
Abstract
Tinnitus affects about 10% of population worldwide. Most patients present with some degrees of hearing impairment, while others remain normal. The aim of this study was to analyze the latency and amplitude of auditory brain stem response (ABR) waveforms in patients with unilateral tinnitus. The tinnitus ears and non-tinnitus ears were compared for each patient. Sixty-seven patients with single-sided tinnitus were enrolled, including 26 male and 41 female patients with a mean age of 54.4 (age ranged from 22 to 79). Eighteen patients had bilateral normal hearing, while 49 patients had some degree of sensorineural hearing. The ABR waveforms were retrospectively analyzed in terms of waves I, III, and V absolute latency, as well as waves I-III, waves II-V, and waves I-V latency intervals, amplitude, and amplitude ratio (III/I, V/I). Statistical analyses were performed within patients. There was no significant ABR difference between the tinnitus and non-tinnitus ears with regard to all the wave latencies and amplitudes in our patients (all P values >0.1). Our result that ABR changes were not found between tinnitus and non-tinnitus ears implies that tinnitus does not simply originate from the defect of the peripheral auditory system. It conforms to the contemporary theory that a higher level of the brain is involved in the generation of tinnitus.
Introduction
Tinnitus is a phantom perception without auditory input, which affects about 10% of the population worldwide. Tinnitus is closely related to hearing loss. 1 Most of the patients with tinnitus present with some degrees of hearing impairment. However, a number of them are without a clinical detectable hearing deficit. 1 -3 Many theories, such as “hidden hearing loss,” were proposed to explain this phenomenon.
Previously, many studies compared the auditory brain stem responses (ABRs) of patients with tinnitus and non-tinnitus individuals to find out abnormalities or lesions along the auditory pathway, which may account for the generation of tinnitus. 1 -7 However, the results are inconclusive (Table 1). One major limitation of prior studies is that they compared the ABRs of patients with tinnitus with those of normal individuals without tinnitus. An ABR recording is highly variable and dependent on variables, such as sex, age, head size, skull thickness, and so on. 2,7 Poorly matched controls will often arrive at misleading results. In order to eliminate these potential variables, we conducted within-subject comparisons of latency and amplitudes of ABR in patients with unilateral tinnitus and symmetric hearing levels. In theory, the measurable condition of tinnitus and non-tinnitus is almost identical.
Comparison of the Auditory Brain Stem Responses Between Patients With Tinnitus and Non-tinnitus Individuals.
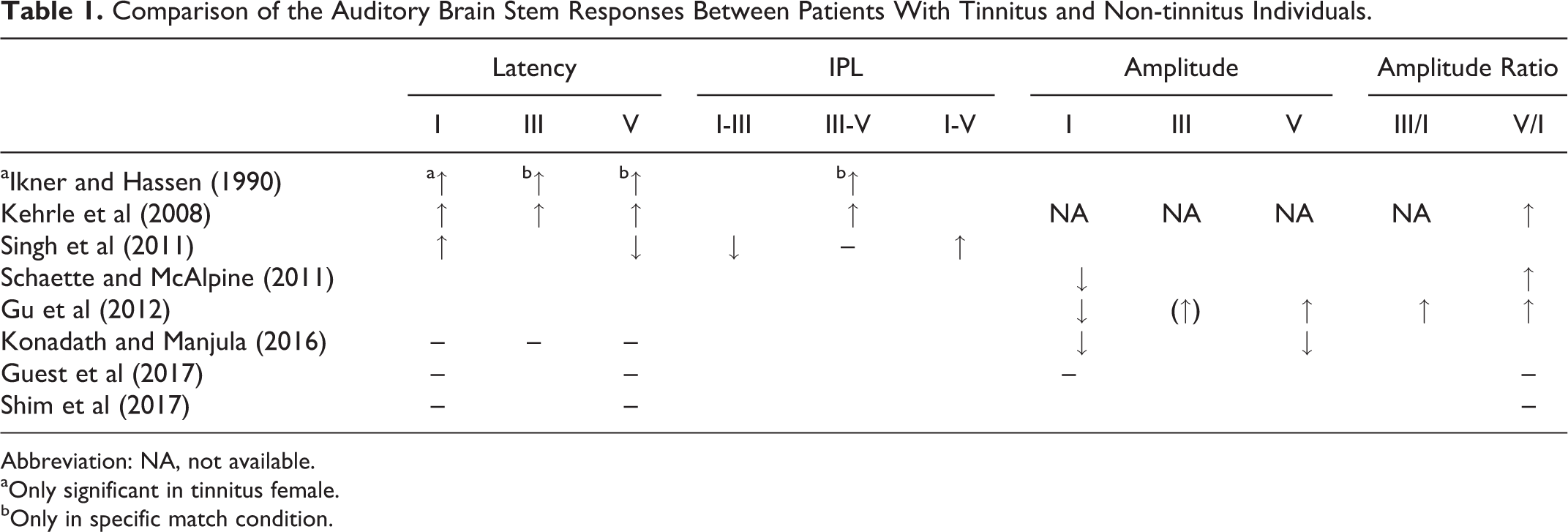
Abbreviation: NA, not available.
