
Abstract
Amyloidosis is an extracellular deposition of amyloid located in different organs or in a systemic distribution. We present a case of a 78 year-old male with hemodyalisis assosciated amyloidosisis involving the right sternoclavicular joint. Clinical and imaging implications are described.
A 78-year-old male with past medical history of hypertension and end-stage renal disease on hemodialysis 3 times per week presented at our institution for a growing right neck mass for the last 3 months. Patient reported tightness in the neck with limited movement and denied neck tenderness, cough, hemoptysis, or dysphagia. Physical examination demonstrated restricted neck movement to the left, a right sternoclavicular 5 cm, fixed, nontender mass, and a left arm arteriovenous fistula. Computed tomography of the chest revealed an expansile mass arising from the right sternoclavicular joint with significant bone fragmentation and destruction. This mass extended slightly into the anterior mediastinum abutting the right lobe of the thyroid gland, which revealed, coincidentally a different soft tissue density mass suggesting a thyroid adenoma (Figure 1). The sternoclavicular mass was subsequently biopsied demonstrating pink collagen-type extracellular material on hematoxylin–eosin staining, salmon pink deposits on Congo red staining, apple-green birefringence, and thioflavin T positivity consistent with Amyloidoma (Figure 2). Biopsy of the thyroid mass did not reveal amyloid deposits.
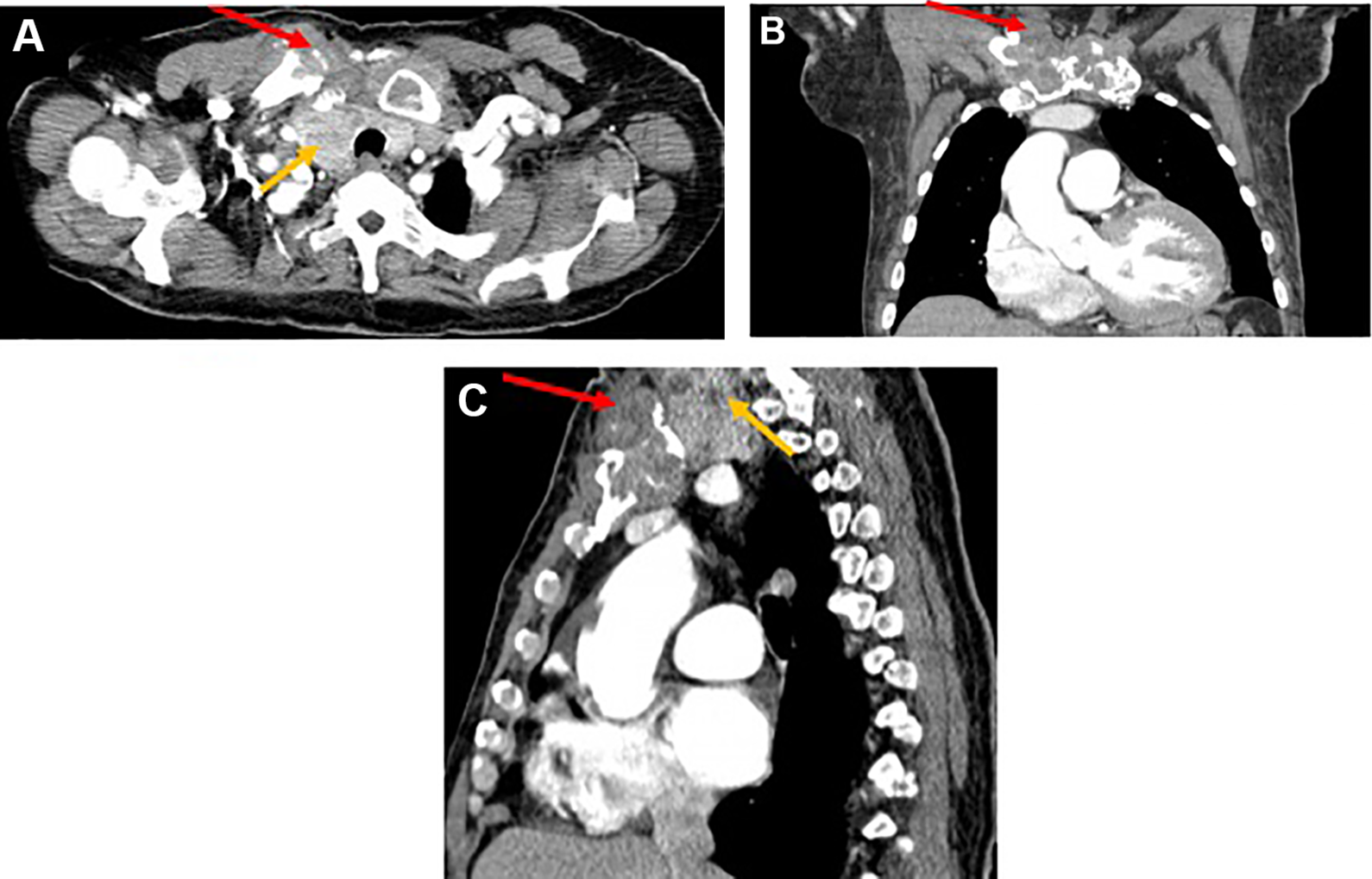
