
Abstract
Objective:
We aimed to evaluate the effect of autologous platelet-rich plasma gel (PRPG) on fat graft myringoplasty (FGM) in tympanic membrane perforations caused by chronic otitis media.
Methods:
This retrospective study involved 63 patients who underwent operations between 2015 and 2018. Fat graft myringoplasty was performed with the transcanal approach with and without the use of PRPG in the surgical field. The patients were classified into 2 groups: group A, which included 32 patients who underwent FGM with the use of autologous PRPG, and group B, which included 31 patients who underwent FGM alone. Tympanic membrane perforations were divided into 2 groups: small perforations (1-2 mm) in a single quadrant and large perforations (2-4 mm) in at least 2 quadrants.
Results:
Both groups were statistically matched regarding age and sex. The mean postoperative follow-up was 11.6 and 12.1 months for groups A and B, respectively. Four months postoperatively, the success rate of the graft in group A (100%) was significantly higher than that in group B (83.8%; P = .03). The preoperative and postoperative median air–bone gaps of the groups were similar (P = .653 and P = .198, respectively). No worsening of the air–bone gap was noted postoperatively in either group.
Conclusions:
This study demonstrated that autologous PRPG application during FGM allows for a higher success rate than FGM alone. Furthermore, the use of PRPG with FGM for large perforations increases the success rate. Further studies are needed to investigate the PRPG healing effect on other tympanic membrane perforation closure techniques.
Introduction
Persistent tympanic membrane (TM) perforations represent one of the most widespread problems encountered in otology. Patients with TM perforations must prevent their ears from being exposed to water. Furthermore, these patients may experience discharge and middle ear infections. Many reconstructive procedures have been used for TM perforation closure, including overlay and underlay techniques with temporal fascia muscle, sponge gel (Gelfoam; Pfizer, New York, NY) patches, autologous fat grafts, paper patches, and hyaluronic acid (HA) ester patches (Epifilm; Medtronic, Minneapolis, Minnesota). 1 -3 Since 1962, fat graft myringoplasty (FGM) has been used as a suitable method to close persistent TM perforations. 4,5 According to the findings in the literature, the success rate after FGM varies from 79% to 91%. 6,7 Previously, individual attempts were made to use supporting material in otology. Saliba et al 8 used HA with FGM (ie, hyaluronic acid fat graft myringoplasty [HAFGM]) and achieved a higher success rate than the results reported for FGM alone. 8 Erkilet et al 9 asserted that in rats, the autologous platelet-rich plasma (PRP) effectively accelerated TM perforation healing. To improve the success rate of myringoplasty, El-Anwar et al 10 applied topical autologous PRP in an underlay graft technique using a conchal perichondrial graft.
Platelet-rich plasma is an autologous blood product that contains concentrated platelets above the basal level (150 000-350 000/μL). To understand how PRP functions in tissue regeneration, we should examine the content of PRP, which includes many autologous growth factors such as platelet-derived growth factor (PDGF) and epidermal growth factor. All these molecules in PRP have significant functions, such as cell proliferation, migration, and angiogenesis. Fibrin and fibronectin are essential proteins in PRP that provide the structural support needed for the cell migration, cell proliferation, and 3-dimensional growth of tissues. Platelet-rich plasma can also be used in the extracellular matrix to stimulate and repair tissues. 11,12
Platelet-rich plasma can be easily obtained by noninvasive blood extraction and manipulation. The purpose of this study is to retrospectively assess the success rate and hearing improvement of 63 patients who underwent FGM with and without platelet-rich plasma gel (PRPG) in the surgical field.
