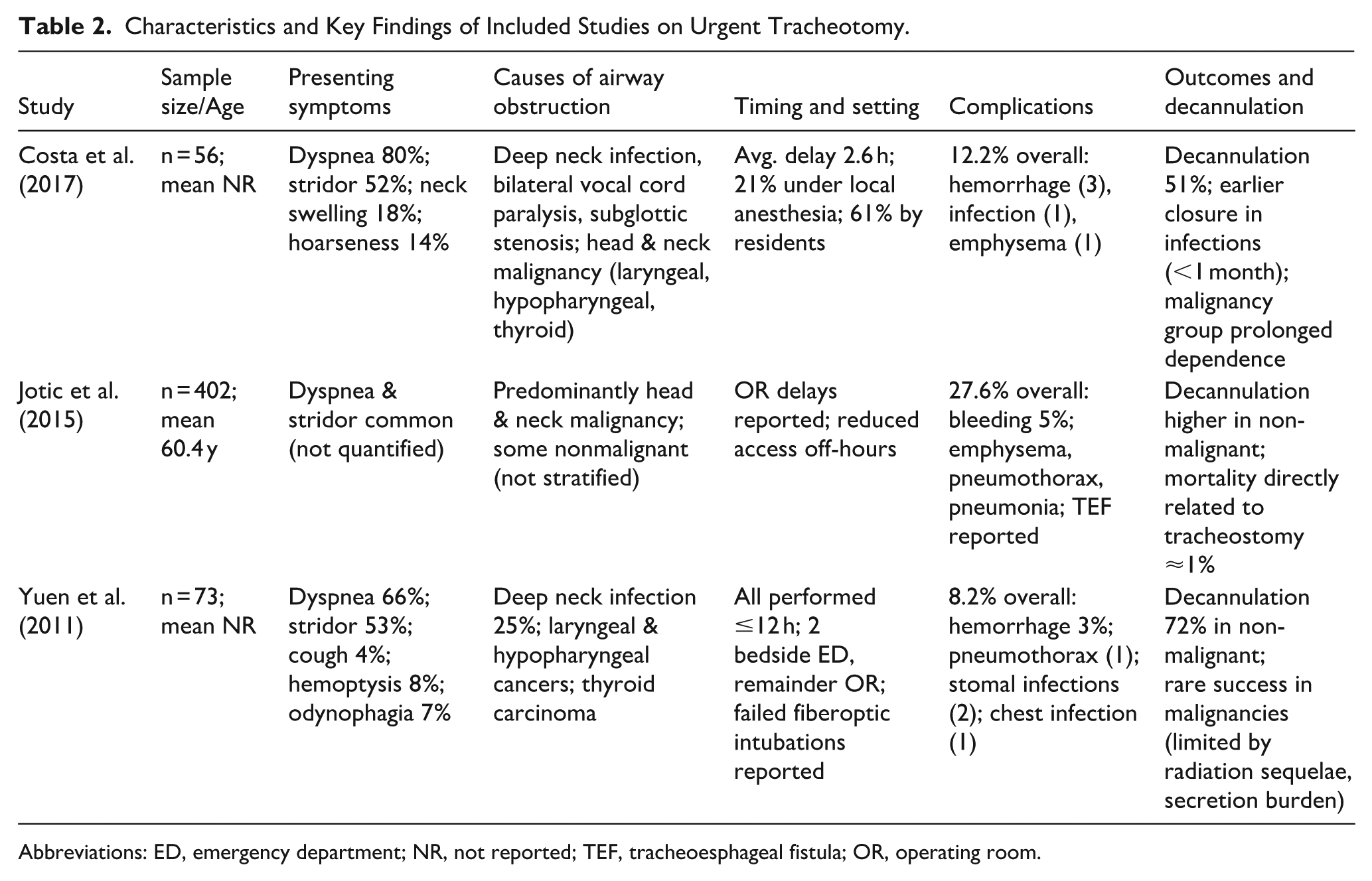
Abbreviations: ED, emergency department; NR, not reported; TEF, tracheoesphageal fistula; OR, operating room.
Presenting Symptoms and Clinical Indicators
Dyspnea (65%-80%) and stridor (52.5%) were the most common presenting symptoms, followed by neck swelling (17.8%), hoarseness (13.7%), and less frequent symptoms such as hemoptysis (8.1%), odynophagia (6.8%) and cough (4.1%).8,18,19 Severe obstruction was reported in ~60% of cases assessed by fiberoptic laryngoscopy. 19
Causes of Airway Obstruction
Both malignant and non-malignant etiologies were reported. Deep neck infections (25%) were the leading non-malignant cause, followed by bilateral vocal cord paralysis and subglottic stenosis. Malignancies—predominantly advanced-stage squamous cell carcinoma of the larynx and hypopharynx—accounted for 27% of cases.8,18,19
Timing and Setting of Tracheotomy
Most procedures occurred within 12 hours of presentation or referral.8,19 Delays were reported in association with OR access and staffing shortages. 18 While tracheotomy was usually performed under general anesthesia, a proportion proceeded under local anesthesia when patients were unstable. Bedside tracheostomies were required in select cases, particularly when intubation failed.18,19
Complications
Overall complication rates ranged from 8% to 28%. Common events included hemorrhage, infection, and subcutaneous emphysema; rare complications included pneumothorax and tracheoesophageal fistula.8,18,19 No deaths were directly attributable to the tracheotomy itself. Predictors of complications included comorbidities, prior radiotherapy, and an emergency bedside setting.
