
Abstract
Objectives:
The purpose of this study is to explore the curative effect of open surgical excision and endoscopic radiofrequency ablation (RA) in the treatment of piriform fossa fistula (PSF).
Methods:
Retrospective study of 80 cases of PSF in the Department of Otolaryngology-Head and Neck Surgery, Shanghai Children’s Hospital, from June 2009 to June 2017.
Results:
In this series, there were 43 males and 37 females, and the mean age was 5.2 years (17 days to 12 years). Surgical excision was performed for 62 patients. Radiofrequency ablation was performed for 18 patients. Six cases of postoperative temporary hoarseness occurred, and the hoarseness rates were not significantly different between the excision and RA groups (6.4% vs 11.1%, respectively, P = .88). Two cases of temporary neck abscess occurred in the RA group. After the mean follow-up period of 3.1 years (1-8 years), no recurrence was found between the excision and RA groups.
Conclusions:
The curative effect of excision and RA for PSF is not significantly different; each of the 2 methods has its advantages and disadvantages. However, RA for PSF has the merit of being minimally invasive, easy to operate, and safe; this procedure seems to be more suitable in the clinic.
Introduction
Piriform fossa fistula (PSF) is a rare congenital anomaly derived from remnants of the third or fourth branchial structure and frequently shows as neck masses, neck inflammation, and repeated suppurative thyroiditis. Conventionally, the treatment consists of open surgical excision with or without hemithyroidectomy. In the last decade, an alternative treatment method is endoscopic cauterization of the internal opening in the pyriform sinus. Endoscopic methods include electrocauterization, chemocauterization, laser, fibrin glue, suture, or radiofrequency ablation (RA). 1,2 In our current study, we explored the curative effect of open surgical excision and RA for the treatment of PSF.
Materials and Methods
We retrospectively reviewed the records of 80 patients who were treated for PSF at the pediatric ENT department at Shanghai Children’s Hospital, China. This study was conducted with the approval of our institutional review board. Records from a total of 62 patients who had open surgical excision performed from June 2009 to June 2017 were collected. Records of 18 patients who had endoscopic RA performed from January 2016 to June 2017 were collected. Intraoperative rigid endoscopy method of examining the internal opening was the gold standard for the diagnosis of PSF. All the surgeries for PSF were accomplished by a senior physician. The selection of the surgical method was not controlled and was decided based on the parents. The medical records were analyzed for demographic details, clinical presentations, diagnosis method, surgical management, and complications. T test and χ2 test were used for the statistical analyses. P value <.05 was considered statistically significant.
For open surgical excision, patients were placed supine with the neck hyperextended under general anesthesia, the internal opening of pyriform sinus was exposed under rigid endoscopy, and methylene blue was injected from the internal opening to locate the fistula tract. We made a fusiform incision for the original scar or mass on the affected side; the lesions were commonly tracked to the lateral lobe pole of the thyroid and then went to the inferior cornu of the thyroid cartilage. Inferior pharyngeal constrictor muscle was longitudinally incised, and the back of the thyroid cartilage was lifted up; the lateral wall of the piriform fossa mucosa was stripped and exposed, and this mucosa turned into a blue cord-like structure, which was the result of the previous injection of methylene blue. High ligation and resection of internal fistula were performed. While the fistulous tract sometimes was impossible to identify and track because of severe inflammatory adhesion in the surrounding tissue, we could directly cut off the inferior pharyngeal muscle near the inferior cornu of the thyroid cartilage, lift up the thyroid cartilage, and expose and ligate the methylene blue–stained internal fistula (Figure 1). The patients were fed via nasal feeding for 3 days after surgery.
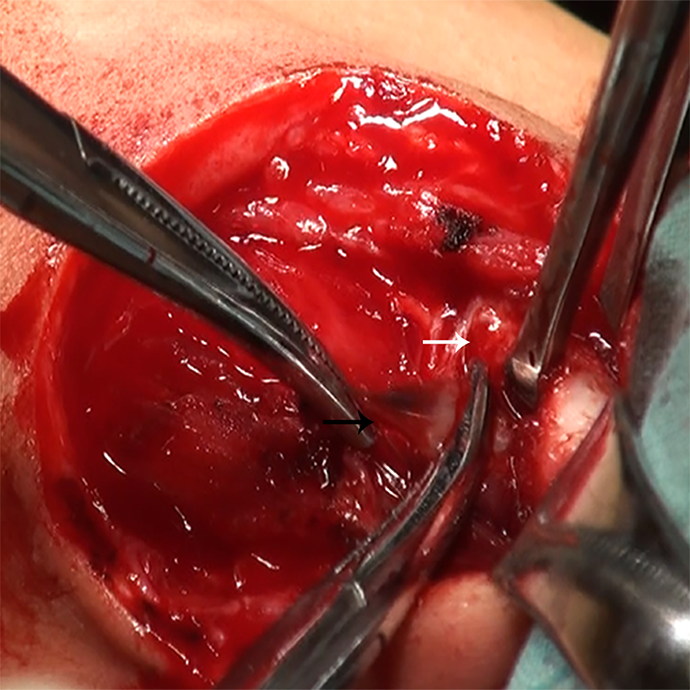
The back of the thyroid cartilage (the white arrow) was lifted up, and the lateral wall of the piriform fossa mucosa had turned into a blue cord-like structure (the black arrow), which was the result of previous injection of methylene blue.
