
Abstract
Introduction
Incidents involving esophageal foreign bodies represent common emergencies in clinical practice, arising from diverse factors including accidental ingestion, mental health conditions, intellectual disabilities, and substance abuse. Historically, adults have commonly encountered complications from the ingestion of chicken and duck bones, 1 as well as fish bones. However, the increasing consumption of jujubes, either as a food ingredient or when consumed whole, is contributing to a rise in incidents of esophageal jujube pit impaction in clinical settings. The jujube, scientifically known as Ziziphus jujuba, is a deciduous tree that belongs to the buckthorn family (Rhamnaceae). Native to the Middle East and South Asia, the jujube tree has been cultivated in various regions, including China. The tree bears small, oval-shaped fruit, commonly referred to as jujubes or red dates (refer to Figure 1). Inside the fruit, there is a single pit. With its 2 sharp edges (refer to Figure 1), the pit can penetrate the walls of the digestive tract. 2 Jujube pit impaction can result in complications such as bleeding, perforation, and infections, and in rare cases, it can be fatal. 3 A timely and accurate diagnosis of the impaction site and its relationship to adjacent structures is crucial for effective treatment. Managing esophageal foreign bodies often requires a multidisciplinary approach, involving otolaryngology, gastroenterology, and emergency departments. Treatment approaches vary depending on the patient’s age and the nature of the foreign body.4,5 In recent years, there has been an increasing application of artificial intelligence technology in diagnosing and identifying esophageal foreign bodies. 6 Computerized tomography (CT) is acknowledged as a sensitive tool for detecting small or faintly opaque objects like jujube pits, toothpicks, fish bones, acrylics, and plastics. 7 In this study, we collected data from 40 patients with esophageal jujube pit impaction, analyzed the multi-slice computed tomography (MSCT) imaging presentations, and compared them with findings from endoscopy or surgery. The objective is to enhance the diagnostic accuracy for esophageal jujube pit impaction and provide valuable references for clinical treatment.
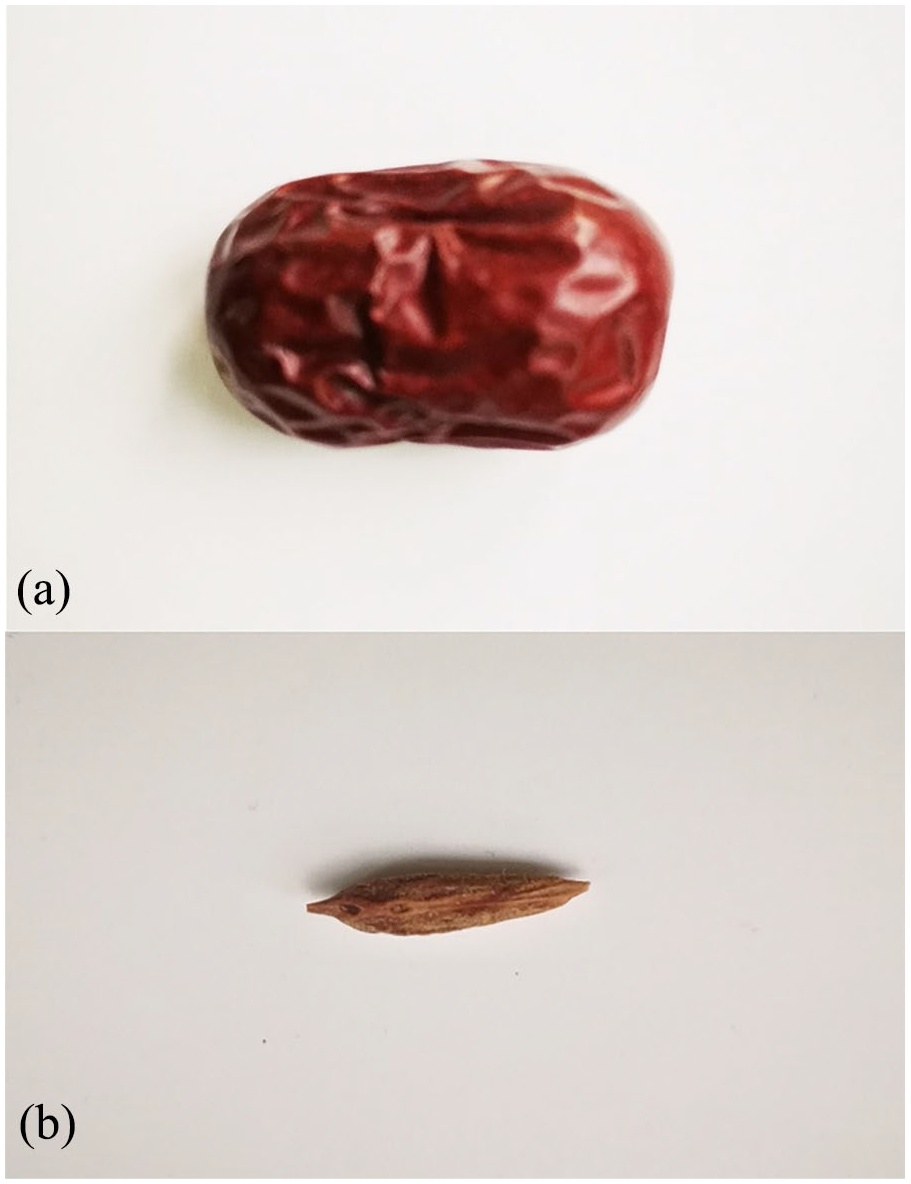
(a and b) Pictures of jujube fruit and its pit, respectively.
