
Abstract
Objectives
To describe our experience in excision of the submandibular gland (SMG) without drain insertion and with preservation of the facial artery as a day case surgery as well as evaluation of the surgical outcomes of this procedure.
Methods
Prospective case series study of 42 cases of chronic calcular submandibular sialadenitis that underwent SMG excision by the same surgical team during the period from 2017 to 2021. The initial surgical plan in all cases was to excise the SMG with preservation of the facial artery and without drain insertion.
Results
SMG excision without drain insertion was successfully achieved in 28 patients who were discharged on the same day. In the remaining 14 patients, the surgical dissection was difficult and a suction drain was inserted at the end of the surgery; consequently, they were discharged on the next day. In all cases, facial vessels were preserved, and complete gland excision was achieved. Among the 28 patients who had no drain insertion, 1 patient had a postoperative seroma and no patient had wound related complications. Among the 14 patients who had drain insertion, 2 patients had postoperative seroma and 3 patients had wound related complications in the form of obvious scar formation. There were no other significant complications in all patients.
Conclusions
Submandibular gland (SMG) excision with facial artery preservation and without drain insertion as a day case surgery could be safely done in cases of chronic calcular inflammation provided that meticulous surgical dissection and complete hemostasis were achieved.
Introduction
Surgical resection of the submandibular gland (SMG) is considered one of the most common head and neck surgical procedures. Its indications are including neoplastic and non-neoplastic conditions as chronic calcular sialadenitis and chronic drooling with failure of conservative treatment. 1 Chronic calcular sialadenitis or SMG sialolithiasis is the most common indication of SMG excision. Although endoscopic techniques of removal of salivary stones are progressively gaining popularity nowadays, there are still considerable number of cases that require surgical resection of the entire gland. 2
The traditional surgical approach for SMG resection is the lateral trans-cervical approach. Although many other surgical approaches have been created for SMG resection, lateral trans-cervical approach is still considered the standard approach for SMG excision (1). In this approach, insertion of a surgical drain for at least one night is the usual surgical practice by most of the surgeons in order to protect the surgical field and also the airway from the risk of any postoperative swelling. 3
However, drains insertion can be associated with higher risks of other complications. These complications include pain, discomfort, local wound infection, obvious scar formation, cutaneous fistula, temporary nerve paralysis, in addition to increase of the hospitalization period. 4 -6 It is well established that day case surgery in general have better outcome than inpatient surgery with overnight hospital stay. 7
According to our knowledge, there are few studies of drain-less excision of SMG 5,6,8 and all these studies described the application of a hemostatic agent in the surgical bed as an alternative to the traditional surgical drain. In this study, we assumed that in selected cases and with meticulous surgical dissection, drain-less excision of SMG can be achieved safely without application of any hemostatic agent.
Material and Method
This prospective case series study was conducted on 42 patients with chronic calcular submandibular sialadenitis who underwent SMG excision by the same surgical team during the period from 2017 to 2021. The Ethical Committee of Zagazig university hospital approved the study. All the patients had signed a written formal consent before participating in the study.
We excluded all cases with non calcular diseases of the SMG including neoplastic diseases, cases with previous neck surgery and cases with bleeding tendency.
The primary goal of the surgery was to remove the entire gland, including any sialoliths that may be present in the submandibular duct, with preservation of the integrity of all adjacent nerves. The secondary goal of the surgery was drainless surgical resection of the SMG.