For endoscopic RA, the internal opening of the PSF was identified under rigid endoscopy (Figure 2), and the diluted iodophor was used to disinfect the fistula tract. Radiofrequency ablation (EIC7070-01; American ArthroCare Corporation) was used to ablate not only the orifice of the fistula but also into the fistula tract located on the interior part of the thyroid cartilage until the orifice of pyriform fossa and surrounding mucosa formed eschar-like (Figures 3 and 4), and the power of RA was maintained at 7 to 10 W. For 4 patients in acute inflammatory stage of PSF, immediately after RA, external incision and drainage of the neck abscess was performed producing copious purulent substances; the skin wound was irrigated with hydrogen peroxide and packed with taped gauze. The patients in the endoscopic group were given a nasal feeding for 2 weeks.
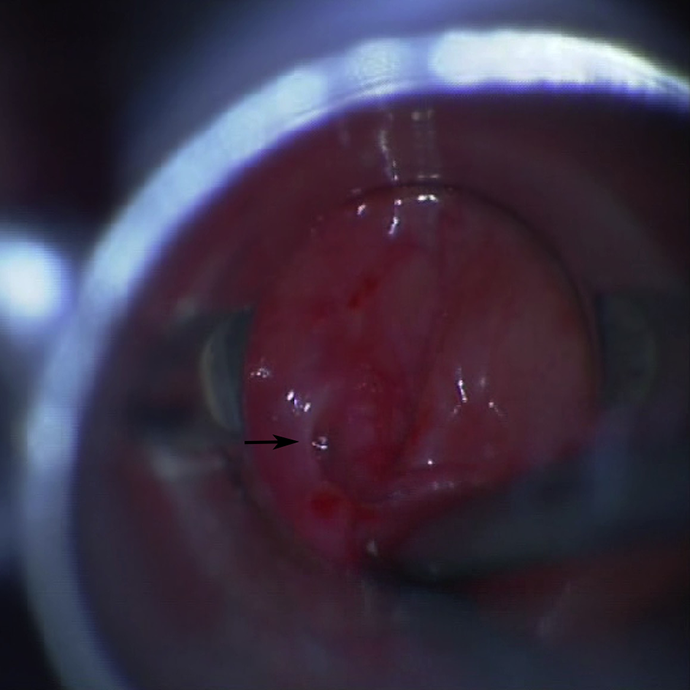
The endoscopic photographs showing the internal opening of pyriform sinus fistula (the black arrow).
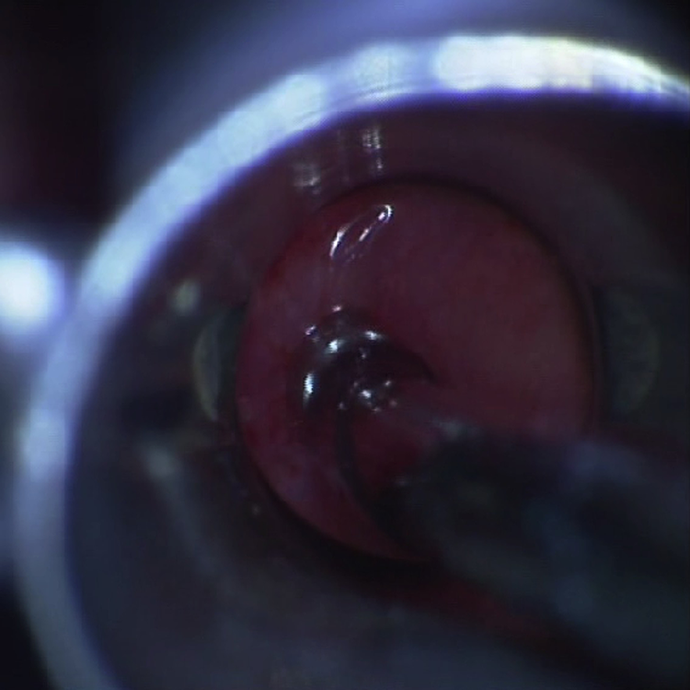
The internal opening was ablated using radiofrequency ablation.