Material and Methods
General Information
We collected data from 40 patients who were diagnosed with esophageal jujube pit impaction utilizing MSCT during the period spanning December 2018 to November 2019. The cohort consisted of 23 males and 17 females, ranging in age from 38 to 77 years, with a median age of 69 years. The onset of symptoms varied from 2 hours to 4 days, all occurring after the inadvertent swallowing of jujube pits. Symptoms manifested as throat discomfort and sternum pain, with some patients reporting swallowing obstruction. Among these cases, 35 underwent endoscopic removal, while 5 received surgical intervention, involving collaborative management by thoracic surgery and gastroenterology departments.
Examination Method
Siemens Definition multi-slice spiral CT (Somaris/7 syngo CT VA48A; SOMATAOM Definition Flash) examinations were performed with patients positioned in a supine orientation. The scanning encompassed the region from the upper margin of the cervical 6 vertebrae to the lower margin of the costal arch. The scanning parameters included 120 kV, adaptive tube current, a pitch of 1.5, a standard layer thickness of 5 mm, an interlayer spacing of 5 mm, reconstruction layer thickness, interlayer spacing of 1 mm, and multi-planar reformation (MPR) of the reconstructed data. The cases were organized and subjected to statistical analysis based on age segments and impaction sites. Furthermore, the angle between the long axis of the impacted jujube pit and the esophageal longitudinal axis (0-30°, 30-60°, 60-90°) was classified and compared with intraoperative findings.
Statistical Analysis
All data were analyzed using SPSS (Version 24.0). The frequency of the onset time, CT manifestations, and incarceration type were presented as n (%). The relationship between onset time, CT manifestations, and incarceration type were analyzed with Pearson correlation analysis. A significant level of P < .05 was considered statistically significant.
Results
Esophageal Jujube Pit Impaction Age Distribution
The distribution of ages was as follows: 3 patients were in the age range of 38 to 47 years, 7 patients in the range of 48 to 57 years, 12 patients in the range of 58 to 67 years, and 18 patients in the range of 68 to 77 years. Notably, 75% of the cases occurred in individuals aged 58 years and above.