Materials and Methods
In this study, FGM procedures with and without the use of PRPG for TM perforations caused by chronic otitis media were retrospectively compared in the department of otolaryngology of a tertiary center. The study protocol was approved by Medical Faculty and Hospital Ethics Committee (07/09/2017-71.07.06.), and all procedures were in accordance with the ethical standards of responsible committee on human experimentation (institutional and national) and with the 1975 Declaration of Helsinki, as revised in 2008. Additional informed consent was obtained from all patients whose data are included in this article. Preoperative and postoperative records of age, gender, affected side, TM perforation site, perforation size, perforation healing, improvements in hearing, and complications were obtained from the registered patient charts in the hospital’s electronic medical record system. Of the screened patients, 63 were included in the study, and these patients were split into 2 groups: group A, 32 patients with PRPG, and group B, 31 patients without PRPG. Patients were excluded from the study based on the following criteria: current tobacco use, marginal TM perforation (more than 4 mm), active infection, diabetes, the presence of cholesteatomas, suspected ossicular problems with an air–bone gap (ABG) greater than 35 dB, extensive tympanosclerosis in the tympanic remnant, active neoplasms, hematologic and autoimmune disease, and the immunosuppressive treatment.
Study Procedures
The patients underwent FGM via the transcanal approach under local anesthesia with and without the use of PRPG on the outer face of the TM remnant and fat graft. Specifically, our attention was focused on the postoperative success rate and the hearing improvement. The patients’ ears were preoperatively examined using pure-tone audiometry and microscopic otoscopy, and each TM perforation was documented preoperatively and in the 1st, 4th, and 12th postoperative months with 0° angulation telescope images. The size of perforations was measured intraoperatively using dissector (Thomassin; Karl Storz, Tuttlinguen, Germany) that was double-ended, distal tips angled 90° to the right or left. Saliba 13 described perforation size subdivisions based on the size of the 4 TM quadrants, and in our study, we used the same process with minor modifications. Perforations in a single quadrant were considered small (1-2 mm), whereas the perforations in at least 2 quadrants were considered large (2-4 mm). Marginal perforations (>4 mm) in 3 or more quadrants were excluded from the study. The patients were evaluated based on their postoperative eardrum status and the improvements in their ABG. The success criteria for the perforation closures was determined from the intact TM 4 months after the operation. Any residual perforation was considered as a failure. The audiogram results were obtained preoperatively and postoperatively (at least 4 months after the operation), and these results were used to assess the hearing improvement. Changes in ABG were used as hearing parameters. The ABG was computed as the mean difference between bone conduction and air conduction at 0.5, 1, 2, and 4 kHz.
Preparation of PRPG
Different methods are used to prepare PRPG, including the use of commercially available kits or the use of laboratory methods, such as that used by Landesberg et al, 14 in which 10 mL of blood was drawn from the brachial vein of the patients into vacutainer tubes that either contained 0.5 mL 0.129 mol/L sodium citrate or 0.048 mL of 15% EDTA (or K3) solution (Becton Dickinson, Franklin Lakes, New Jersey). The vacutainer tubes were carefully inverted several times to homogenize the blood with anticoagulant. The tube was centrifuged at 800 rpm for 10 minutes in an NF 800R centrifuge (NÜVE, Ankara, Turkey). Using an 18-G needle (Jelco; Smiths Medical, Plymouth, Minnesota), all the plasma was transferred to a 15-mL conical polypropylene tube (Corning, Corning, New York) and centrifuged at 800 rpm for 10 minutes. The upper and lower halves of the preparation were designated the platelet-poor plasma and PRP, respectively. Platelet-rich plasma gel was manufactured with the addition of thrombin/calcium chloride. A thrombin–calcium chloride solution was prepared with 5000 units of bovine thrombin (Thrombin-JMI; GenTrac Inc, Middleton, Wisconsin) dissolved in 5 mL of 10% calcium chloride. Then the solution was transferred to a sterile tube (Eppendorf; Eppendorf AG, Hamburg, Germany) using a syringe. For each 1 mL of PRP, 0.167 mL of the thrombin–calcium chloride mixture was added and left to solidify in the safe-lock tube (Eppendorf; Eppendorf AG) at 37°C in a water bath.