Computed tomography of the chest. A, Axial, (B) coronal, and (C) sagittal views reveal an expansile mass arising from the right sternoclavicular joint with significant bone fragmentation. This mass extends slightly into the anterior mediastinum (red arrows) abutting the right lobe of the thyroid gland which reveals, coincidentally a different soft tissue density mass suggesting a thyroid adenoma (yellow arrows). The sternoclavicular joint mass is consistent with amyloid arthropathy in the clinical setting of end-stage renal disease and hemodialysis.
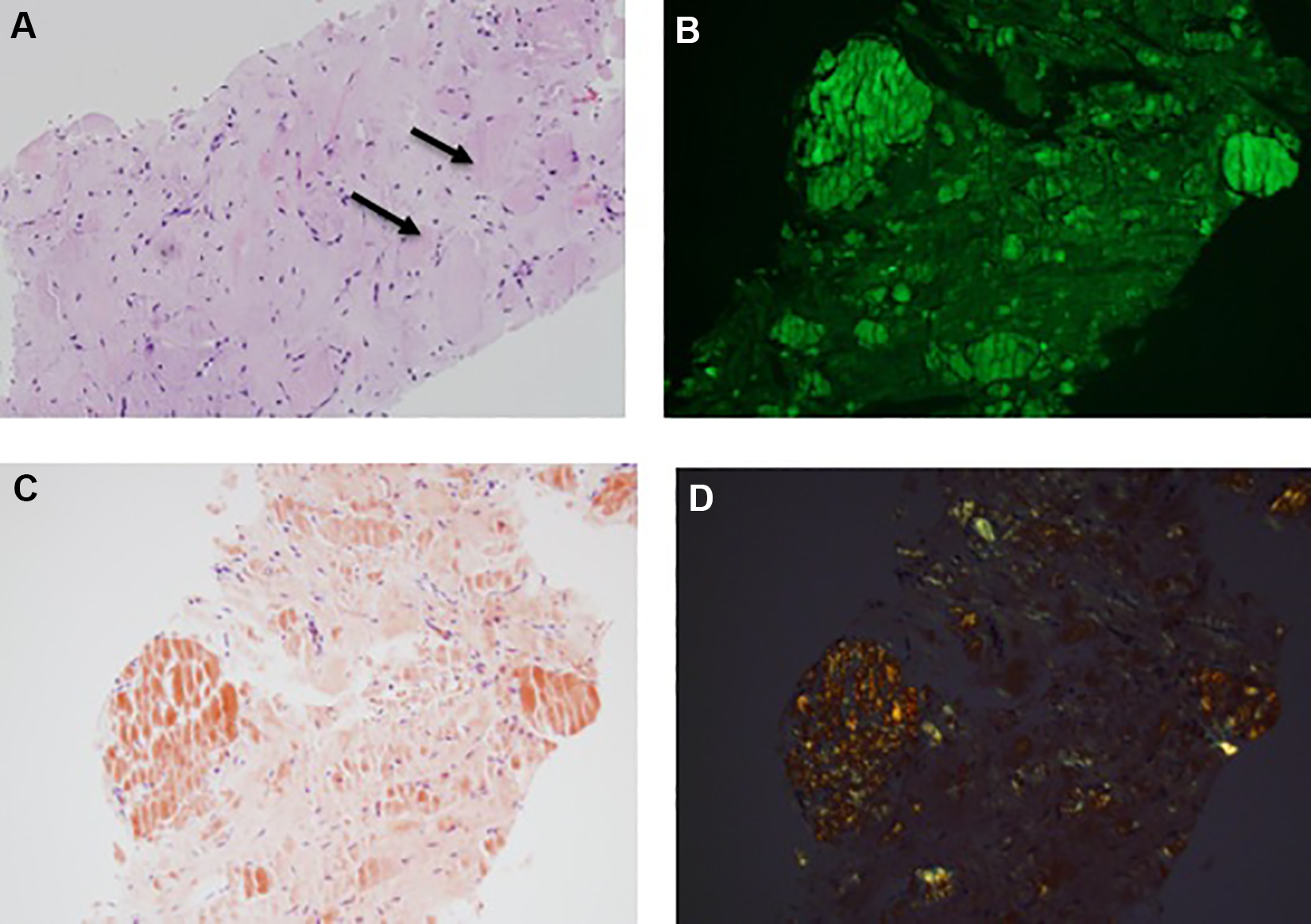
Right clavicular mass core biopsy. A, Hematoxylin and eosin staining reveals eosinophilic collagen-type extracellular material (black arrows). B, Thioflavin t positivity. C, Congo red staining demonstrates salmon pink deposits. D, Polarized light microscopy shows apple green birefringence. Findings are consistent with amyloidoma.
Amyloidosis is defined as extracellular deposition of amyloid protein located in a specific organ or in a systemic distribution. 1 Based on the fibril protein of the amyloid deposit, the Nomenclature Committee of the International Society of Amyloidosis classifies this entity in primary, secondary, and hemodialysis-associated amyloidosis. Primary amyloidosis is characterized by monoclonal immunoglobulin light chains; secondary amyloidosis is caused by the accumulation of the acute phase protein serum amyloid A and an increase in β-2 microglobulin is often seen with hemodialysis associated amyloidosis due to the inability of the urinary system to excrete the aforementioned molecule. 1 -4