Esophageal Jujube Pit Impaction Site and CT Characteristics
Out of the instances of impaction, 32 were located in the cervical esophagus, precisely at the entrance, 4 in the upper thoracic esophagus, 3 in the midthoracic segment, and 1 in the lower thoracic segment. Impactions at the esophageal entrance constituted 80% of the overall cases. The axial position revealed circular or oval high-density shadows, and MPR distinctly illustrated the spindle shape of the jujube pit, exhibiting varying degrees of low density at the center.
Positional Relationship Between Jujube Pit and Esophageal Wall and Complications
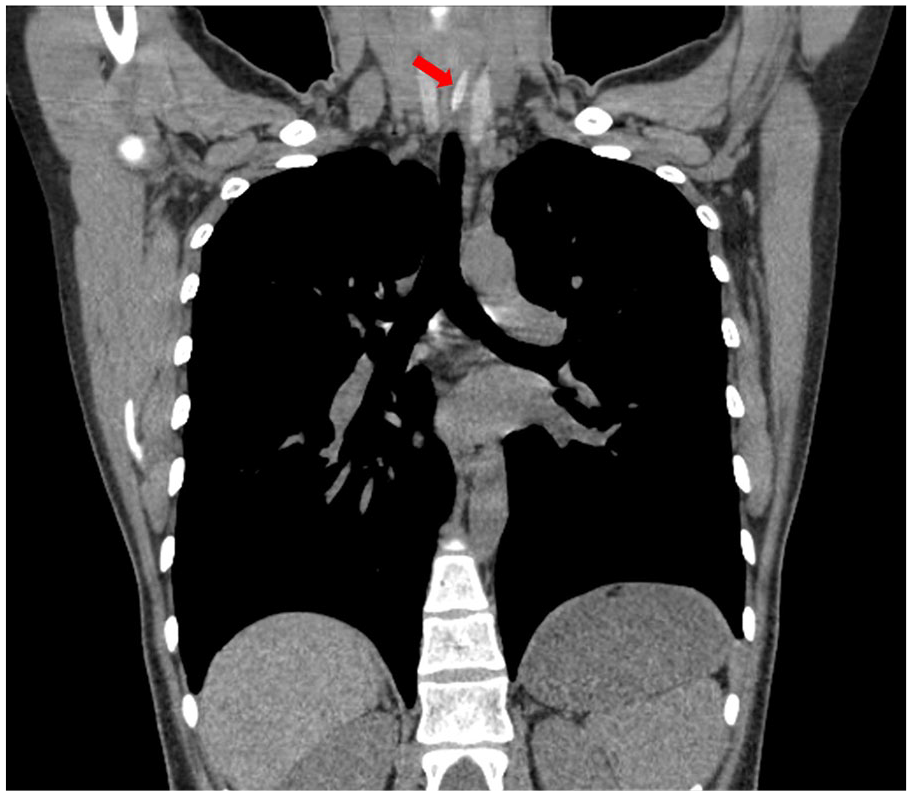
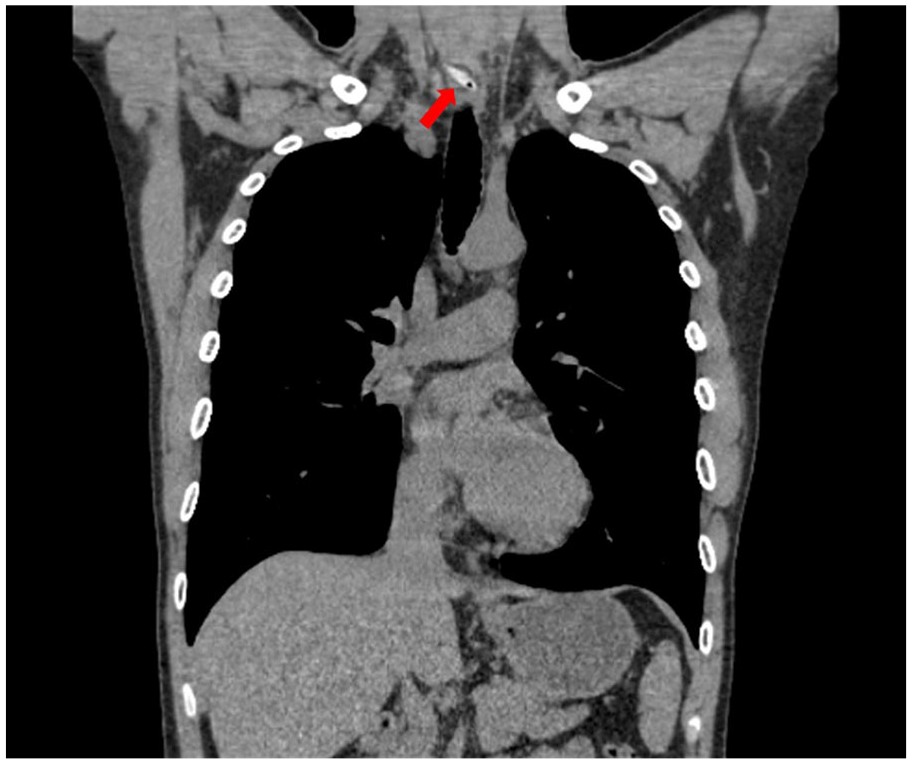
All instances of jujube pit impaction exhibited a lateral orientation. Among these, 2 cases featured an angle less than 30° between the long axis of the jujube pit and the esophageal longitudinal axis, classifying them as longitudinal impaction (refer to Figure 2). In addition, there were 16 cases of oblique impaction, characterized by angles ranging from 30° to 60° (refer to Figure 3), and 22 cases of transverse impaction, with angles falling within the range of 60° to 90° (refer to Figure 4). Out of the total 40 cases, 28 demonstrated only slight thickening of the esophageal wall at the impaction site, while 9 displayed increased periesophageal fat density, and 3 exhibited small air bubbles around the esophagus, indicative of perforation. In the 9 cases with increased fat density and the 3 with air bubbles, the long axis of the impacted jujube pit was at an angle of 60° to 90° to the esophageal longitudinal axis. One case highlighted the impaction site near the aorta (refer to Figure 5), prompting the choice of a safer thoracoscopic extraction combined with endoscopy instead of direct endoscopic removal. In another case, heightened chest pain post-endoscopic removal necessitated a follow-up CT scan, revealing the presence of mediastinal emphysema (refer to Figure 6). We found that the transverse impaction of the jujube pit may pose the highest risk of complications, followed by the oblique and longitudinal impaction.
Solid high-density jujube pit at the esophageal entrance, showing longitudinal impaction (indicated by a red arrow).
Oblique impaction of a jujube pit at the esophageal entrance (red arrow), with localized wall thickening.