Commercial kits were used to isolate PRP in another protocol. Venous whole blood was collected from the patients into 10 mL Regen BCT tube containing cell separator gel (Regen Lab SA, Le Mont-Sur-Lausanne, Switzerland). 15 Each tube contained 1 mL of sodium citrate as an anticoagulant. The tubes were inverted several times to homogenize the blood with the anticoagulant, and then they were centrifuged at 3000 rpm for 5 minutes. A volume of 1 mL of calcium gluconate was added to the resulting supernatant. Following this, PRPG was removed with sterile surgical forceps and separated from the part remaining in the tubes (Figure 1). The commercial PRP kits cost an average of US$22 per patient.
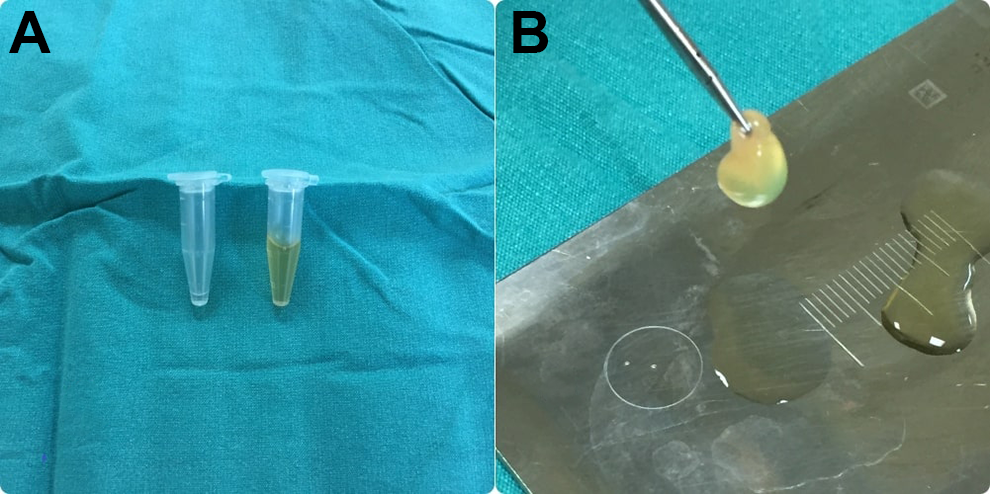
A, Thrombin–calcium chloride solution and platelet-rich plasma. B, Platelet-rich plasma gel.
Surgical Techniques
All patients underwent operations under local anesthesia. A single surgeon (the corresponding author) performed all surgeries.
Fat graft myringoplasty with the PRPG technique: A local anesthetic injection (1% lidocaine with 1:100,000 epinephrine) was administered in the 4 quadrants of the ear canal and to the ear lobe. Through a small incision in the rim of the ear lobe, a small piece of adipose tissue was removed and stored in saline solution. The incision was closed with several 6-0 polypropylene sutures. Using 0° angulation telescope visualization, the edges of the perforation were deepithelialized with a sharp prick. To support the fat graft, pieces of sponge gel (Gelfoam; Pfizer) were passed through the perforation into the middle ear. A piece of the previously removed adipose tissue was then inserted through the perforation in a grommet tube fashion.
In group A: After the fat graft and adjusted in its place, PRPG was inserted into the external auditory canal (EAC) on the outer face of the TM remnant and fat graft. Special attention was given to obtaining close contact among the PRPG, TM, and fat graft. Then the PRPG was covered with sponge gel (Gelfoam; Pfizer) pieces soaked in saline, and the EAC was filled with nitrofurazone ointment (Furacin; Zentiva, Prague, Czech Republic).
In group B: The fat graft covered the pieces of sponge gel (Gelfoam; Pfizer) soaked in saline, and EAC was filled with nitrofurazone ointment (Furacin; Zentiva).
In both groups, the patients were instructed to instill ofloxacin otic drops in the EAC and take oral ciprofloxacin twice daily, avoid blowing their nose, and observe water precautions.