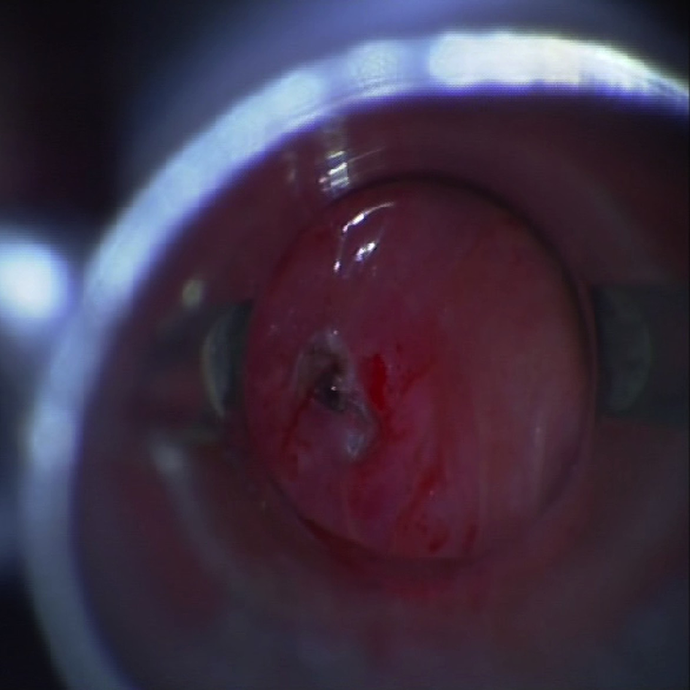
The internal opening of pyriform fossa and surrounding mucosa were then obliterated and formed eschar-like.
Results
The summary of 80 patients with PSF in this series is depicted in Table 1. The male to female ratio was 1.16:1. The mean age at operation was 5.2 years (range, 17 days to 12 years). The lesions were predominantly located on the left side (75/80, 93.8%), 42 (52.5%) cases had histories of incision and drainage, and 10 (12.5%) cases failed open surgical procedure at other hospitals. The clinical presentations included neck abscess, recurrent cervical inflammatory swelling, and suppurative thyroiditis. Due to the rarity of PSF, there were 19 (23.8%) patients who were misdiagnosed: 13 (16.3%) patients were misdiagnosed with acute thyroiditis, 4 patients with lymphadenitis, 1 patient with thyroglossal duct cysts, and 1 patient with a subcutaneous cyst.
Features of 80 Cases With Pyriform Sinus Fistula.
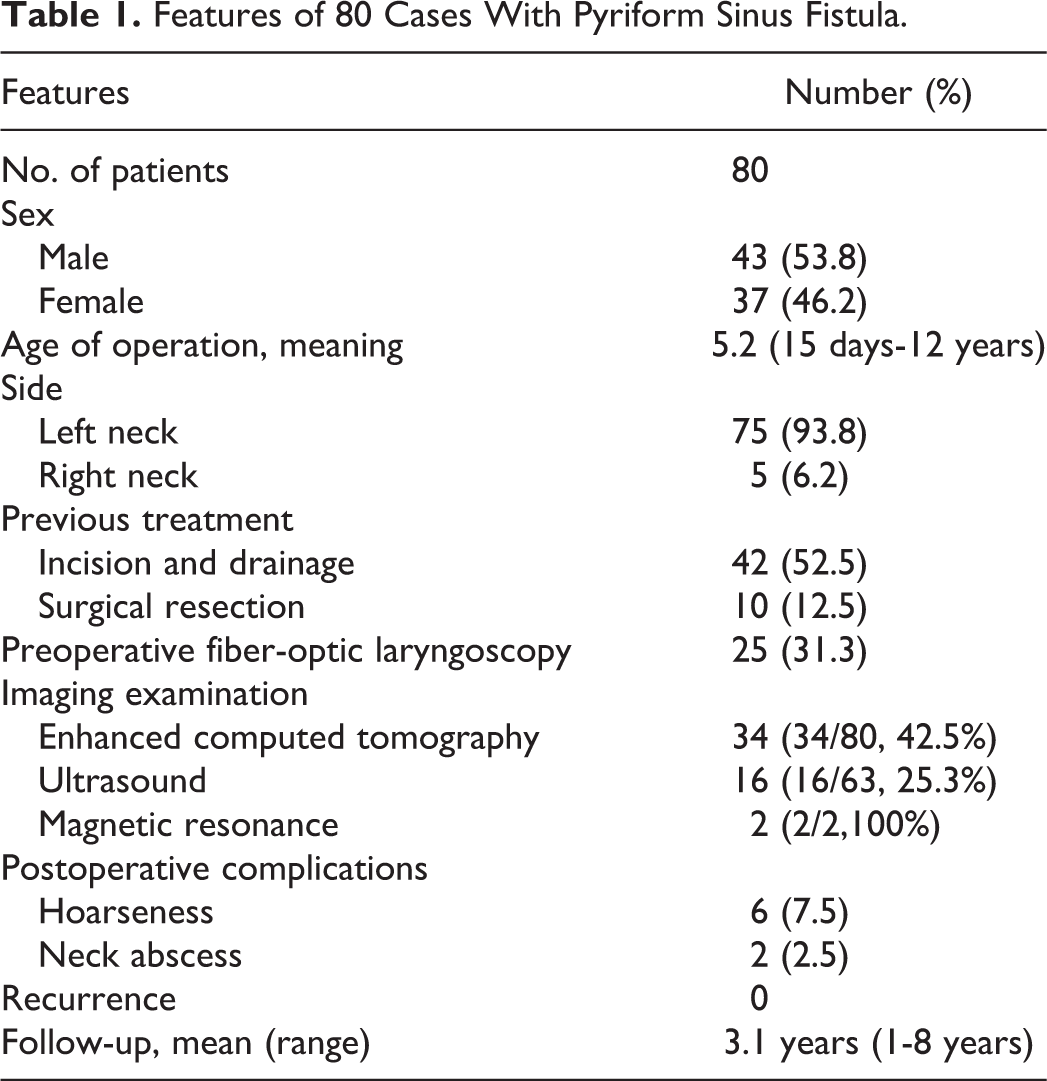
Preoperative fiber-optic laryngoscopy was performed to check the presence of the internal opening of PSF, but the diagnostic rate was only 31.3% (25/80, 31.3%). Enhanced computed tomography showed vague and uneven density lesions; 1 side of the thyroid was compressed by the lesion, suggesting thyroiditis, and there were 34 (34/80, 42.5%) patients diagnosed as PSF. Ultrasound presented the mixed thyroid echo area or hypoechoic area of the affected thyroid gland, and 16 (16/63, 25.3%) patients were diagnosed as PSF. Magnetic resonance imaging was performed in 2 patients, all diagnosed as PSF.
Open surgical excision of the fistula tract was performed for 62 cases, and 2 cases appeared hoarseness before the operation. During the procedure, 1 case had serious inflammatory adhesion around the recurrent laryngeal nerve, and release of the recurrent laryngeal nerve and surrounding fibrous tissue was performed. One case had ruptured recurrent laryngeal nerve near the thyroid cartilage, and anastomosis of the recurrent laryngeal nerve was performed. The postoperative hoarseness of 2 children was recovered. Endoscopic RA was performed for 18 cases (Table 2); for 4 cases in acute inflammatory stage, the affected side of the neck presented swelling pain, and RA combined with incision and drainage of the neck abscess were adopted. One case performed adenotonsillectomy simultaneously because of snoring at night.
Features of 18 Cases With Pyriform Sinus Fistula in the RA Group.