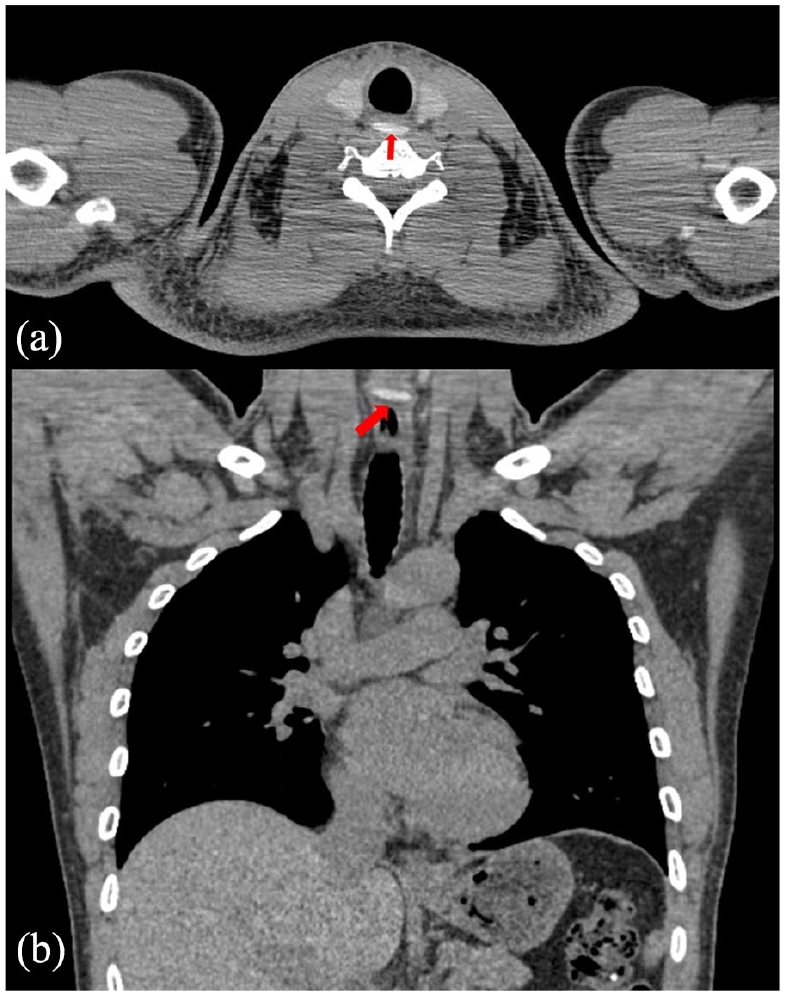
Transverse impaction of a jujube pit at the esophageal entrance (red arrow). (a) An axial image and (b) a coronal image, both showing localized thickening of the wall of the tube.
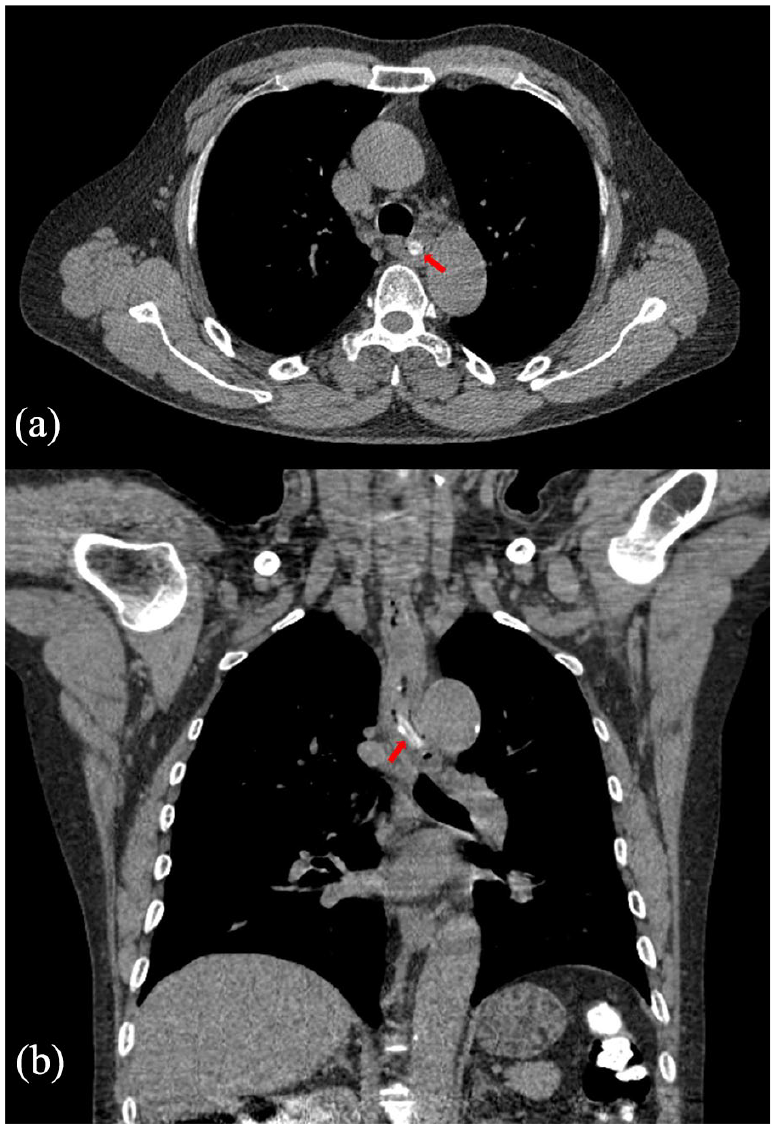
Impaction of a jujube pit in the upper thoracic esophagus (red arrow). (a) The axial view and (b) the coronal view, both displaying the jujube pit impaction site adjacent to the descending aorta.