Statistical Analysis
Data were analyzed using the Statistical Package for Social Sciences, version 21 (SPSS Inc, Chicago, Illinois). Quantitative data on the FGM with PRPG and FGM alone groups were compared using a t test. Categorical variables were compared with a χ2 test for sex, and Fisher exact test was used for the other outcome results. A P value less than .05 was considered significant.
Results
Of the screened patients, 63 were included in the study. Of these 63 patients, 10 males (31.25%) and 22 females (68.75%) were in group A and 10 males (31.25%) and 22 females (68.75%) were in group B. There was no statistically significant difference in gender between the 2 groups (P = .754). The average ± SD ages for groups A and B were 23.9 (±9.13) and 21.9 (±10.51), respectively, and there was no statistically significant difference in age between the 2 groups (P = .445). The groups were similar in terms of TM perforation size (P = .182; Table 1).
Comparison Between the Studied Groups Regarding Age, Sex, and Perforation Size.
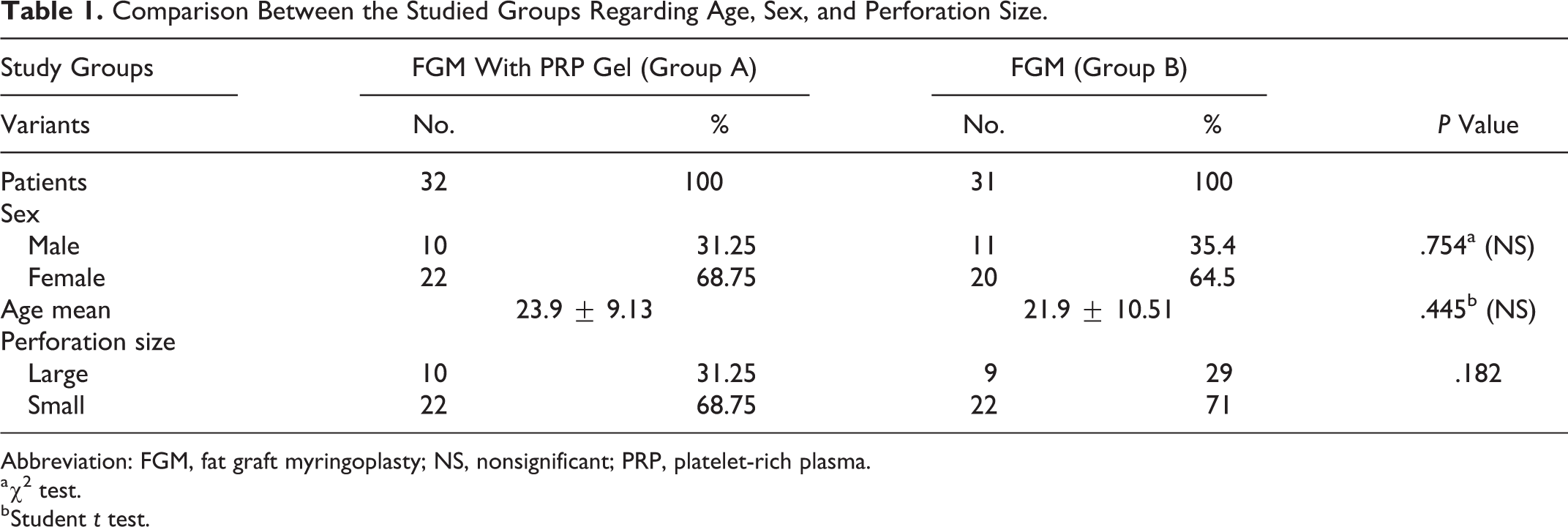
Abbreviation: FGM, fat graft myringoplasty; NS, nonsignificant; PRP, platelet-rich plasma.
a χ2 test.
b Student t test.