Surgical Steps
After infiltration of the skin with 1% Xylocaine 1-100,000 epinephrine for hemostasis, 4 to 5 cm skin incision was done two fingers breadths below the angle of the mandible in a natural skin crease. The incision was deepened down onto the gland and then deep to platysma to rise a subcapsular flap (Figure 1) (not rise a subplatysmal flap) which will help to protect the marginal mandibular nerve which is running in the subplatysmal plane. The subcapsular plane.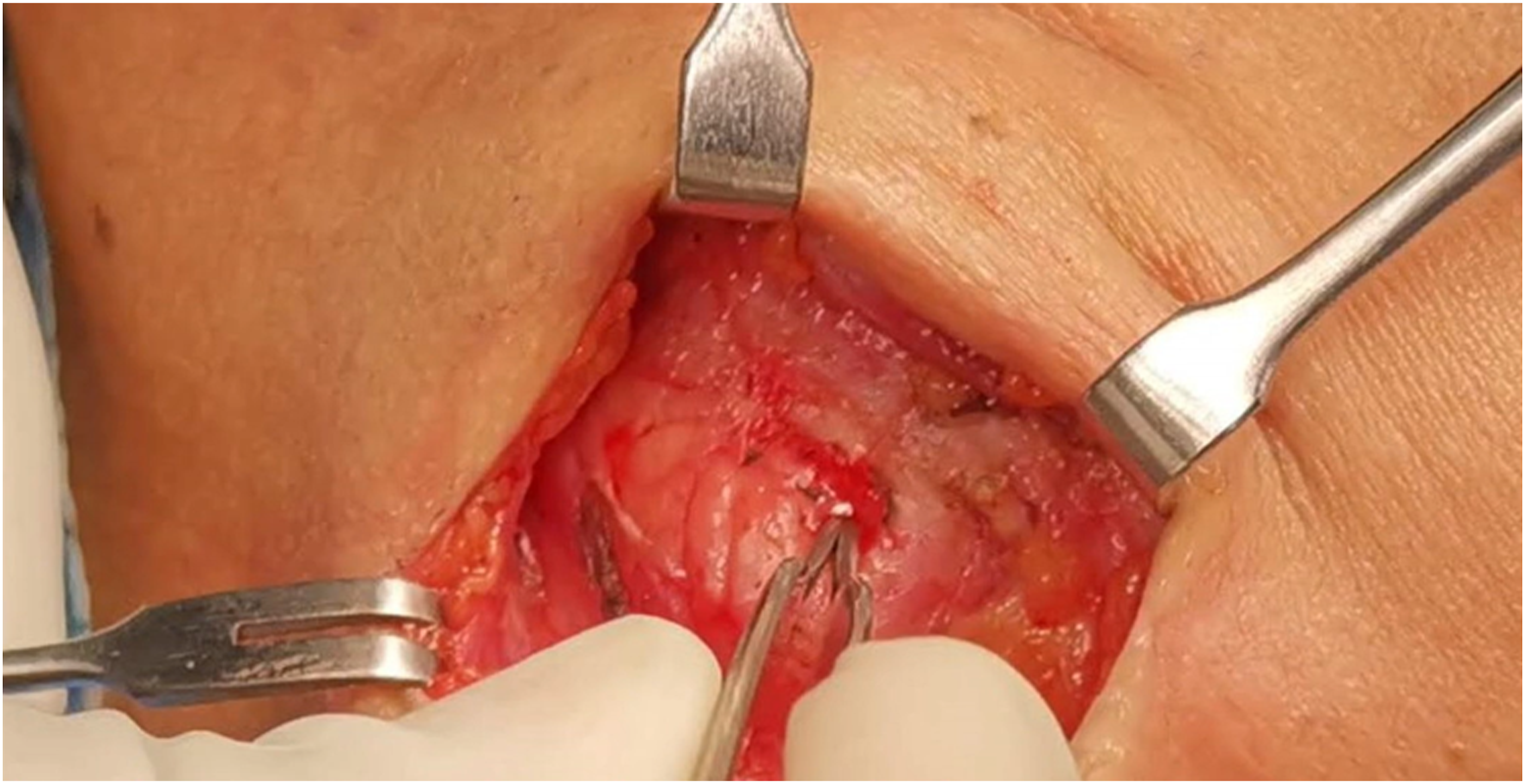
Dissection of the superficial lobe of the gland was done. We did not ligate the facial vein of facial artery, this was done by meticulous and careful dissection with only cautery or ligate the feeding vessels