
Abstract
Objectives:
Treatment effects in patients with laryngeal squamous cell carcinoma may vary significantly even among those with the same TNM stage. Routine preoperative blood and coagulation tests are economical and easily available hematological indicators. This study aimed to investigate the clinical predictive significance of pretreatment evaluation of plasma fibrinogen (FIB) level, neutrophil-to-lymphocyte ratio (NLR), and platelet-to-lymphocyte ratio (PLR) in patients with laryngeal carcinoma.
Methods:
Clinicopathological and demographic data from 203 patients who underwent surgery for laryngeal carcinoma were collected and analyzed. The optimal cutoff values for FIB, NLR, and PLR were determined using receiver operating characteristic curve analysis. Univariate and multivariate Cox regression analyses were used to study the relationship between blood markers and patient survival.
Results:
The optimal cutoff values for FIB, NLR, and PLR were 3.05 g/L, 2.41, and 110.94, respectively. Preoperative hyperfibrinemia (FIB >3.05 g/L) was an independent prognostic factor for overall survival (OS) and disease-free survival in patients with laryngeal carcinoma. An NLR >2.41 was associated with reduced OS in patients with laryngeal carcinoma, while PLR >110.94 had no effect on prognosis in these patients.
Conclusions:
Fibrinogen and NLR were valuable markers in predicting survival in patients with laryngeal carcinoma and may be used to inform clinicians in designing individual treatment strategies.
Introduction
Laryngeal squamous cell carcinoma (LSCC) remains a prevalent malignant tumor of the head and neck and ranks second in the incidence of respiratory tumors. In 2018, 12 410 new cases of laryngeal cancer and 3760 cancer-related deaths were reported in the United States. 1 Currently, the main treatments for LSCC include surgery, chemotherapy, radiotherapy, or multimodal therapy. Despite advances in medical technologies, however, the survival and recurrence rates of laryngeal cancer have not improved significantly.
The relationship between inflammatory response and/or systemic immune status and malignant tumor development has recently become a “hot topic.” In the past few years, inflammatory indexes, such as neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio, and platelet-to-lymphocyte ratio (PLR), have been demonstrated to be associated with prognosis in many solid tumors including breast, colorectal, esophageal, and cervical cancers.2-5 In addition, hematological indexes, such as red cell distribution width, plasma fibrinogen (FIB), mean platelet volume, albumin globulin ratio, and C-reactive protein, have also been studied as prognostic and prediction indexes in various types of cancer.6-10 Hematological indexes are common, economical, and simple markers used in the clinic. However, few studies have investigated the utility of these markers for predicting prognosis in patients with laryngeal cancer.
This study aimed to explore the clinical predictive value of preoperative FIB, NLR, and PLR in patients with LSCC to provide a reference for clinicians to design better treatment strategies.
Patients and Methods
Patients
Clinical data from 264 patients with newly diagnosed LSCC, who underwent surgical treatment in the First Affiliated Hospital of Wenzhou Medical University (Wenzhou, Zhejiang, China) between December 2008 and September 2014, were collected. Individuals who underwent radiotherapy or chemotherapy before surgery (n = 31); those with infection or serious diseases affecting the liver, kidney, or circulatory system (n = 16); patients with other malignancies or previous history of malignancies (n = 11); and those with poor compliance, who did not actively cooperate with treatment (n = 3), were excluded from the analysis. Ultimately, this study retrospectively selected 203 patients with laryngeal cancer, including 7 females and 196 males, with a mean (± standard deviation) age of 62.45 ± 9.51 years (range, 33-85 years). According to the 2017 Union for International Cancer Control/American Joint Committee on Cancer TMN classification system, there were 85 cases of stage T1, 66 of stage T2, 32 of stage T3, and 20 of stage T4. Among the 203 patients with laryngeal carcinoma, 33 were treated with transoral CO2 laser resection, 125 with open partial laryngectomy, and 45 with total laryngectomy. The Medical Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University approved this study, and all patients and their families provided informed consent.