The average postoperative follow-up periods for groups A and B were 11.6 and 12.1 months, respectively. Four months postoperatively, the graft success rate in group A (100%) was significantly higher than that in group B (83.8%; P = .03). The preoperative and postoperative median ABGs of the groups were similar (P = .653 and P = .198, respectively). No worsening of the ABG was noted postoperatively in either group. The average ± SD hearing gains for groups A and B were 10.3 ± 6.74 dB and 7.23 ± 6.72 dB, respectively, and there was no statistically significant difference in these gains (Table 2). The FGM with PRPG technique resulted in a significantly higher success rate for large perforations than FGM alone (P = .01; Table 3).
Success Rates According to Graft Taking and ABG, Mean Hearing Results.
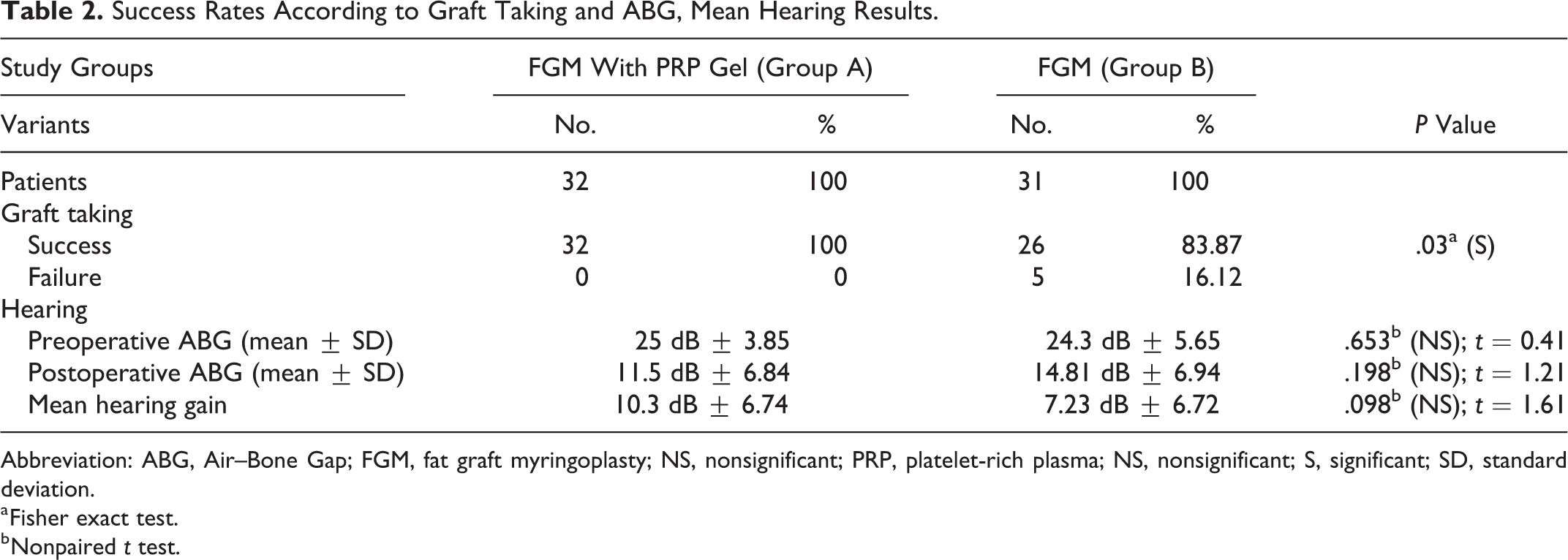
Abbreviation: ABG, Air–Bone Gap; FGM, fat graft myringoplasty; NS, nonsignificant; PRP, platelet-rich plasma; NS, nonsignificant; S, significant; SD, standard deviation.
a Fisher exact test.
b Nonpaired t test.
Success Rates According to Perforation Size.