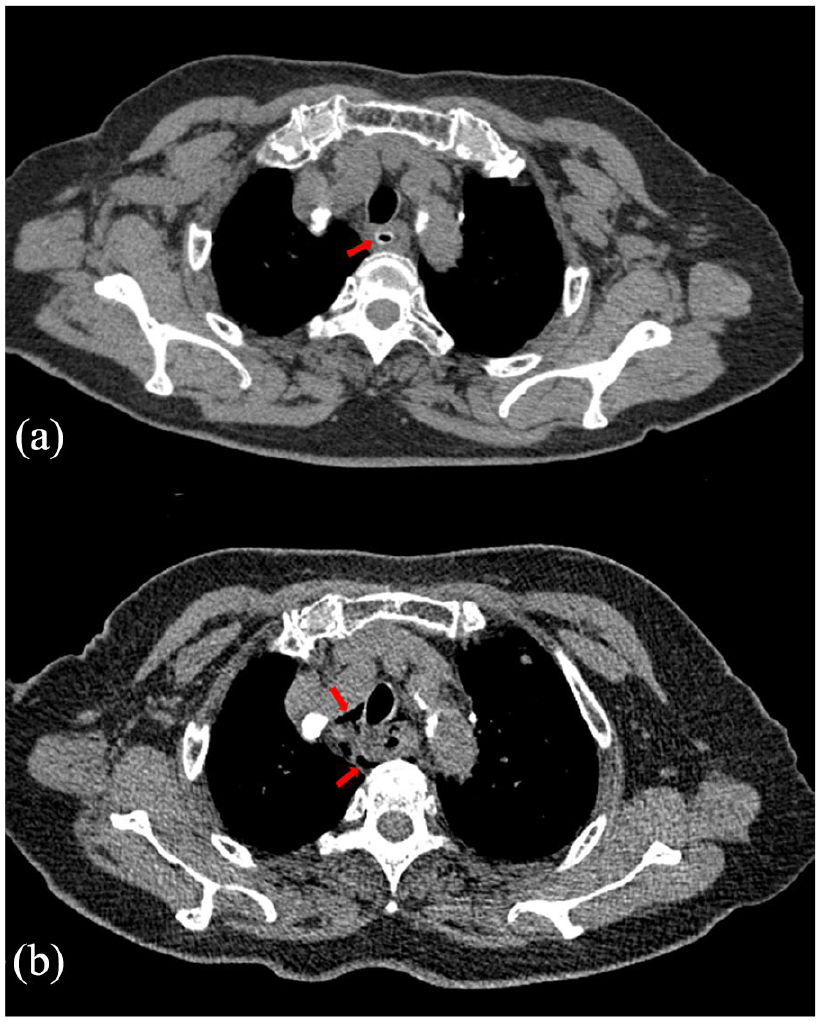
Impaction of a jujube pit in the upper thoracic esophagus. (a) The preoperative image (red arrow) with central gas density and (b) the postoperative review showing multiple gas shadows around the esophagus (red arrow).
Endoscopic and Intraoperative Findings
Endoscopic assessment revealed evident damage to the esophageal mucosa in 35 instances, with esophageal perforation formation observed in 4 cases. In one of these cases, pus was additionally identified within the perforation. Following endoscopy, the 5 patients with perforation underwent surgical intervention. In the course of these procedures, it was discovered that one or both ends of the jujube pit had penetrated the esophageal wall, accompanied by varying degrees of surrounding inflammatory encapsulation.
Relationship Between the Onset Time, CT Manifestations, and Incarceration Type
The frequency and percentage of the onset time, CT manifestations, and incarceration type are shown in Table 1. Pearson correlation analysis among the 3 are shown in Table 2. The result showed that the correlation coefficient between the onset time and CT manifestations was −0.150, which was close to 0, and the P value was .357, indicating that there was no correlation between the onset time and CT manifestations. The correlation coefficient between the onset time and the incarceration type was −0.022, which was close to 0, and the P value was .891, indicating that there was no correlation between the onset time and the incarceration type.
The Frequency of the Onset Time, CT Manifestations, and Incarceration Type.