Outcomes and Decannulation
Decannulation rates varied by etiology. Nonmalignant cases (eg, infection) showed higher success (up to 72%) and earlier closure, whereas malignant obstructions often required prolonged tracheostomy, with post-radiation sequelae limiting decannulation.8,19
Risk of Bias Assessment
All 3 studies were retrospective and single-center, with limitations including selection bias, inconsistent reporting of complications, and variability in procedural context. External validity was limited by resource differences and observational study designs (Table 3).
Risk of Bias Assessment of Included Studies.
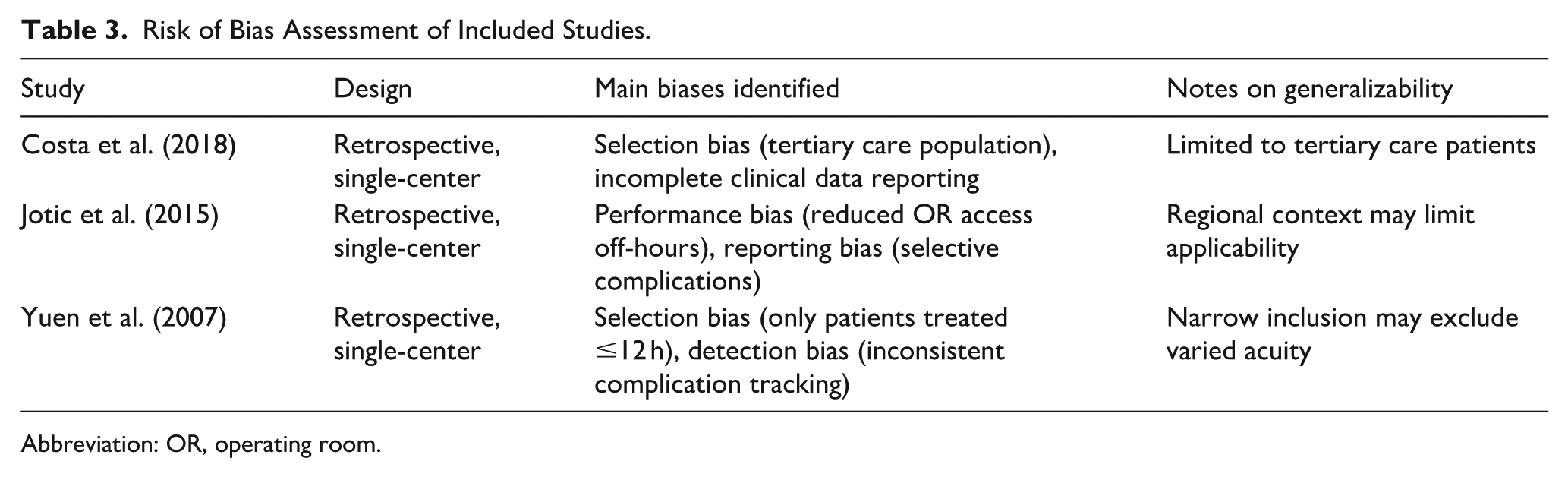
Abbreviation: OR, operating room.
Discussion
Airway management is central to emergency otolaryngology, and timely intervention was consistently associated with improved outcomes8,18,19; however, the evidence is observational and cannot establish causality.
From these studies, older males with oncologic or infectious etiologies predominated.8,18,19 The included studies used non-uniform timing metrics; for example, Costa et al reported a mean delay of 2.6 hours, while Yuen et al applied a ≤12-hour threshold. Jotic et al. inferred delays from procedural location and resource constraints.8,18,19
Simulation data underscore the need for standardized emergency front-of-neck airway (FONA) protocols and multidisciplinary training. 20 Comparisons with alternative techniques were limited across the included studies: Costa et al noted sporadic conversions from cricothyrotomy, Yuen et al reported failed fiberoptic intubations, and Jotic et al focused exclusively on surgical tracheostomies.8,18,19 Nonetheless, cricothyrotomy remains pivotal in CICO scenarios and, per Marcotte et al, should be first line in most cases, with emergency tracheotomy reserved for distorted anatomy or failed cricothyrotomy. 21 At the systems level, broader analyses and difficult airway response teams integrating multiple strategies can strengthen institutional readiness and improve outcomes across airway emergencies.22,23
Operational and patient-related factors influence timing: evening staffing and OR access, procedural location and prior irradiation, and adherence to predefined thresholds.8,18,19 Recurrent barriers include OR availability, interservice coordination, and case complexity. Altman et al. further highlight the potential role of community-based centers in improving access. 24
Beyond the small number of condition-specific studies included here, broader prospective datasets such as the Global Tracheostomy Collaborative provide important complementary evidence. 25 This large international registry demonstrated differences in mortality between acute and elective indications, while also highlighting the benefits of multidisciplinary teamwork, protocol standardization, and patient partnership in improving safety. 25 Although not restricted to malignancy or infection, these data reinforce that delays and adverse outcomes are strongly shaped by system-level factors.