of the gland (Figure 2 and 3). Then dissection of the deep lode of the gland and separation of the gland from the submandibular ganglion was performed. The submandibular duct with its relation the lingual nerve was identified and the submandibular duct (Wharton’s duct duct) was ligated as far as we could. Hemostasis was insured and no drain was used. The wound was closed in two layers. The patient was discharged within 24 hours. ligation of the feeding vessels to the submandibular gland. Complete separation of the gland by only ligation and cautery of the feeding vessels without ligation of the facial vein or artery either anterior or posterior.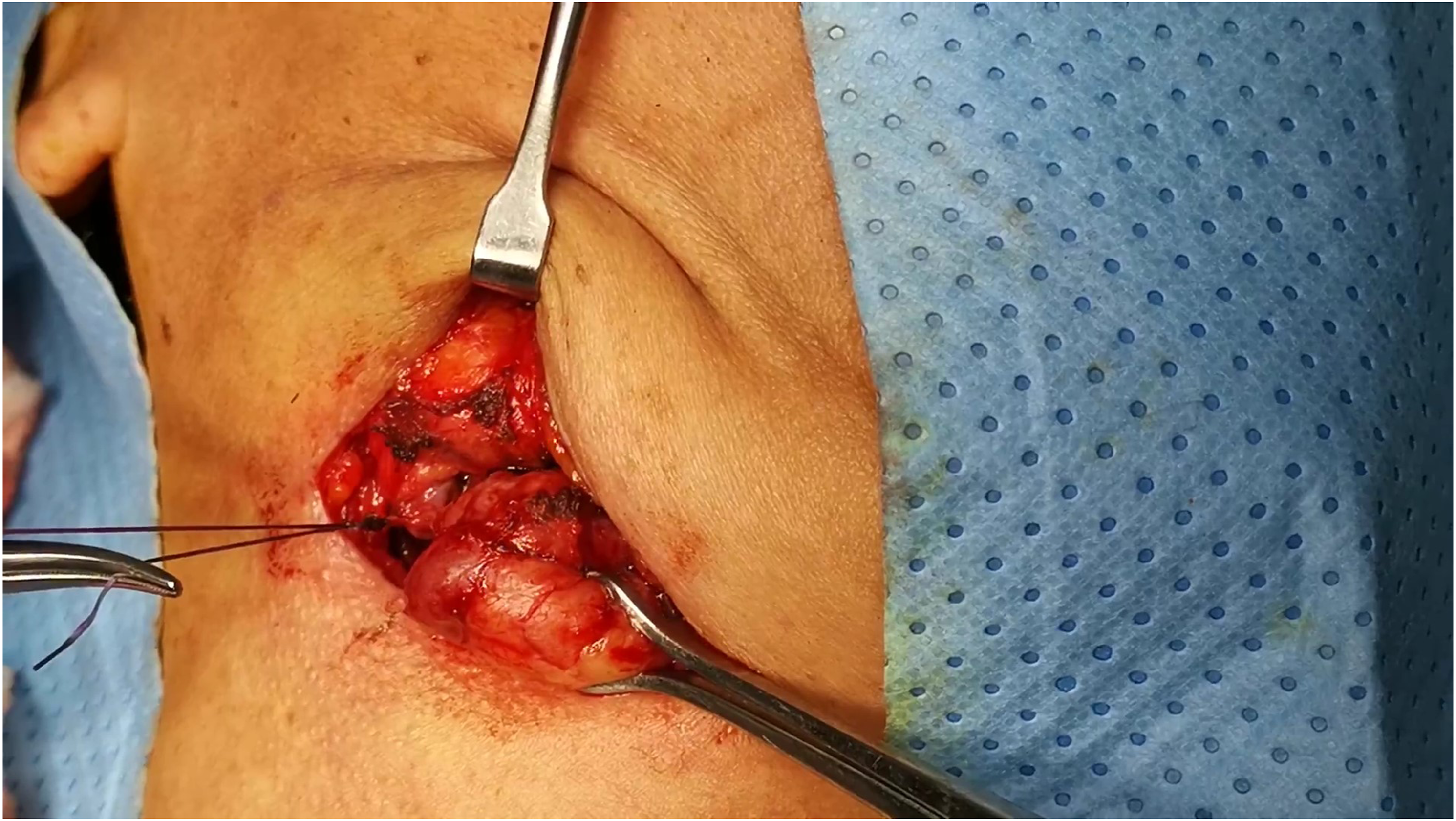
Results
Results of the Surgeries.