Methods
The patient’s most recent blood test results before surgery were collected, including neutrophils, platelet, and lymphocyte counts, FIB level, NLR, and PLR. Patient prognosis was primarily assessed according to outpatient reexamination and telephone follow-up. The end of follow-up was September 2019.
Statistical Analysis
Data analysis was performed using SPSS version 22.0 (IBM Corporation, Armonk, New York). The count data are expressed as ratio, and comparisons were performed using the χ2 test or Fisher exact probability method. Determination of optimal cutoff values was performed using receiver operating characteristic (ROC) curve analysis. Differences between groups were compared using Kaplan-Meier survival analysis. Univariate and multivariate Cox regression were used to determine independent risk factors; differences with P < .05 were considered to be statistically significant.
Results
Optimal Cutoff Values for FIB, NLR, and PLR
Death was considered as the end point; the results of ROC curve analysis for FIB, NLR, and PLR are shown in Figure 1. The areas under the ROC curve for FIB, NLR, and PLR were 0.663 (95% confidence interval [CI]: 0.587-0.739; P < .05), 0.620 (95% CI: 0.541-0.699; P < .05), and 0.585 (95% CI: 0.505-0.664; P < .05), respectively. The maximum value of the Youden index (sensitivity + specificity − 1) was considered to be the optimal cutoff value. The optimal cutoff values, based on the ROC curve, were 3.05 g/L (FIB), 2.41 (NLR), and 110.94 (PLR), and the corresponding sensitivities and specificities were 82.7% and 44.3% (FIB), 53.1% and 71.3% (NLR), and 60.5% and 54.1% (PLR). Patients with laryngeal cancer were divided into the following groups: high FIB (>3.05 g/L) and low FIB (≤3.05 g/L); high NLR (>2.41) and low NLR (≤2.41); and high PLR (>110.94) and low PLR (≤110.94).
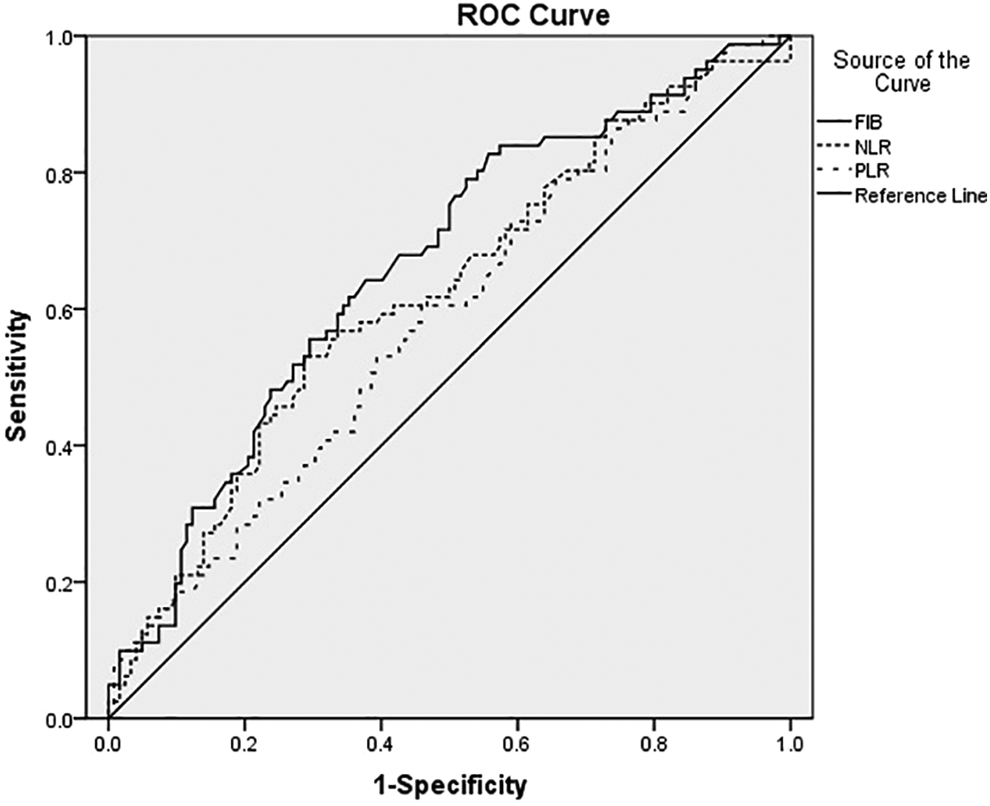
The results of receiver operating characteristic (ROC) curve of FIB, NLR, PLR. FIB indicates fibrinogen; NLR, neutrophil–lymphocyte ratio; PLR, platelet-to-lymphocyte ratio.