aOnly significant in tinnitus female.
bOnly in specific match condition.
Patients and Methods
This study is a retrospective analysis. From January 2017 to January 2018, the ABRs of 68 patients who visited our clinic with the complaint of unilateral chronic tinnitus were collected for analysis. All patients underwent pure tone audiometry (PTA; 0.25 k-8 k Hz), tympanometry, and ABR by experienced audiologists. The inclusion criteria were: (1) bilateral normal hearing and symmetric average hearing levels (defined with an average hearing level of 0.25 k-8 k Hz on PTA ≤25 dB) or bilateral symmetric mild to moderate hearing loss over high frequencies; (2) non-pulsatile unilateral tinnitus for more than 3 months, and (3) bilateral normal middle ear function. Among 68 patients, only those with abnormal ABR result received magnetic resonance imaging examination. One case of acoustic neuroma was detected and excluded from the data analysis, resulting in 67 patients eligible for analysis. We further selected those with symmetric hearing as each (PTA) threshold difference less than 15 dB as precisely matched group for sub-analysis. This study was approved by the institutional review board of our hospital.
There was no visual analogue scales (VAS) or tinnitus handicap inventory (THI) record due to the nature of chart review. As a result, the severity of tinnitus is categorized as mild (only present in quite environment, intermittent), moderate, and severe (disturbing daily life or not satisfied for previous treatment). Other-related symptoms presence of aural fullness, vertigo, and headache) and noise exposure were also analyzed.
The audiometric data of the tinnitus ear were then characterized in terms of 2 parameters: hearing level and audiogram configuration. 8,9 The classification of hearing levels was modified from American Speech-Language-Hearing Association, was calculated by a 4-tone average (0.5, 1, 2, and 4 kHz), and labeled as mild (25-40 decibel hearing level [dBHL]) or moderate (41-70 dBHL). 10 Patients with a hearing threshold >25 dBHL at any frequency, but with an average hearing level ≤25 dBHL, were also classified as mild hearing loss. The presence of any level of hearing loss was classified as “abnormal hearing.” The audiogram configurations were classified as flat or non-flat. The flat configuration was defined as the violation of hearing threshold at all frequencies was within 15 dBHL. The non-flat configuration includes those audiograms with high-tone sloping. 8,9,11
The ABR was initially used to screen the possibility of a cerebellopontine angle tumor. It was performed using diagnostic ABR (Navigator Pro; Bio-Logic Systems Corp, Mundelein, Illinois) with an 85-dB click as the stimulus (center frequency: 2 kHz) via an inserted headphone. The latency of waves I to V; interpeak latency of wave intervals I-III, III-V, and I-V; amplitude of wave intervals I-V; and amplitude ratio of waves III/I and V/I were compared within patients between tinnitus and non-tinnitus ears.
The difference of continuous parameters (ie, PTA, ABR) between the matched and non-matched ears was tested by independent sample t test. The distribution of categorical variables (ie, configuration) between the matched and non-matched ears was compared by Fisher exact test. The difference of continuous parameters (ie, PTA, ABR) between the tinnitus and non-tinnitus ears was tested by paired sample t test. The distribution of categorical variables (ie, shape) between the tinnitus and non-tinnitus ears was compared by McNemar-Bowker test. Finally, the relationship between duration of tinnitus, age, and ABR difference between tinnitus and non-tinnitus ears was tested using Pearson correlation. A 2-sided P value <.05 was considered statistically significant. No adjustment of multiple testing (multiplicity) was made in this study. Data analyses were conducted using SPSS version 25 (IBM SPSS Inc, Chicago, Illinois).