Amyloid arthropathy is caused by the accumulation of amyloid in either the axial skeleton affecting the skull, hyoid bone, rib cage, and vertebral column or the appendicular skeleton affecting the shoulder and pelvic girdle and upper and lower extremities. 5 Amyloid arthropathy also affects the osteoarticular system resulting in erosive osteoarthropathies and destructive spondyloarthropathies. Clinical presentation depends on the location of the affected joints. 4 Signs and symptoms include carpal tunnel syndrome, compression radiculopathy, and pathological fractures. 4,5 Imaging modalities to diagnose this condition include radiographs, ultrasound, computed tomography, and magnetic resonance. 1 -6 Amyloid bone lesions on radiographs demonstrate different size radiolucencies within the cortical or medullary bone with juxta-articular soft tissue swelling and subchondral cysts; ultrasound reveals echogenic amyloid tissue within the affected joint and thickening of the involved tendon plus accumulation of fluid within the bursae; computed tomography shows areas of osteolysis in cortical bone, osseous erosion, and periarticular soft tissue density mass; magnetic resonance demonstrates amyloid infiltration as an abnormal soft tissue deposition with low signal intensity on T1 and low to intermediate signal intensity on T2 located periarticularly or within the involved joint. 1 -6
Histopathology findings of this condition include infiltrate with collagen-type extracellular material that stains pink on hematoxylin–eosin staining; salmon pink deposits on Congo red histochemical staining, apple-green birefringence on polarized light microscopy, and thioflavin T positivity for amyloid fibrils. 1,3,7 To our knowledge, this is the first report in English literature highlighting sternoclavicular amyloid arthropathy findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.