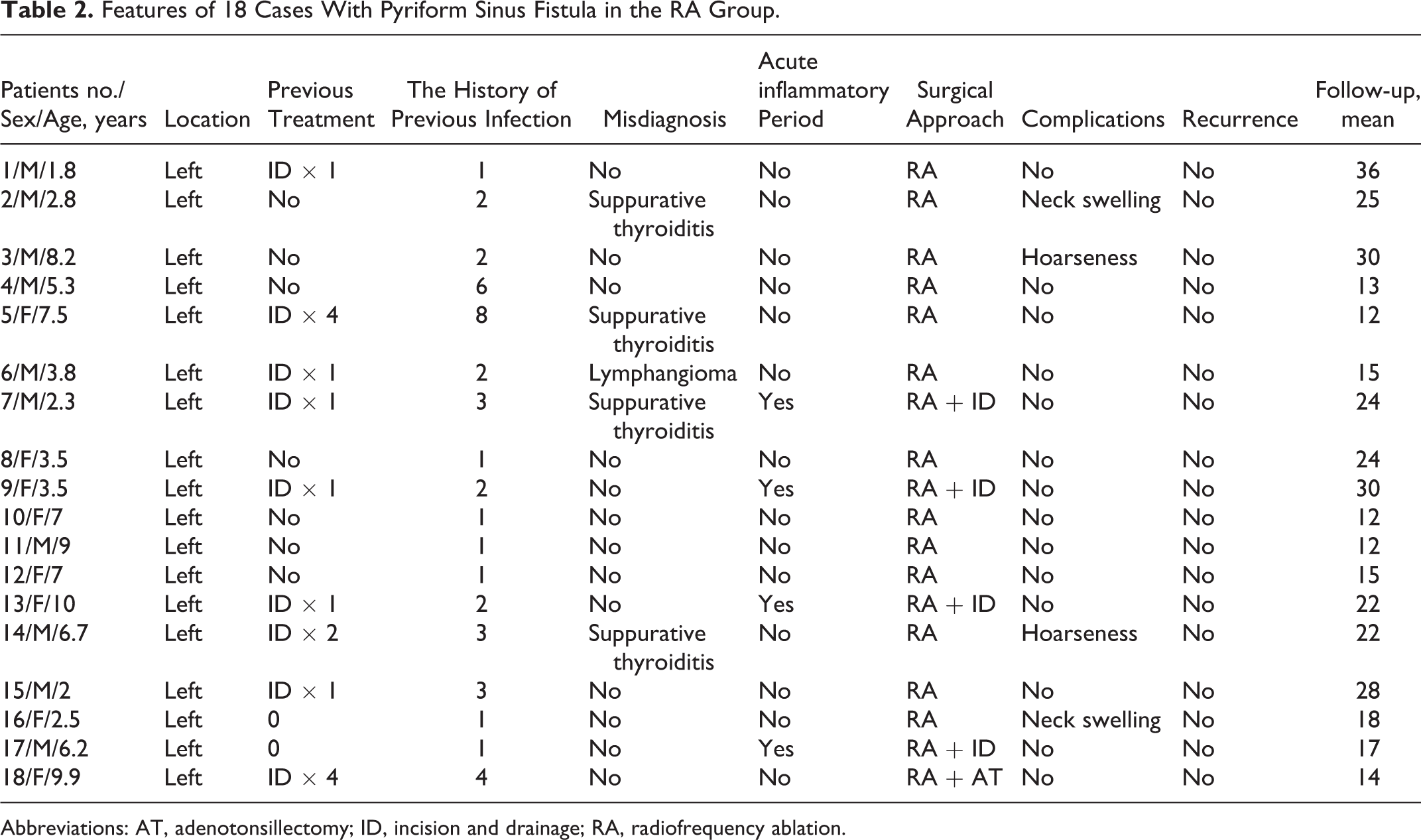
Abbreviations: AT, adenotonsillectomy; ID, incision and drainage; RA, radiofrequency ablation.
The postoperative period was uneventful in all cases. Six cases (the excision group: 4 cases; the RA group: 2 cases) occurred a temporary hoarseness, and these cases with the hoarseness symptom all recovered 1 month after treatment with hormones and nutritional neuro drugs. Two cases (2/18, 11.1%) appeared temporary neck abscess in the RA group. One case developed neck swelling and pain accompanied by fever on the 3 days after surgery (Figure 5). Abscess incision and drainage was given, and the neck symptoms improved after wound dressing for 7 days. One case presented a bulging lump in the left neck without obvious swelling and pain for 2 months after the operation; we intended to ablate the internal PSF opening again under rigid endoscopy, but the pyriform fossa mucosa was found to be intact, and the internal opening was closed. After treatment with intravenous antibiotics for 10 days, the neck mass gradually disappeared. After the mean follow-up period of 3.1 years (1-8 years), no recurrence was found between the excision and RA groups.

One patient developed neck swelling and pain (the black arrow) on the 3 days after RA surgery. RA indicates radiofrequency ablation.
Comparative analyses revealed that the hoarseness rates were not significantly different between the excision and RA groups (6.4% vs 11.1%, respectively, P = .88, Table 3). The excision group required longer operative times (mean 57.1 vs 10.4 minutes; P < .0001). Hospital stays also tended to be longer in the excision group (mean 6.8 vs 4.8 days; P = .002).
Open Surgical Excision Versus Radiofrequency Ablation.