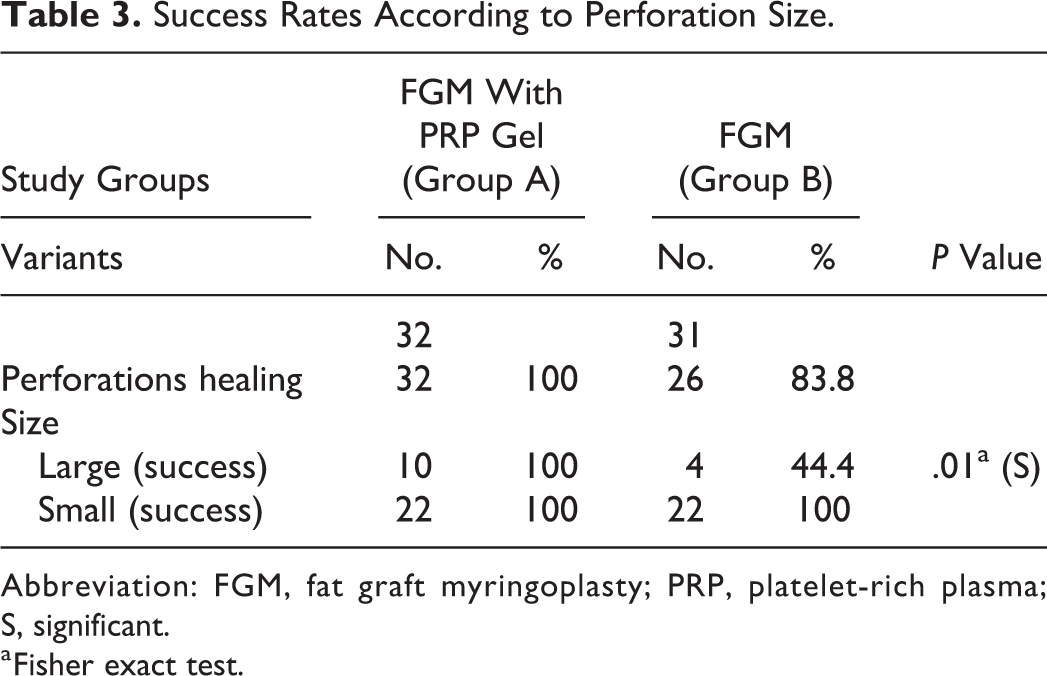
Abbreviation: FGM, fat graft myringoplasty; PRP, platelet-rich plasma; S, significant.
a Fisher exact test.
In cases of failure, a residual perforation was identified within the first 4 postoperative months. During the follow-up period, no graft was lateralized or displaced into the middle ear and no retraction pockets were observed. No infections were detected in either group. In group A, some adipose tissue remained under the new epithelium of the healed TM 4 months after the operation.
Discussion
Otologists have been attempting to close TM perforations for 300 years. 1 Various graft materials have been used for this purpose. Currently, the most commonly used graft materials are temporalis fascia and cartilage perichondrium. 16 However, these grafts require a postauricular or endaural incision, preparation of a tympanomeatal flap, and may cause injury to the middle ear ossicles, tympanic annulus, or chorda tympani. Ear lobe adipose tissue was first introduced as a graft substance for repairing TM defects in 1962 first by Ringenberg. 4 Many authors have reported high success rates for FGM (76%-92%) and minimal morbidity, mostly for the closure of small TM perforations. 6,7,17 Moreover, FGM has some advantages; it is generally performed with the transcanal approach, which is easier to perform under the local anesthesia than the other approaches applied in classic myringoplasty. Successful FGM closure is commonly observed in the small TM perforations with better audiological results, whereas the rates of graft failure were have been found to be higher for large perforations. 17,18 Saliba 13 observed that the addition of HA ester films to FGM (ie, the HAFGM technique) allowed for a high success rate for perforations of all sizes and in all quadrants in cases where it was possible to completely visualize the epithelial margin. 8,18 However, PRPG has some advantages over HA ester films; it is a cost-efficient autologous material that does not have a graft rejection risk. Gün et al 19 recommended the HAFGM procedure to achieve a flat TM postoperatively and better audiological results, which make the technique a better procedure than that of FGM for large perforations. Prior et al 20 recommended against the use of HA ester films alone to repair TM perforations. In all 5 of the patients in their study, although the HA dissolved, the perforations remained the same size. 20 In our series, the overall success rate for FGM alone was 83.8%, which is comparable to that in other studies conducted mainly on small perforations. In this study, we found that FGM with PRPG resulted in more effective TM perforation closure than the FGM alone. The results of this study confirm that the FGM-PRPG is a superior technique to FGM alone and reveal that PRPG is important in TM healing.