Relationship Between FIB, NLR, PLR, and Prognostic Factors of Laryngeal Cancer
Levels of FIB, NLR, and PLR before surgery were not related to age, sex, or smoking history but were associated with lymph node metastasis, differentiation grade, T classification, primary location, adjuvant therapy, and clinical stage (P < .05; Table 1).
Relationship Between FIB, NLR, PLR, and Prognostic Factors of Laryngeal Cancer.
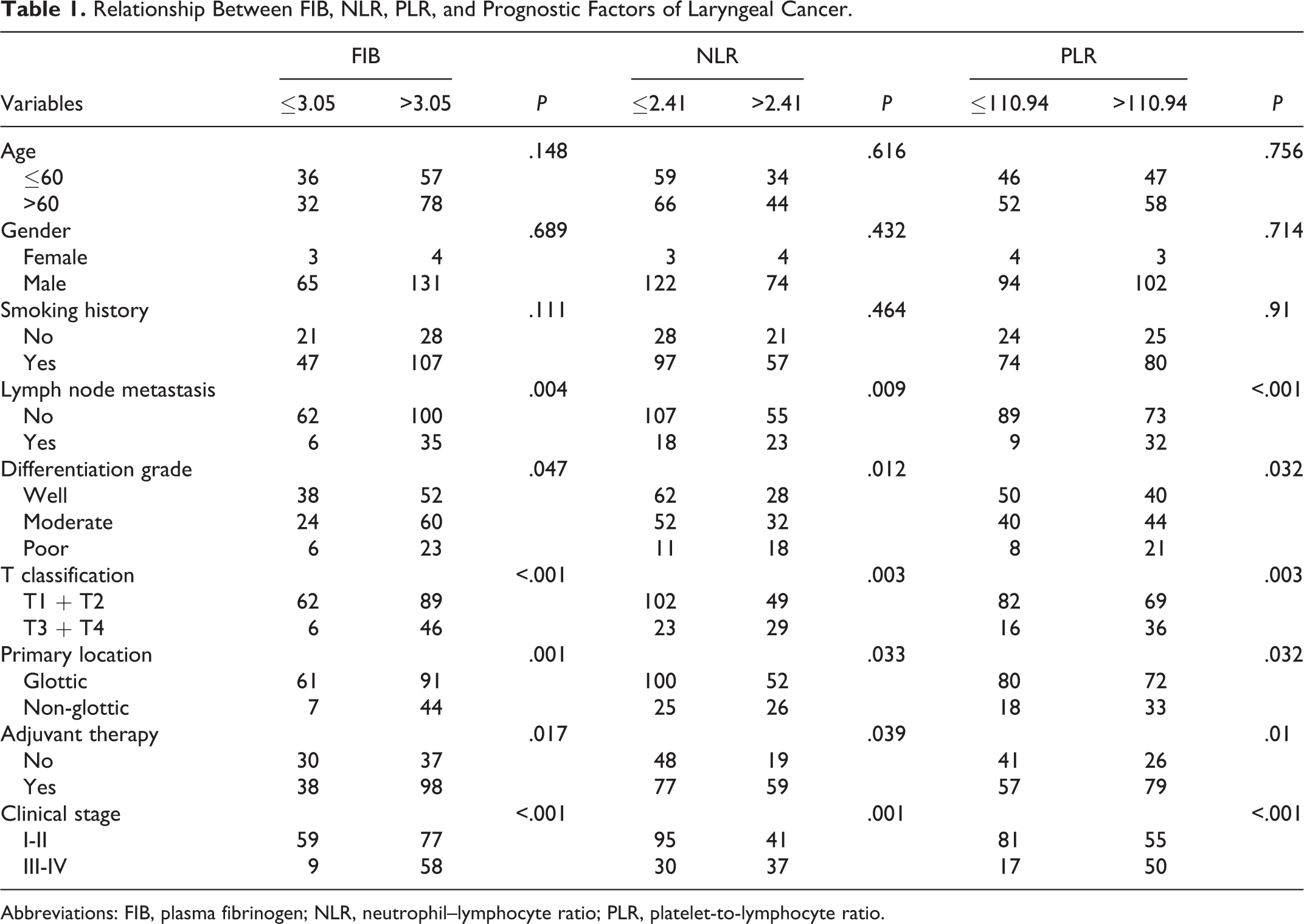
Abbreviations: FIB, plasma fibrinogen; NLR, neutrophil–lymphocyte ratio; PLR, platelet-to-lymphocyte ratio.