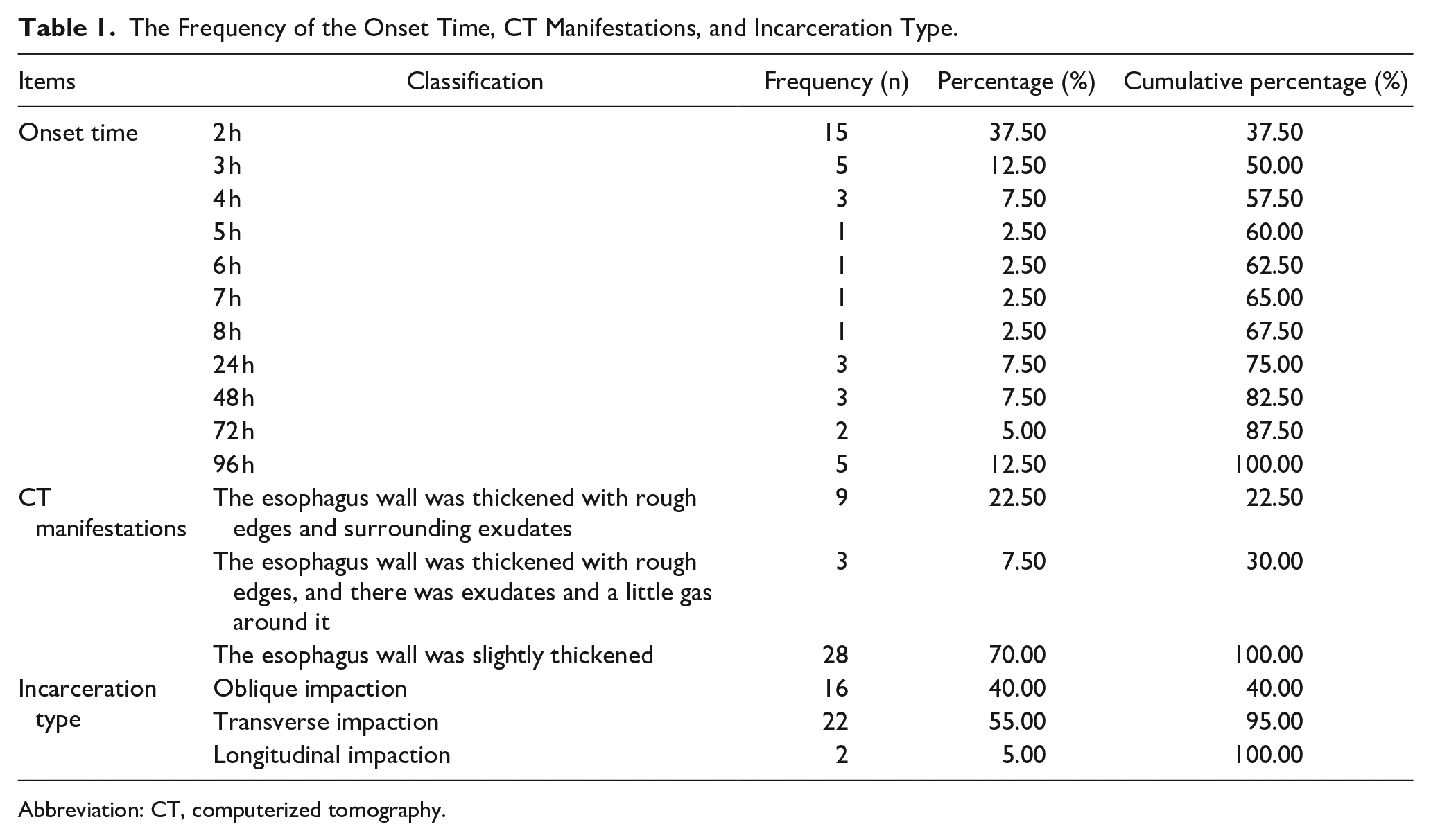
Abbreviation: CT, computerized tomography.
Pearson Correlation Analysis of Onset Time, CT Manifestations, and Incarceration Type.
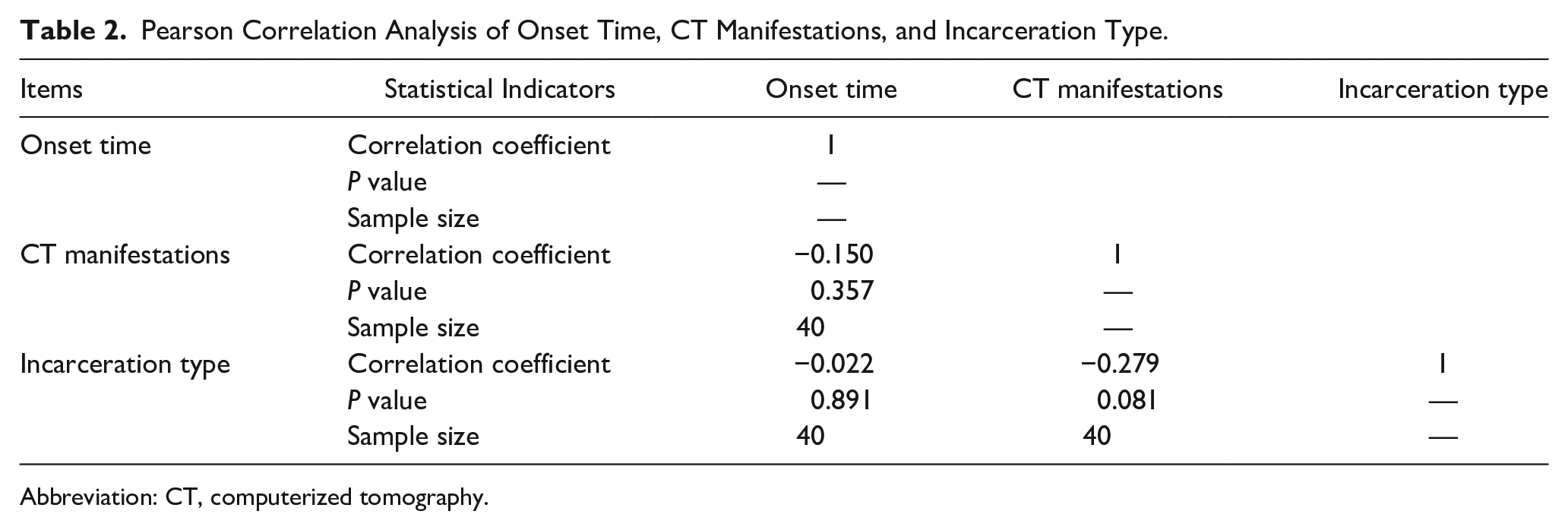
Abbreviation: CT, computerized tomography.