Deddens et al 21 thought that TM perforation size is a critical factor for successful FGM and, accordingly, applied the FGM procedure for perforation sizes between 5% and 30% of the TM surface. In his study, Stenfors 22 concluded that if a TM perforation is dry and less than 1 quadrant in size, HA treatment could be an alternative to myringoplasty. Konstantinidis et al 18 emphasized that the success rate of FGM decreases significantly if the perforation size is over 30% of the pars tensa. Specifically, the low success rate of FGM alone for large perforations impelled us to use a new material that enhances healing during FGM for TM perforations in at least 2 quadrants. In our study, the success rate of TM perforation closure was 100% in the group that underwent FGM-PRPG for large TM perforations (Figure 2). Moreover, all failed treatments were performed on large perforations in the FGM alone group.
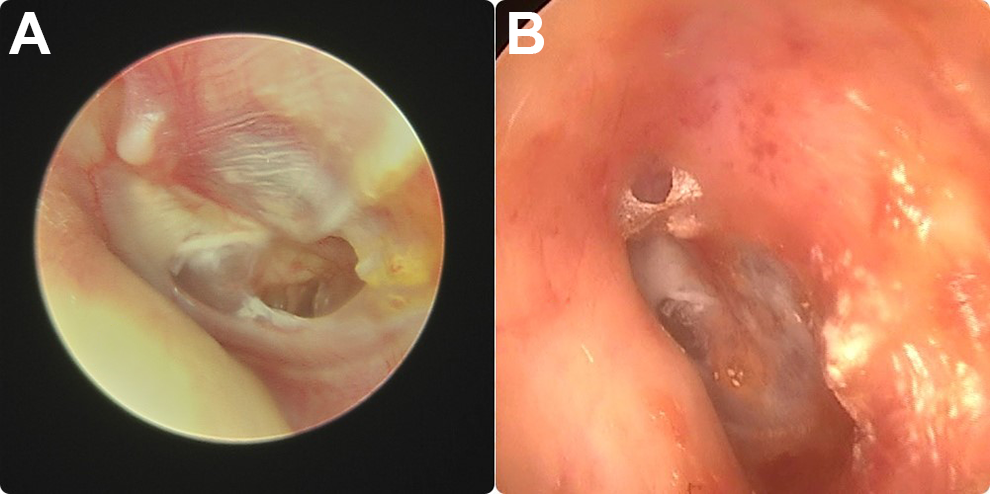
A, Endoscopic preoperative view of right ear with central medium size tympanic membrane (TM) perforation. The fat graft myringoplasty was performed with addition of platelet-rich plasma gel. B, Endoscopic 4-month postoperative view of the same ear showing a fatty adipose tissue behind intact TM.