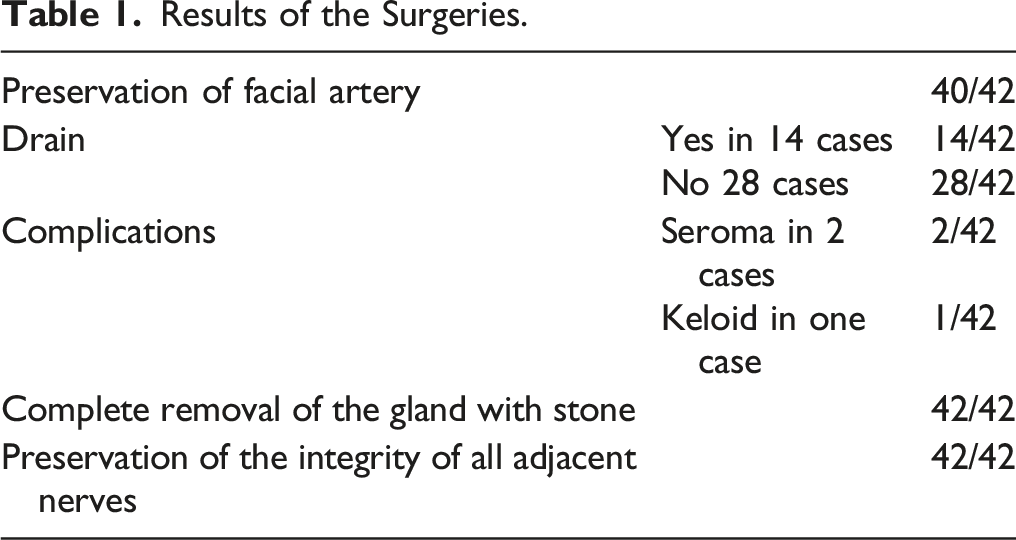
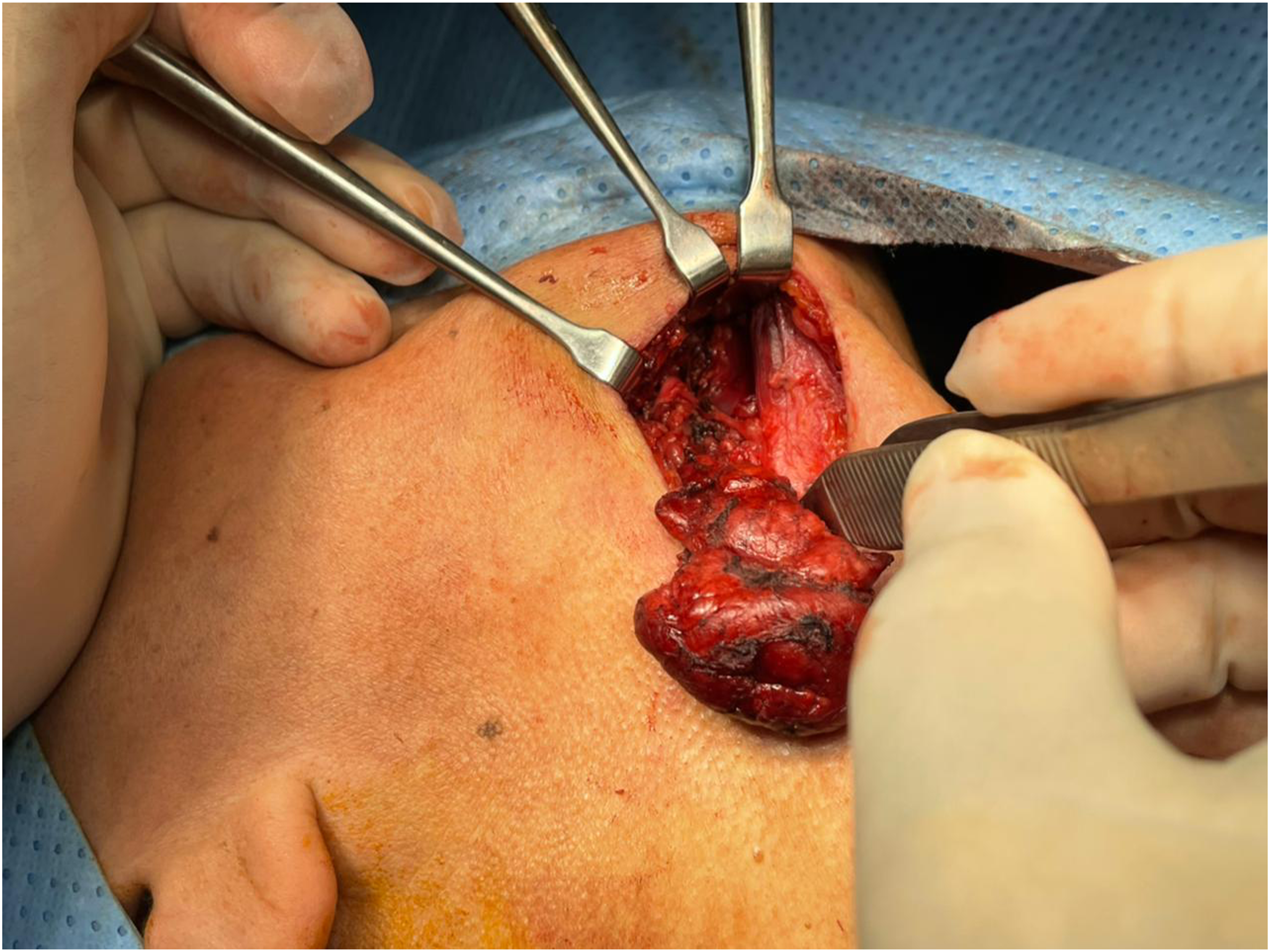
In all cases, removal of the entire gland, including any sialoliths, and preservation of the integrity of all adjacent nerves were achieved successfully (Figure 4). Facial vessels were preserved in 40 patients. The submandibular gland after complete excision.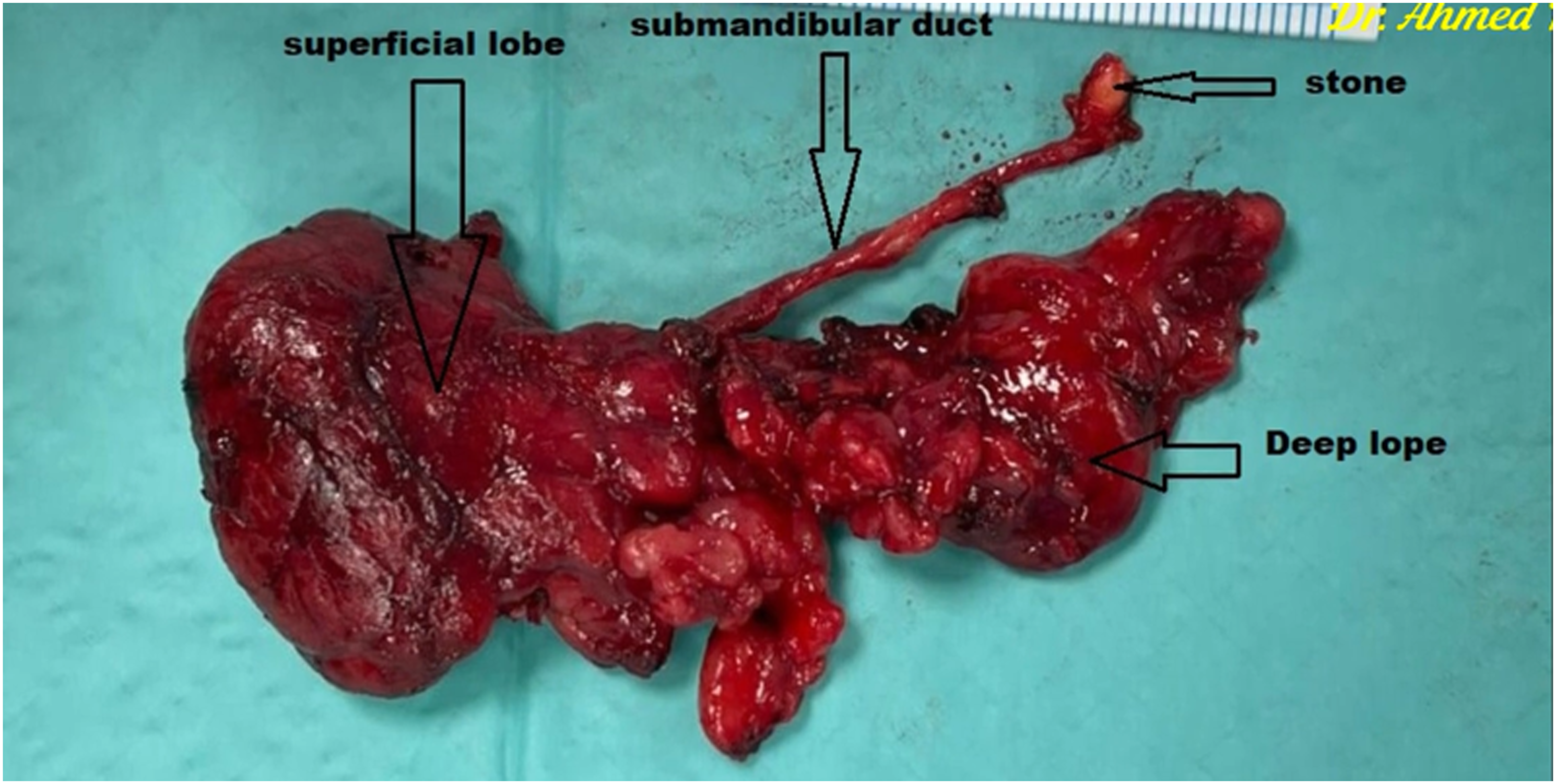
SMG excision without drain insertion was successfully achieved in 28 patients who were discharged on the same day. In the remaining 14 patients, the surgical dissection was difficult and a suction drain was inserted at the end of the surgery; consequently, they were discharged on the next day.