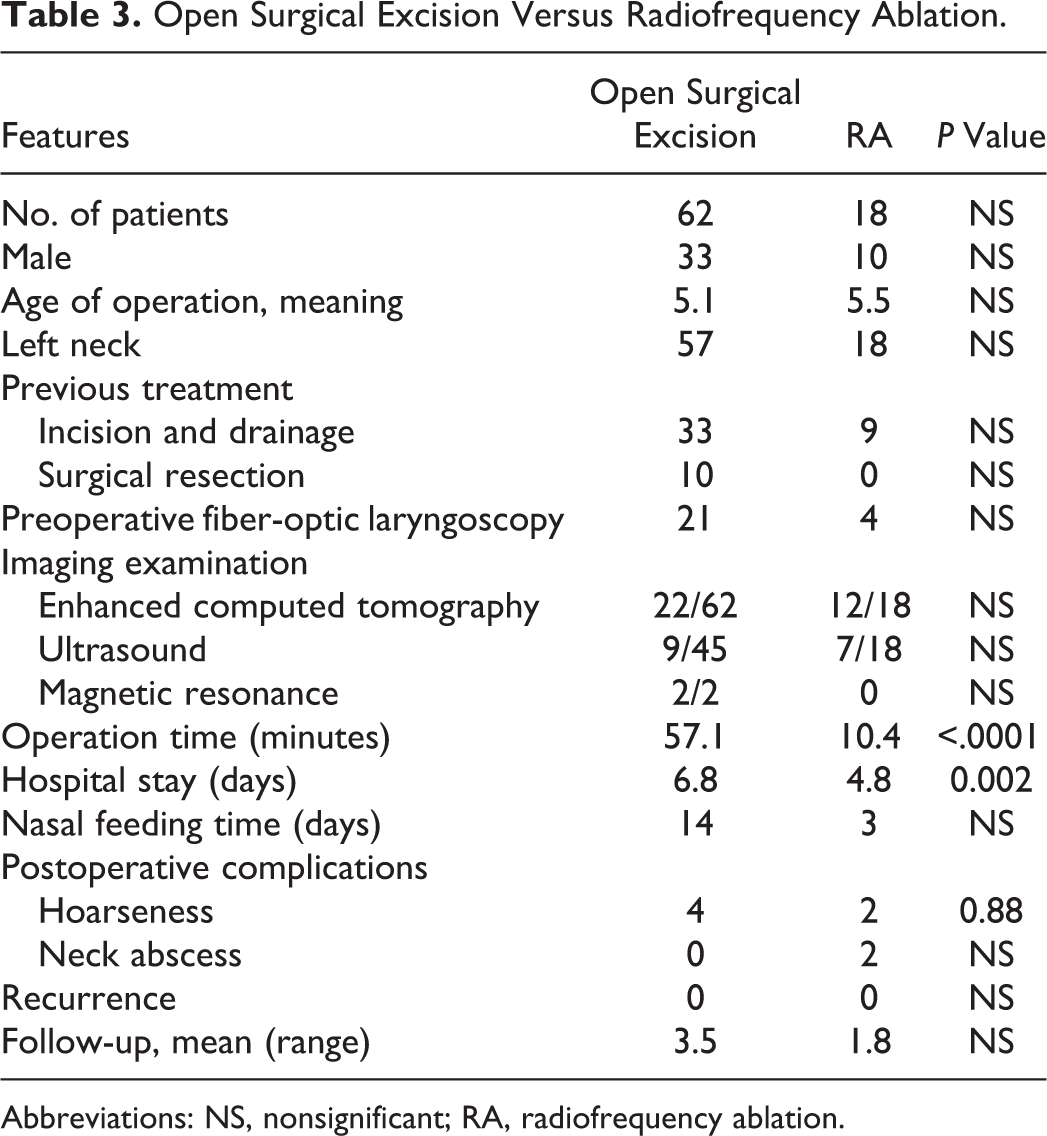
Abbreviations: NS, nonsignificant; RA, radiofrequency ablation.
Discussion
The typical treatment of PSF is open surgical excision. Complete excision of the fistulous tract with partial or hemithyroidectomy is essential during a quiescent period. If the procedure is executed in the inflammatory stage, it will be prone to infectious complications, accidental damage to the recurrent laryngeal nerve, and incomplete excision of PSF tract. Surgical drainage of pus is necessary in neck abscess and suppurative thyroiditis, which led to inflammatory adhesion in the surrounding tissue and made subsequent surgery more complicated. Intraoperative seek and high ligation of internal fistula are the key to ensure no recurrence but are often difficult and challenging. Endoscopy-assisted methylene blue injection or intubation through the internal opening can facilitate the exhibition of the tract during fistulectomy. 3 Some researchers reported that the cannulation of the tract with a guide light or wire was also effective. 4
The route of the fistula tract in each patient is inconsistent, which can penetrate the inferior cornu of thyroid cartilage or the inferior pharyngeal constrictor muscle when it emerges from the larynx. It was reported that resection of the inferior pharyngeal constrictor muscle and exposure of the inferior cornu of thyroid cartilage could help the dissection of the proximal part of the tract or even section excision of the posterior border of thyroid cartilage was necessary. In our current study, the advantage of fistulectomy was to lift up the thyroid cartilage and to ligate the fistula from the roots of the piriform fossa. This modified method was not only convenient for directly searching internal fistula, which was methylene blue–stained, but also may reduce the probability of recurrence. Thus, no recurrence was found in any of the PSF patients in the excision group.