Risk Factors for LSCC Prognosis
Among 203 patients with laryngeal cancer, 81 died, 84 relapsed, and 14 (6.90%) were lost to follow-up. The cumulative 3-year overall survival (OS) and disease-free survival (DFS) were 76.2% and 62.9%, and the 5-year OS and DFS were 66.2% and 52.9%, respectively. Univariate analysis revealed that FIB, NLR, PLR, lymph node metastasis, differentiation grade, T classification, primary location, and clinical stage were significant factors affecting OS (P < .05). FIB, NLR, lymph node metastasis, differentiation grade, T classification, primary location, adjuvant therapy, and clinical stage were significant factors affecting DFS (P < .05) as shown in Table 2. Factors that significantly affected OS and DFS in single factor analysis were included in the Cox proportional risk model for multivariate factor analysis, which revealed that FIB, NLR, lymph node metastasis, and T classification were independent factors (P < .05) that affected OS after surgery. FIB, lymph node metastasis, and differentiation grade were independent factors (P < .05) that affected DFS after surgery (Table 3). In the low FIB (ie, ≤ 3.05 g/L) group, the 5-year cumulative OS rate was 81.6%, while in the high FIB (ie, > 3.05 g/L) group, the 5-year cumulative OS rate was 58.5% (Figure 2). Correspondingly, the 5-year cumulative DFS rates were 66.8% in the low FIB group and 45.8% in the high FIB group (Figure 3). Patients with FIB levels > 3.05 g/L had significantly shorter OS and DFS than those with FIB levels ≤ 3.05 g/L.
Prognostic Factors for DFS and OS According to Univariate Analysis.
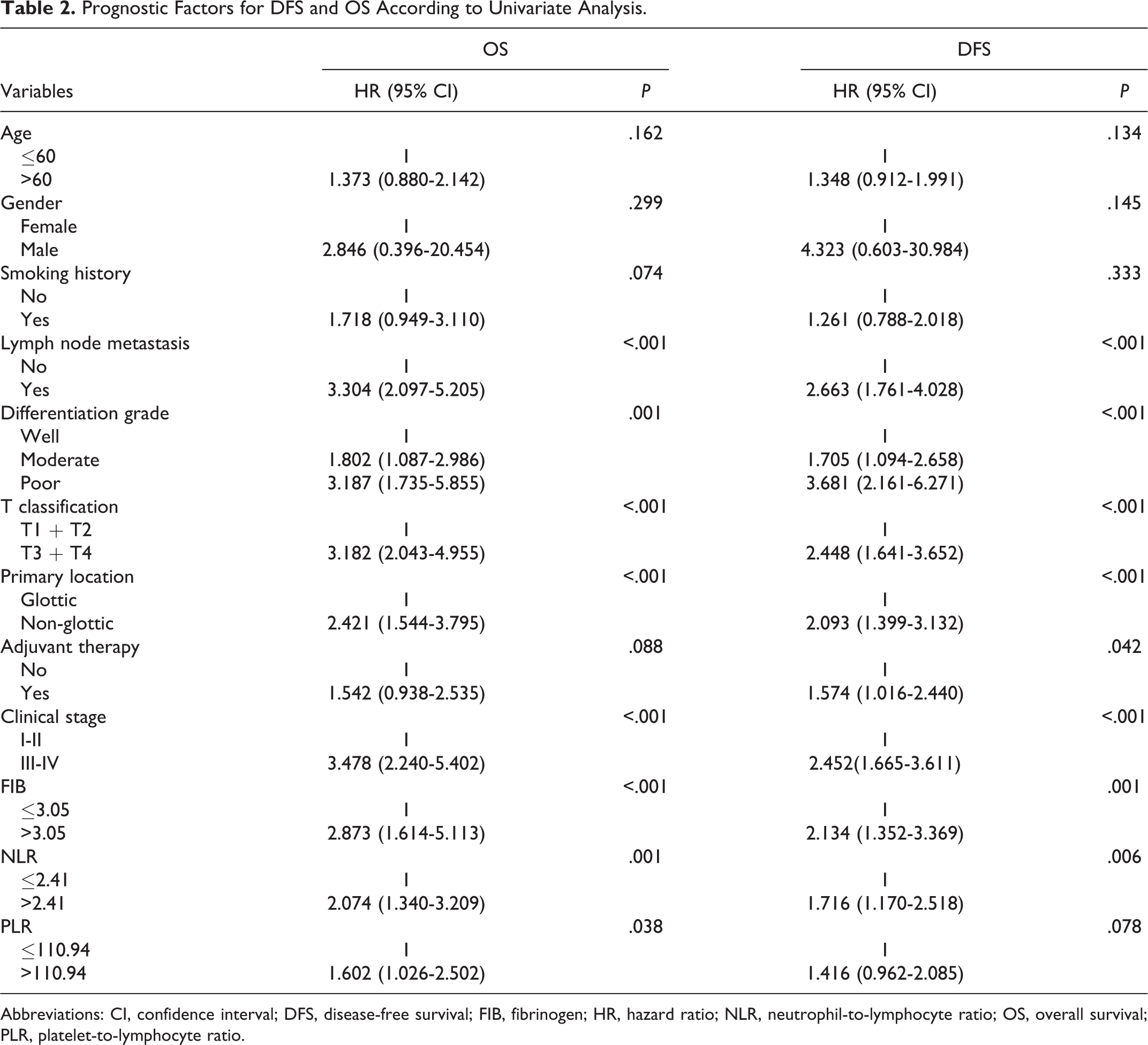
Abbreviations: CI, confidence interval; DFS, disease-free survival; FIB, fibrinogen; HR, hazard ratio; NLR, neutrophil-to-lymphocyte ratio; OS, overall survival; PLR, platelet-to-lymphocyte ratio.