Timely intervention was a consistent theme: urgent awake tracheotomy can be technically challenging (hypoxia, inability to position), yet it reduces hemorrhage and wound infections when not delayed.8,19,26 Institutional context matters—lighting, cautery, positioning, and coordinated teams—to avoid loss of control and complications.18,27
Decision-making drives time-to-OR: malignancy accounted for ~45% of indications in Costa et al; awake tracheotomy for advanced head and neck tumors is complex and complication-prone, while timely awake tracheotomy prevents complete obstruction.8,18,19 Complication rates did not differ between residents and specialists, underscoring the value of structured training and supervised experience in urgent tracheotomy.8,19,28,29
Reported complication rates varied widely (5%-40%) across designs and settings.29 -33 Urgent cases and high-acuity patients carried a higher risk, with hemorrhage and infection most common; nevertheless, immediate and early complication rates of 12% in Costa et al 8 support the overall safety of urgent tracheotomy when performed promptly.
Across studies, delays correlated with higher complication burden, while predictors of adverse outcomes included comorbidities, prior irradiation, neck pathology, and emergency setting.8,18,19
Actionable Recommendations for Reducing Delays
Based on our findings, 4 key strategies can help minimize delays in urgent airway management:
Streamlined Protocols: Clear guidelines for airway emergency management can reduce decision-making delays. These protocols should include criteria for early identification of patients requiring urgent tracheotomy and predefined roles for multidisciplinary teams.
Enhanced Staffing: Addressing staffing limitations during nighttime and weekends could significantly reduce delays.
Simulation Training: Regular simulation exercises improve preparedness across learners. Costa et al and Nguyen et al showed that structured curricula enhance both technical and teamwork skills in trainees, while Sommerfeld et al demonstrated similar benefits for practicing otolaryngologists.8,34,35 Together, these findings support simulation as an essential tool for airway emergency readiness.
Improved Coordination: Establishing rapid-response teams can optimize coordination in airway emergencies. McGrath et al, the largest multicenter QI study, showed mortality reduction with multidisciplinary teams, while Ninan et al, as a systematic review, concluded that interprofessional tracheostomy teams improve safety, reduce adverse events, and shorten hospital stay.36,37 Consensus tools such as Schiff et al further underscore the value of standardized checklists in strengthening institutional readiness. 38
Limitations of Reviewed Studies
The included studies have limitations that must be considered when interpreting their findings. Our exclusion of trauma, angioedema, laryngotracheal stenosis, post-radiation edema, and vocal fold paralysis narrowed the scope but strengthened internal validity by allowing clearer identification of institutional barriers (eg, OR availability, staffing, and coordination) in a more homogenous subset of airway emergencies. This focused approach, however, reduces generalizability.
Large-scale datasets such as the Global Tracheostomy Collaborative highlight differences in mortality across acute and elective indications and provide an important global context that future reviews should incorporate.
Moreover, Costa et al noted the lack of comprehensive clinical data, such as initial symptoms and degree of airway obstruction, which limits external validity. Jotic et al and Yuen et al focused primarily on specific patient populations and procedural contexts, which may not fully capture the variability in time-to-OR delays across different healthcare systems.8,18,19
Because the available studies were retrospective and observational, causality between procedural delays and outcomes cannot be inferred. Associations reported should be interpreted cautiously, as they may reflect unmeasured confounding factors such as disease severity, comorbidities, and institutional practices.
Conclusion
This scoping review highlights the critical need for timely airway management in emergency situations. Delays in airway procedures are associated with worse outcomes, and addressing institutional challenges, standardizing protocols, and enhancing training can significantly improve the timeliness and effectiveness of airway care. Recognizing these predictors can help clinicians refine patient selection and optimize the timing of urgent tracheotomy.
Supplemental Material
sj-docx-1-ear-10.1177_01455613251388399 – Supplemental material for Factors Influencing Time-to-OR for Urgent Tracheotomy: A Scoping Review
Supplemental material, sj-docx-1-ear-10.1177_01455613251388399 for Factors Influencing Time-to-OR for Urgent Tracheotomy: A Scoping Review by Raisa Chowdhury, Jacob G. J. Wihlidal and Yvonne Chan in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
Ms. Eleni Philippopoulos, Assistant Librarian, Undergraduate Medical Education, Schulich Library of Physical Sciences, Life Sciences, and Engineering, McGill University.
Author Contributions
R.C. contributed to the study conception and design, screened articles, and was a major contributor in producing the paper’s original draft as well as subsequent revisions; J.G.J.W. contributed to the study conception and design, screened articles and substantively revised the manuscript; and Y.C. contributed to the study conception and design, screened articles, supervised, and substantively revised the manuscript. All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.