The use of electrocautery or chemocauterization in the sinus tract or its cautery by laser has been described, mostly for PSF, but their efficacy is controversial. Sun et al 5 reported that 22 patients were treated with electrocautery; the success rate after initial cauterization was 91%, and no procedure-related morbidity was recorded. Ishinaga et al 6 demonstrated that 6 of 8 patients with PSF (75%) achieved obliteration of the fistula using electrocautery. However, Leboulanger et al 7 believe that electrocautery was inaccurate and inconvenient, and thermal diffusion may cause injury to the superior laryngeal nerve and recurrent laryngeal nerve.
Regarding chemocauterization, Yanagisawa et al 8 showed that the success rate of treatment for PSF after the primary chemocauterization with trichloroacetic acid was 50% (2/4), and the cumulative success rate after the second remedy was 100%. Cha et al 9 demonstrated that the success rate after the first line of treatment with chemocauterization was 77.3%, and the success rate after second treatment was 93.2%. One potential merit of trichloroacetic acid was that it could penetrate into the fistula and sealed the entire fistula channel, but it was less effective than electrocauterization in the cause of tissue inflammation and adhesion and required repeated cauterization.
Wang et al 10 reported that the success rate of CO2 laser was 55.9% (57 of 102) after 1 treatment; the cumulative success rate after 2 treatments was 85.3% (87 of 102), and the authors thought that CO2 laser cauterization was a safe effective approach with optimal patient outcomes. In addition, the combination of the 2 endoscopic methods enhanced the occlusion of the orifice in the piriform fossa and may have reduced the probability of recurrence. Lammers et al 11 successfully performed electrocauterization combined with injection of fibrin sealant for bilateral PSF.
Radiofrequency ablation technology utilizes a system of radiofrequency bipolar electrical current that passes through a medium of normal saline, which results in the production of a plasma field of sodium ions. These energized ions are able to breakdown intercellular bonds and effectively vaporize tissue at a temperature of only 60°C. This vaporization theoretically results in effective dissection with less postoperative pain from thermal injury. Zhang et al 12 first reported that the success rate of endoscopic RA after the first line of treatment for PSF was 90.3% (28 of 31) in 2015 and that complications of hoarseness occurred in 3 cases. Then, Wang et al 2 reported 106 cases of PSF that were performed by RA in the same institution in 2018, and the success rate of the procedure was 98% (104 of 106). The authors advocated using this minimally invasive technique as the first line of treatment for PSF. In our study, the success rate was 100% (18/18) after initial RA during a mean follow-up period of 21 months, which seemed higher than previous reports on endoscopic cauterization. While some patients had relatively short follow-up time, further investigation should be conducted to assess the actual effect of the procedure.
In the acute inflammation period of PSF, abscess incision and drainage could be used for treatment, but the recurrence rate of third and fourth branchial abnormalities was 94% and 89%, respectively. After 4 to 6 weeks of inflammation control, surgical intervention was the most significant way to avoid recurrence. In recent years, several reports have described endoscopic minimally invasive technology concomitant with incision and drainage for the treatment of PSF during the period of active inflammation 13 -17 (Table 4). Abbas et al 17 managed with concurrent endoscopic ablation and incision and drainage for a 12-year-old girl with a history of recurrent thyroid abscesses secondary to PSF. In our series, 4 cases presented swelling of the neck and abscess formation before the surgery, RA, and external incision and drainage of the neck abscess were performed, postoperative neck wound was irrigated with hydrogen peroxide for 1 week, and all the children recovered well. Concurrent procedures would offer clinicians a renewed approach for PSF in the acute inflammatory period, and this method could shorten the overall treatment time and alleviate the pain of the children while saving the cost of medical treatment.
Cauterization Technology Concomitant With Incision and Drainage for PSF.