Prognostic Factors for DFS and OS According to Multivariate Analysis
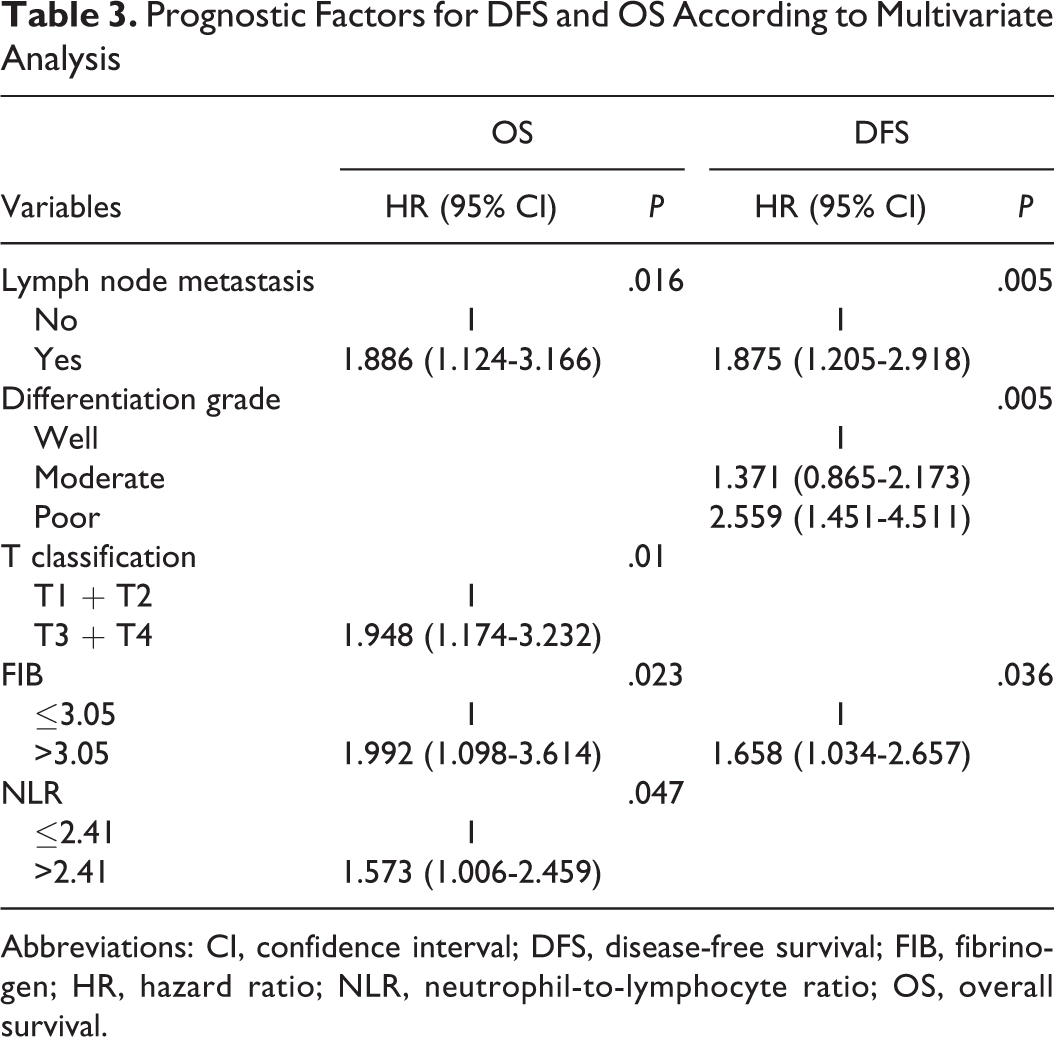
Abbreviations: CI, confidence interval; DFS, disease-free survival; FIB, fibrinogen; HR, hazard ratio; NLR, neutrophil-to-lymphocyte ratio; OS, overall survival.
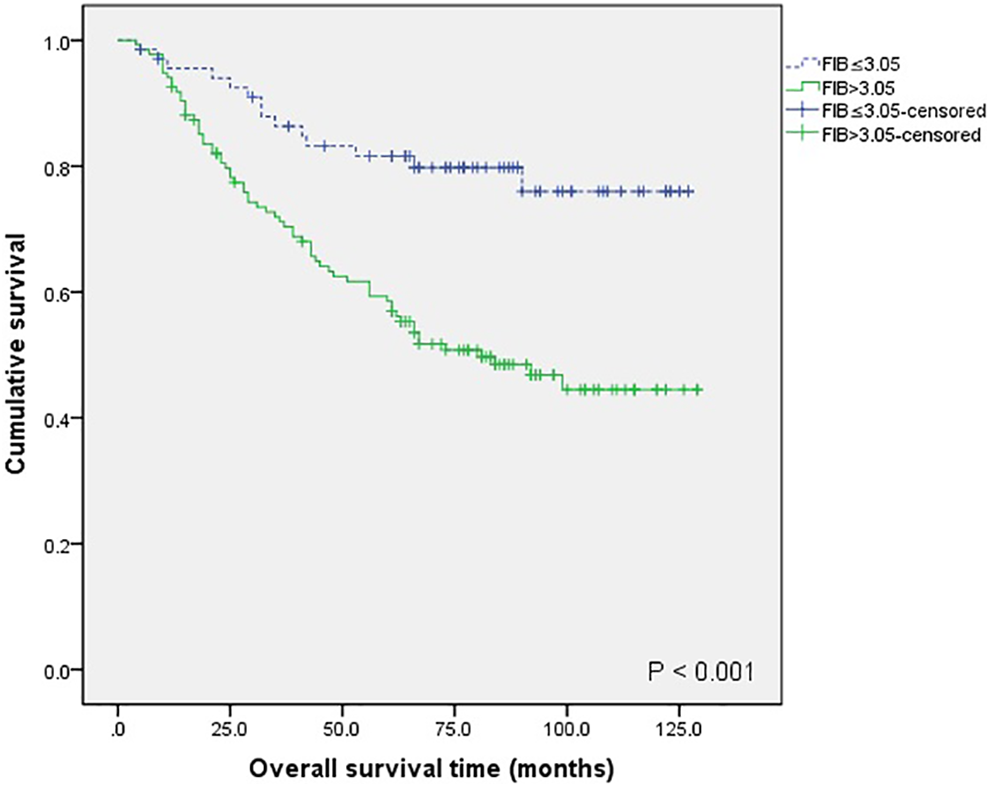
Kaplan-Meier curves for overall survival (OS) between patients with fibrinogen (FIB) > 3.05 and FIB ≤ 3.05.
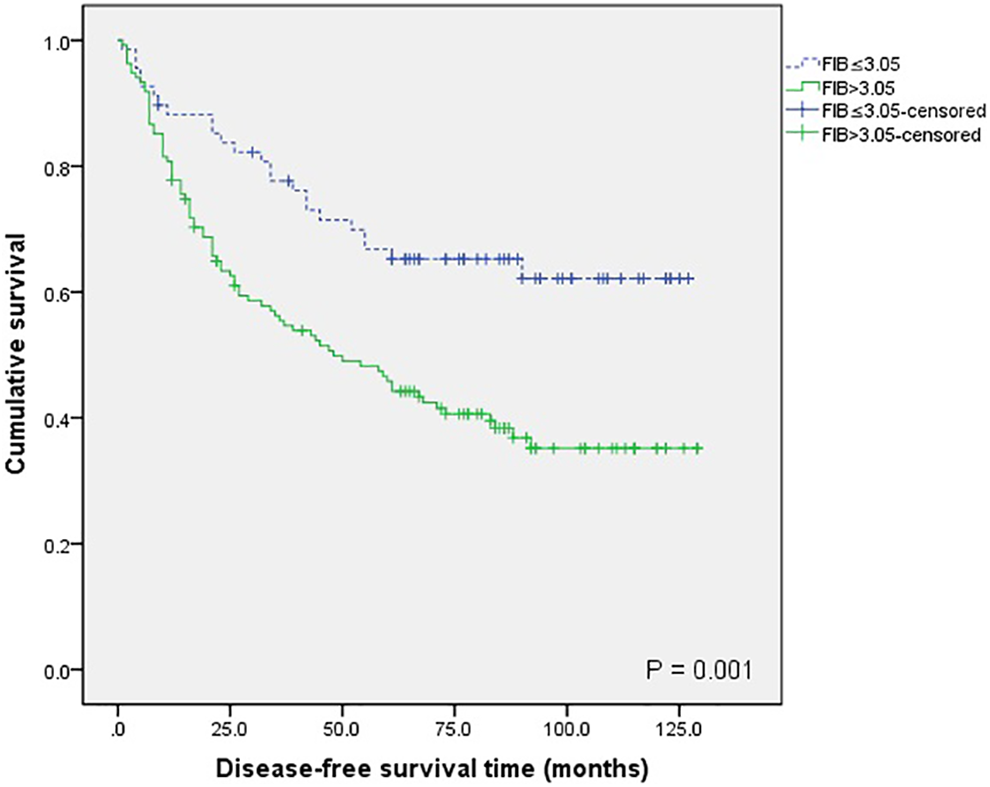
Kaplan-Meier curves for disease-free survival (DFS) between patients with fibrinogen (FIB) > 3.05 and FIB ≤ 3.05.