In the first animal study that used PRP in TM perforations, Erkilet et al 9 documented that PRP effectively accelerated TM perforation healing, and the authors suggested that PRP may be effective in humans, especially because it is an autologous material. In another experimental study, Aksoy et al 12 showed the benefits of using PRP with fat grafts to repair the TM perforations in a rat model with histopathological findings. They showed that the degree of normal adipocyte area and the number of mature vessels in the PRP group were significantly higher than those in the control group, and they had better granulation tissue area and vacuolization area results. 12 In the first clinical study of topical autologous PRP to repair large TM perforations, El-Anwar et al 10 revealed that the treatment safely and effectively improved the success rate of underlay myringoplasty. Saeedi et al 23 reported that adding PRP to conventional sponge gels used in TM perforation repair increased the complete healing rate of TM perforation with fewer complications and less morbidity. Fouad et al 24 found that FGM alone achieved significantly lower success rates than the HAFGM and PRP-FGM. In addition, they found no significant difference between the PRP and HA. 24
Platelets are the key element of the coagulation system, as they activate hemostasis and the healing process. Platelet-rich plasma contains a high concentration of platelets and can be activated to form PRPG and release PDGF for the therapeutic use. Alpha granules of the nonactivated platelets in PRP contain PDGF, and therefore, they are not functional because they are not released or in contact with the tissue. The platelets must be activated to release these growth factors. The PDGFs of the platelet gel are the peptides that enhance cell proliferation, differentiation, chemotaxis, and migration. They have a significant role in healing. Mixing PRP with thrombin and calcium chloride will activate the platelet concentrate and produce a viscous PRPG solution. Platelet-rich plasma gel is applied as a solid jelly mass to wounds. 25 In our study, PRP was transformed into a PRPG and we used it with FGM. Our success rate was higher than that in similar studies that did not use the gel form of PRP (Table 4). In a study that used PRP in FGM by Fouad et al, 24 the success rate was slightly lower (85.7%) than that in our study (100%). Alhabib and Saliba 26 found the results for PRP myringoplasty were significantly worse than those for HAFGM, and because of the negative results with PRP, the study was not completed. We did not use PRP alone but used PRPG in addition to FGM. Our findings were consistent with those in the studies by Navarrete Álvaro et al 27 and El-Anwar et al. 10
Reports of PRP-FGM Procedures in the Literature.
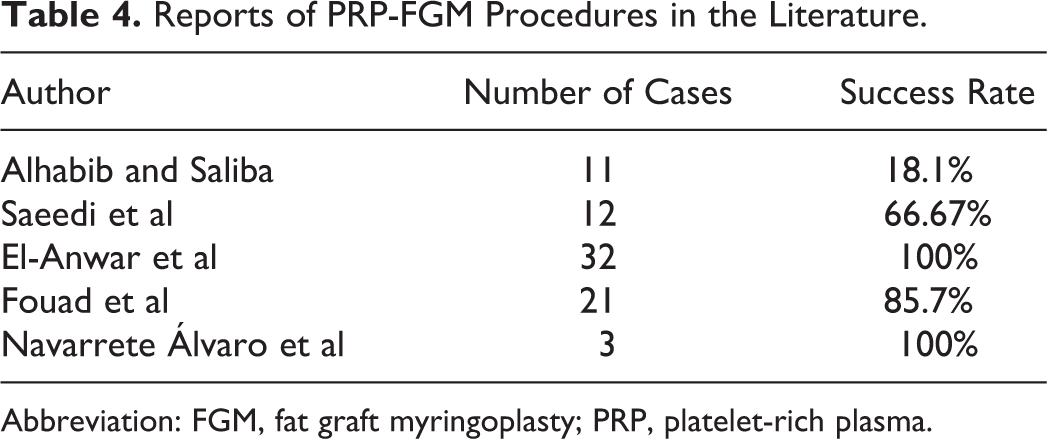
Abbreviation: FGM, fat graft myringoplasty; PRP, platelet-rich plasma.
Unfortunately, the number of studies using PRP and PRPG in TM perforation repair is insufficient. This study is the first clinical study on topical platelet gel application in FGM during the repair of TM perforations caused by chronic otitis media that achieved a significant success rate for healing, which reveals that PRPG application in FGM is safe and highly effective.
Conclusion
This study shows that autologous platelet gel application during FGM has a higher success rate than FGM alone. There were no statistically significant differences between the audiological results between patients who underwent FGM-PRPG and patients who underwent FGM alone. Specifically, FGM alone is not satisfactory for large perforations. Furthermore, the use of PRPG with FGM for large perforations increases the success rate. Further studies are needed to investigate the platelet gel’s healing effect on other TM perforation closure techniques.
Footnotes
Author Contributions
T.E. contributed to conception, design, supervision, materials, data collection and/or processing, analysis and/or interpretation, literature search, and writing manuscript. E.G. contributed to materials and critical review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.