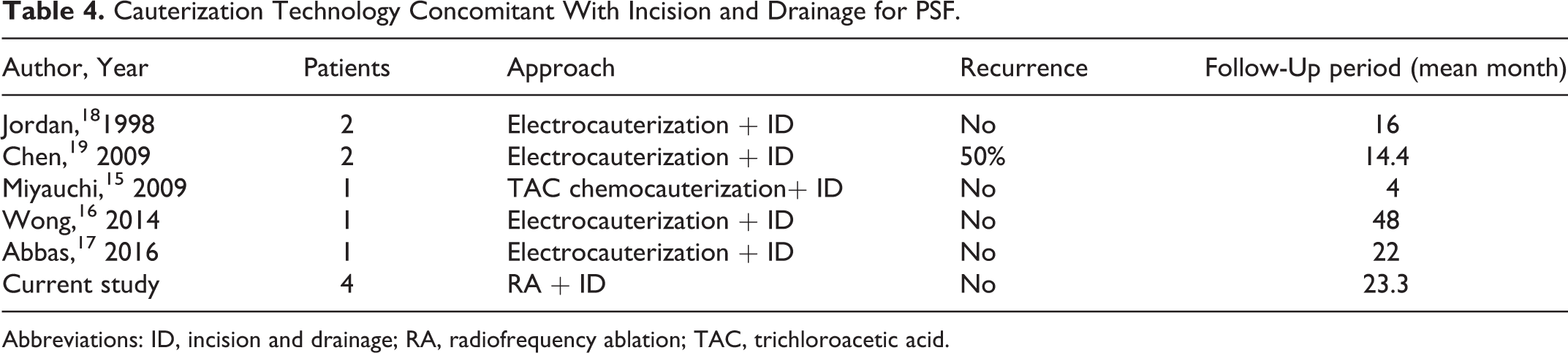
Abbreviations: ID, incision and drainage; RA, radiofrequency ablation; TAC, trichloroacetic acid.
For postoperative complications, the most common complications of endoscopic cauterization in the treatment of PSF were recurrent laryngeal nerve or superior laryngeal nerve injury, especially electrocautery and chemocauterization. Wong et al 16 reported that 3 cases of PSF were treated with electrocauterization, and 2 cases had hoarseness after the operation. Park et al 20 showed that in 2 cases, postoperative hoarseness appeared after treating by chemocauterization. Similarly, in our study, 2 children (2/18, 11.1%) developed transient hoarseness after treatment by RA and recovered after 1 month. We suspected that the branch of the laryngeal nerve in the pyriform fossa mucosa may be damaged by thermal injury. Postoperative neck swelling after minimally invasive surgery is rare in the literature, 9,14 the reason may be that although the internal opening of the PSF had closed after the coblation, the residual sinuses in the thyroid gland formed a closed lacuna (cyst), and the residual epithelium in the cyst remains continuous secretion, shedding, accumulating, and then secondary infection.
Hwang et al 18 compared open surgery with endoscopic minimally invasive surgery and reported that 27 PSF patients were treated by open surgery and endoscopic trichloroacetic acid chemocauterization, and the recurrence rates were not significantly different between the excision (5/14, 35.7%) and chemocauterization groups (6/13, 46.1%). Derks et al 19 conducted a systematic review, where the success rate after 1 treatment with cauterization ranged from 66.7% to 100% and from 77.8% to 100% after 2 treatments, and the success rate after the first-line treatment with open surgery ranged from 50% to 100% and was 100% after the second surgical attempt. The effectiveness of cauterization seemed to be comparable to surgical treatment in preventing recurrence.
In our study, the success rate and postoperative hoarseness complications between the excision and RA groups were similar. In the excision group, the advantage was that the indwelling time of gastric tube was shorter, and there was no postoperative swelling of the neck, but the disadvantages were complex procedure, long operation time, and a remaining surgical scar. For patients with extensive scarring or painless protuberant lumps on the affected side of the neck (Figure 6), external cervical approach can be used to remove the fistula and make the neck more cosmetic after the operation.

One patient showing painless protuberant lumps on the affected side of the neck.
In the RA group, this method was easier to operate, had shorter hospital days, was minimally invasive, and there were no surgical scars on the neck. However, the risk of swelling and pain in the neck may occur after surgery, and the retention time of the gastric tube was longer. For patients with initial treatment, no obvious neck scar, or skin integrity, they can give priority to RA treatment. In addition, with regard to active inflammation of PSF, RA concomitant with incision and drainage provides clinicians a renewed approach, while fistulectomy is better avoided in the presence of inflammatory lesions.
Conclusion
The curative effect of excision and RA for PSF is not significantly different; each of the 2 methods has its advantages and disadvantages. However, RA for PSF has the merit of being minimally invasive, easy to operate, and safe; this procedure seems to be more suitable in clinic.
Footnotes
Acknowledgments
Shilei Pu and Wanpeng Li contributed equally to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.