Among the 28 patients who had no drain insertion, one patient had a postoperative seroma and no patient had wound related complications. Among the 14 patients who had drain insertion, 2 patients had postoperative seroma and one patient developed keloid. There were no other significant complications in all patients.
During surgery, the decision of drain insertion was taken in 14 cases based on either the presence of difficulty during surgical dissection or the presence of abnormal oozing of blood while testing hemostasis at the end of surgery by valsalva maneuver. The difficulty in surgical dissection was thought to be due to either the difficulty in preservation of the facial vessels which was found embedded inside the SMG tissue (2 cases), the presence of congestion caused by acute inflammatory effect (6 cases), or the presence of abnormal unexplained oozing of the surgical field (6 cases).
Discussion
The SMG is enclosed within a sheath formed by the investing fascia of the neck that is attached superiorly to the mandible. The marginal mandibular nerve forms an important external landmark as it passes just superficial to the fascia of the SMG and deep to the plane of the platysma (review). Consequently subcapsular dissection of the SMG can protect the marginal mandibular nerve without the need for its identification.
The surgical dissection of SMG in chronic calcular sialadenitis differs from that dissection performed in case of neoplastic condition of the SMG. As in the later condition the plane of dissection should be extracapsular or subplatysmal plane which cause more difficulty in surgical dissection and consequently more expected perioperative surgical complications. Therefore, we considered chronic calcular inflammatory conditions as a one of the selection criteria for drain-less excision of SMG and we performed subcapsular dissection of the SMG without identification of the marginal mandibular nerve.
We found that surgical dissection of the submandibular duct (Wharton’s duct) can be performed safely without increasing risk of intraoperative bleeding, provided that accurate identification of the related lingual nerve was achieved. This is step is essential to allow for ligation of the Wharton's duct as distal as possible in order to avoid the recurrence of the stone.
The traditional description of the surgical steps of SMG excision considered the step of ligation of the facial artery as an essential step in the surgery. 9,10 However, later on, some literature found that facial artery can be safely preserved in all cases of SMG excision for benign diseases and in selected cases of malignancy. 11 In our study, we could preserve the facial artery in all cases except only 2 cases in which the facial artery was embedded deep in the matrix of the SMG; Consequently, ligation of the artery was performed to allow for clear surgical dissection of the SMG. Preservation of the facial artery keeps the artery for any future usage of any vascularized flap depended on the artery later in the patient life.
Laverick et al 3 performed a quantitative assessment of the amount of the drainage that occurs over the first 24 hour after surgical resection of the SMG. They documented that there is a clear reduction, or plateau, in the volume of the drained fluids over the first 6-8 h postoperatively. 3 Therefore, we were keeping the patients under observation for 8 hours to confirm that there is no expanding hematoma or airway compromise.
Previous studies on drainless SMG excision described the application of a hemostatic agent as an alternative to the insertion of a surgical drain. 5,6,8 Park HS et al 5 used hemostatic fibrin glue in 23 patients and they reported minor complications in 2 cases only. Bannister M and Ah-See K (8) used hemostatic agent Surgiflo® in 17 patients and they reported no complications in all cases. ŞAHİN B et al used hemostatic oxidized regenerated cellulose in 17 patients and they reported minor complications in 2 cases only. All of these studies included different indications for SMG excision.
In our study we performed drain-less SMG excision without application of any hemosatic material in the surgical bed. We found that in selected cases drain-less SMG excision could be done safely. Our selection criteria for drain-less SMG excision were presence of chronic inflammatory condition in the SMG as an indication for surgery, absence of acute inflammatory condition of the SMG during surgery, easy dissection in the correct, subcapsular, surgical plane, successful preservation of the main facial vessels, and secured hemostasis with absence of any oozing during performing valsalva maneuver at the end of surgery. We assumed that under these circumstances, drain-less SMG excision can be safely performed without application of any hemosatic material in the surgical bed.
Limitation of the study: We need further comparative studies to test the role of each criteria in the expected amount of drainage and hence the decision of application of surgical drain.
Conclusion
Submandibular gland (SMG) excision with preservation of the facial artery and without drain insertion as one day case surgery could be reliable and safe in cases of chronic calcular inflammation provided that meticulous surgical dissection and complete hemostasis were achieved.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Obtained.
Informed consent
Obtained from all authors.
Data Availability
Available.