Discussion
It is currently believed that the occurrence and development of LSCC is the result of a combination of various carcinogenic factors, including long-term smoking or alcohol history, human papilloma virus infection, laryngeal reflux, sex hormone metabolism disorder, and/or genetic susceptibility. An increasing number of investigators are beginning to focus on potential biomarkers, such as genetic, immunological, and hematological markers in peripheral venous blood, to predict tumor metastasis, recurrence, and prognosis.11-14 Results of the present study demonstrated that preoperative hyperfibrinemia, NLR, T classification, and lymph node metastasis were independent factors affecting OS, while preoperative hyperfibrinemia, lymph node metastasis, and differentiation grade were independent factors affecting DFS in patients with LSCC. Preoperative FIB and NLR have important clinical significance because they are economical and simple tests for predicting survival in patients with laryngeal carcinoma.
Fibrinogen is an important protein synthesized by the human liver and is one of several vital components involved in the process of coagulation and thrombosis. Fibrinogen is also a pro-inflammatory protein that participates in the formation of extracellular matrix and can be endogenously synthesized by cancer cells. 15 Multiple studies have shown that FIB can promote tumor proliferation, invasion, and migration by stimulating tumor angiogenesis, regulating the growth of cancer cells and inhibiting natural killer cell functions.16-18 A meta-analysis revealed that high levels of FIB before treatment were significantly associated with decreased survival in patients with multiple solid tumors. 19 There have been few studies investigating the relationship between preoperative FIB levels and prognosis of LSCC. In the present study, we determined that the best cutoff value for FIB was 3.05 g/L, according to ROC curve analysis. Compared to plasma FIB ≤ 3.05 g/L, OS and DFS in patients with hyperfibrinemia were significantly reduced (P < .05). As such, it may be feasible to use FIB levels to evaluate and predict postoperative survival in patients with laryngeal cancer.
Studies have shown that the human inflammatory response can affect all aspects of tumor occurrence and development and not only depend on the biological characteristics of the tumor. 20 Neutrophils produce a variety of inflammatory mediators, affect tumor angiogenesis, attenuate T lymphocyte function, and promote tumor cell proliferation and metastasis.21-23 Lymphocytes alter the microenvironment of the tumor by releasing a variety of factors, inhibiting antitumor immunity, and promoting tumor growth and metastasis.24-25 Many studies have shown that NLR is associated with survival in patients with multiple cancers, including gastric, lung, colorectal, nasopharyngeal, and esophageal cancers.26-30 Mascarella et al reported that increases in NLR portended worse OS in patients with head and neck carcinoma. 31 In the current study, patients with an NLR ≤ 2.41 exhibited a significantly longer OS compared to those with an NLR > 2.41 (P < .05). Platelets inhibit the immune surveillance of by tumors natural killer cells through secretory transforming growth factor β, thereby promoting tumor proliferation and metastasis. 32 Regrettably, we found that PLR has no direct connection with survival in patients with laryngeal cancer.
This study had a few limitations, the first of which was its retrospective design. Although we recorded detailed data and follow-up results, prospective studies will help to better assess the prognostic factors in patients with laryngeal cancer. Therefore, our conclusions need to be verified in prospective studies with larger sample sizes. Second, an increasing number of studies have shown that inflammatory factors are related to poor prognosis. As such, the prognosis of LSCC patients can also be evaluated using lymphocyte-to-monocyte ratio and other inflammatory markers; however, only NLR and PLR were assessed in this study. In addition, some studies suggest that PLR is associated with prognosis in LSCC; however, the multivariate analysis performed in this study did not confirm this point, which may be related to different sample selection and sizes. Nevertheless, the prognostic value of PLR is still worthy of further study.
Conclusion
Patients with laryngeal cancer having hyperfibrinemia demonstrated poorer prognosis than those with lower FIB levels. A high NLR was associated with diminished OS in patients with laryngeal cancer. Further large-scale prospective studies are needed to verify our findings, and relevant basic research is anticipated to uncover clues to pathophysiological mechanisms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received financial support from the Natural Science Foundation of Zhejiang Province, China (No. LY19H130001).