Discussion
Esophageal jujube pit impaction represents a distinctive form of esophageal foreign body. The slender and sharp ends of these pits elevate the potential for complications such as perforation and bleeding. Hence, precise localization of the impaction and the identification of any associated complications are vital prerequisites before clinical intervention. This crucial information informs the choice of an effective treatment approach, aiming to mitigate subsequent risks.
Traditionally, diagnostic approaches for esophageal foreign bodies have included X-ray films, barium swallow radiography, CT scans, and endoscopy. X-ray films, hindered by their limited density resolution and the challenges of 2-dimensional imaging that may overlap with neighboring structures, exhibit a diminished detection rate for foreign bodies, particularly in assessing complications. Barium swallow radiography, while being straightforward and cost-effective, is less frequently preferred due to the potential risk of contrast medium leakage in cases of esophageal perforation, which can subsequently lead to mediastinitis. Moreover, the contrast medium may adhere to both the foreign body and esophageal wall, obscuring the endoscopic view. This complicates the understanding of the relationship between the esophageal wall and the foreign object, prolonging the procedure and increasing associated risks.8,9 Consequently, it is no longer the primary choice for foreign body diagnosis. While endoscopy remains the favored method for foreign body retrieval, it lacks a clear view of the tube wall and surrounding areas, escalating the risks of intraoperative and postoperative complications due to blind maneuvers. MSCT, boasting superior density and spatial resolution, coupled with its capacity for isotropic volume scanning that produces high-quality MPR images, can precisely delineate the position, shape, and surrounding relationships of foreign bodies, offering substantial assistance for subsequent treatment. MSCT is also invaluable for post-endoscopic reexamination when necessary, providing crucial assistance in clinical decision-making concerning the identification of post-procedural complications.
In this study, the majority of cases involving esophageal jujube pit impaction pertained to elderly individuals, with the esophageal initial segment identified as the most prevalent site of impaction, aligning with prior literature.10,11 The heightened incidence among the elderly is attributed to age-related physiological declines, including reduced chewing ability and diminished sensitivity in oral mucosal muscles, often exacerbated by tooth loss, leading to an increased risk of inadvertent swallowing. The esophageal entrance, constrained by the cricoid cartilage pressing against the cervical vertebrae due to cricopharyngeal muscle contraction, emerges as the narrowest of the 3 anatomic esophageal constrictions, making it more susceptible to impaction. Continued consumption following initial impaction, in some cases, may push the jujube pit downward, resulting in esophageal damage. In addition, the esophagus’s larger transverse diameter compared to its anteroposterior diameter explains the predominance of lateral impactions. Once impacted, the esophagus’s natural contractions and peristaltic movements can easily cause the sharp ends of the jujube pit to pierce its wall. MSCT plays a pivotal role in accurately determining the impaction site and delineating the shape and length of the jujube pit. On imaging, most jujube pits exhibit peripheral high density with central low density, occasionally resembling a gas-like appearance, a variation related to the type and age of the jujube pit. Precise measurements of the jujube pit’s length and its angle with the esophageal longitudinal axis on CT images provide essential information for treatment planning.
MSCT not only displays the impaction site but can also be used to accurately assess the relationship between the impacted jujube pit and adjacent organs, as well as the presence of perforation. A comparison of the angle between the jujube pit and the esophageal longitudinal axis with the occurrence of perforation revealed that in cases where the angle was less than 30°, the pit typically penetrated at one end with shallow depth and post-endoscopic removal, there was generally no esophageal mucosal damage. In cases with an angle of 30° to 60°, impaction often involved both ends of the pit, with one end penetrating more deeply. During endoscopic procedures, the shallower end was addressed first, followed by the deeper end, and postoperatively, mucosal erosion was common, but perforation was not observed. Cases with an angle of 60° to 90° had a higher likelihood of perforation. Transversely impacted pits are more prone to penetrate the esophageal wall. In addition, in some patients, continued consumption of food after inadvertently swallowing the pit caused transverse impaction, leading to secondary esophageal injury or even perforation. Considering that the adult esophagus wall is relatively thin, about 3 to 4 mm, and lacks a serosal layer, being composed only of loose connective tissue with abundant elastic fibers, it is more susceptible to rupture when a jujube pit impacts.
Surgical suturing of the esophagus is particularly challenging due to its anatomical structure. Esophageal perforation is a grave complication that can lead to esophagotracheal fistula, especially in the thoracic segment, where an esophageal aortic fistula can occur, significantly increasing mortality rates. In CT imaging, the direct indicator of perforation is the presence of a gas shadow around the wall of the tube at the impaction site. However, not all perforation cases exhibit this sign. In this study, out of 5 cases of perforation formation, imaging only showed surrounding bubble shadows in 3 cases. The other 2 cases did not display this sign, and intraoperative findings revealed that the perforation was covered and wrapped by inflammatory tissue, preventing gas from escaping the esophageal lumen. The results of some studies suggest that the conventional abdominal window width and level used in observing images may overlook subtle gas shadows, and utilizing an increased window width may help in diagnosing such conditions.12,13 In a particular case lasting 48 hours, notable exudate was evident in the CT image, and endoscopy revealed the formation of pus in the perforation. Reports indicate a direct correlation between the duration of foreign body impaction and the incidence of complications.14,15 Accurate preoperative diagnosis can provide valuable references for clinical treatment, and CT excels in displaying perforation and surrounding abscesses.
In the endoscopic removal of jujube pits, tools such as alligator forceps, transparent caps, and net cage sleeves are commonly used.16,17 The approach and technique vary depending on the jujube pit’s position and the extent of wall penetration. MSCT MPR can vividly display the shape of the jujube pit or its sharper end, whether the impaction involves one or both ends, and the relationship between the impacted pit, the trachea, and blood vessels. Preoperative CT provides crucial references for selecting endoscopic instruments and surgical methods. If preoperative findings indicate that the impacted jujube pit is at the level of the aorta, direct endoscopic removal is risky. In instances of this nature, a combined approach involving thoracoscopy and endoscopy may be employed. This entails the separation of the aorta from the esophagus to a safe distance under thoracoscopic guidance before initiating the endoscopic procedure.18,19
Esophageal impaction of jujube pits represents a common and urgent scenario encountered in gastroenterology and emergency medical settings. Precise diagnosis is paramount in determining the most suitable treatment strategies and evaluating posttreatment results. MSCT, with its superior density resolution, thin reconstruction layers, and MPR capability, facilitates a comprehensive and multidimensional examination of the impaction site. It effectively enables the analysis of the interactions between the jujube pit, the esophageal wall, and surrounding tissues and organs, while concurrently detecting complications such as perforation and adjacent abscesses. In clinical practice, MSCT imaging data guide the selection of optimal treatment approaches and assists in choosing appropriate surgical instruments. In addition, computer-assisted software facilitates simulated endoscopy, contributing to increased procedural success rates, reduced operation durations, and minimized intraoperative and postoperative complications. MSCT plays an indispensable role in the diagnosis and management of esophageal jujube pit impaction, serving critical functions in preoperative, and postoperative care. For cases that only require endoscopic treatment, intraoperative MSCT has high feasibility. If the clinician has a need, the endoscope machine can be moved to the CT room for intraoperative MSCT. However, for complex cases that require thoracoscopy or open-heart surgery, the application of intraoperative MSCT has significant limitations.
Conclusion
In conclusion, MSCT imaging is essential in the diagnosis and management of esophageal impaction of jujube pits. Its excellent resolution and multidimensional capabilities enable accurate diagnosis, assessment of complications, and guidance in treatment approaches. MSCT, combined with computer-assisted software, optimizes patient care throughout all stages of management.
Footnotes
Author Contributions
Zhong-Xing Dong and Dong Zheng conceived the idea and conceptualized the study. Xiao-Ying Wang, Yang Zhao, and Kai Xu collected the data. Jun-Hua Liu, Jie Cui, Ru-Yi Yan, and Kai Xu analyzed the data. Jun-Hua Liu, Jie Cui, Ru-Yi Yan, Xiao-Ying Wang, and Yang Zhao drafted the manuscript, then Zhong-Xing Dong and Dong Zheng reviewed the manuscript. All authors read and approved the final draft.
Availability of Data and Materials
We declared that materials described in the article, including all relevant raw data, will be freely available to any scientist wishing to use them for noncommercial purposes, without breaching participant confidentiality.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of PLA Strategic Support Force Characteristic Medical Center. This study was conducted by the Declaration of Helsinki. Written informed consent was obtained from all participants.
Consent for Publication
Not applicable.