Results
Eighteen patients had bilateral normal hearing (clinically defined as all thresholds ≤25 dB), and 49 patients had abnormal hearing, that is, some degree of sensorineural hearing loss at any frequency (defined as a threshold at any frequency >25 dB). There were 26 male and 41 female ears with a mean age of 54.4 (age ranged from 22 to 79). All patients had symmetric hearing levels but had complaints of tinnitus in only one ear (32 right sides and 35 left sides). There was no significant difference of demographics between the precisely matched and non-matched study groups (Table 2). We further divided the precisely matched group by hearing level (normal and abnormal) and audiogram configuration (flat and non-flat) of the tinnitus ears, discovering that there was no difference of demographics between each sub-analysis groups (Supplemental Table 1). Table 3 shows the results of PTA and ABR of tinnitus and non-tinnitus ears. There were no significant differences between the ABR parameters except in amplitude ratio V/I; while considering the precisely matched group, all ABR parameters showed no significant difference between tinnitus and non-tinnitus ears (all P values >.1; (Table 3 and Figure 1). There was also no significant difference of ABR parameters between tinnitus and non-tinnitus ears among sub-groups of either hearing level or audiogram configuration (Supplemental Tables 2 and 3). We further tested the relationship between duration of tinnitus, age, and ABR difference between tinnitus and non-tinnitus ears. The results suggested that no correlations between duration of tinnitus, age, and ABR difference were observed (all P values >.1; Table 4).
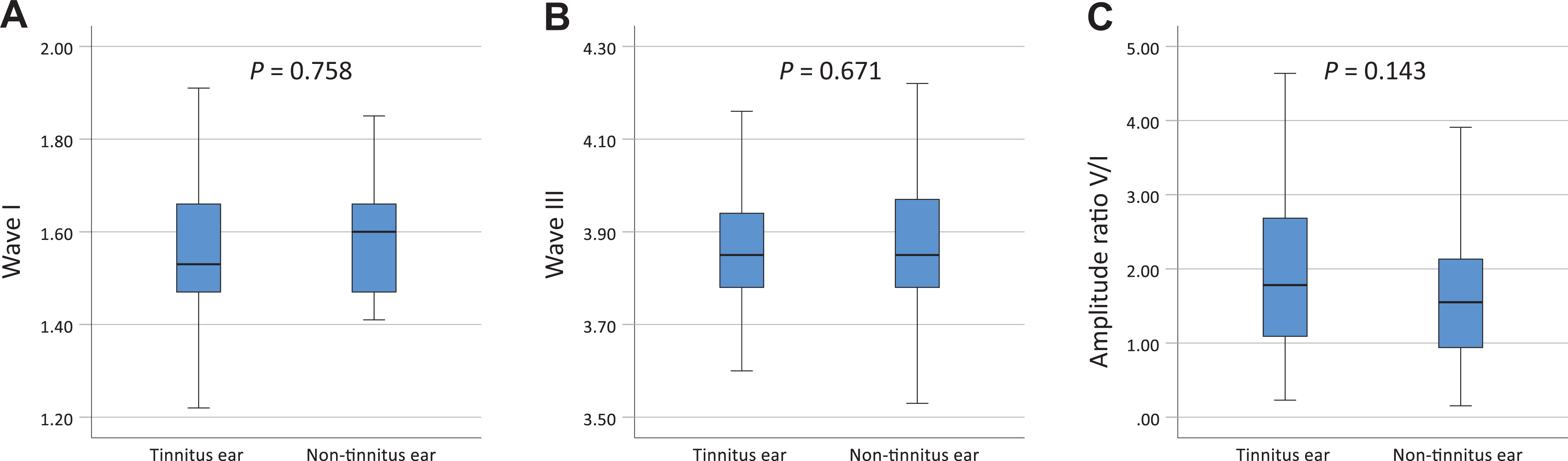
Values of wave I (A), wave III (B) and amplitude ratio V/I (C) in the tinnitus and non-tinnitus ears in the precisely matched group.
Baseline Characteristics in the Total, Precisely Matched, and Non-matched Ears.a
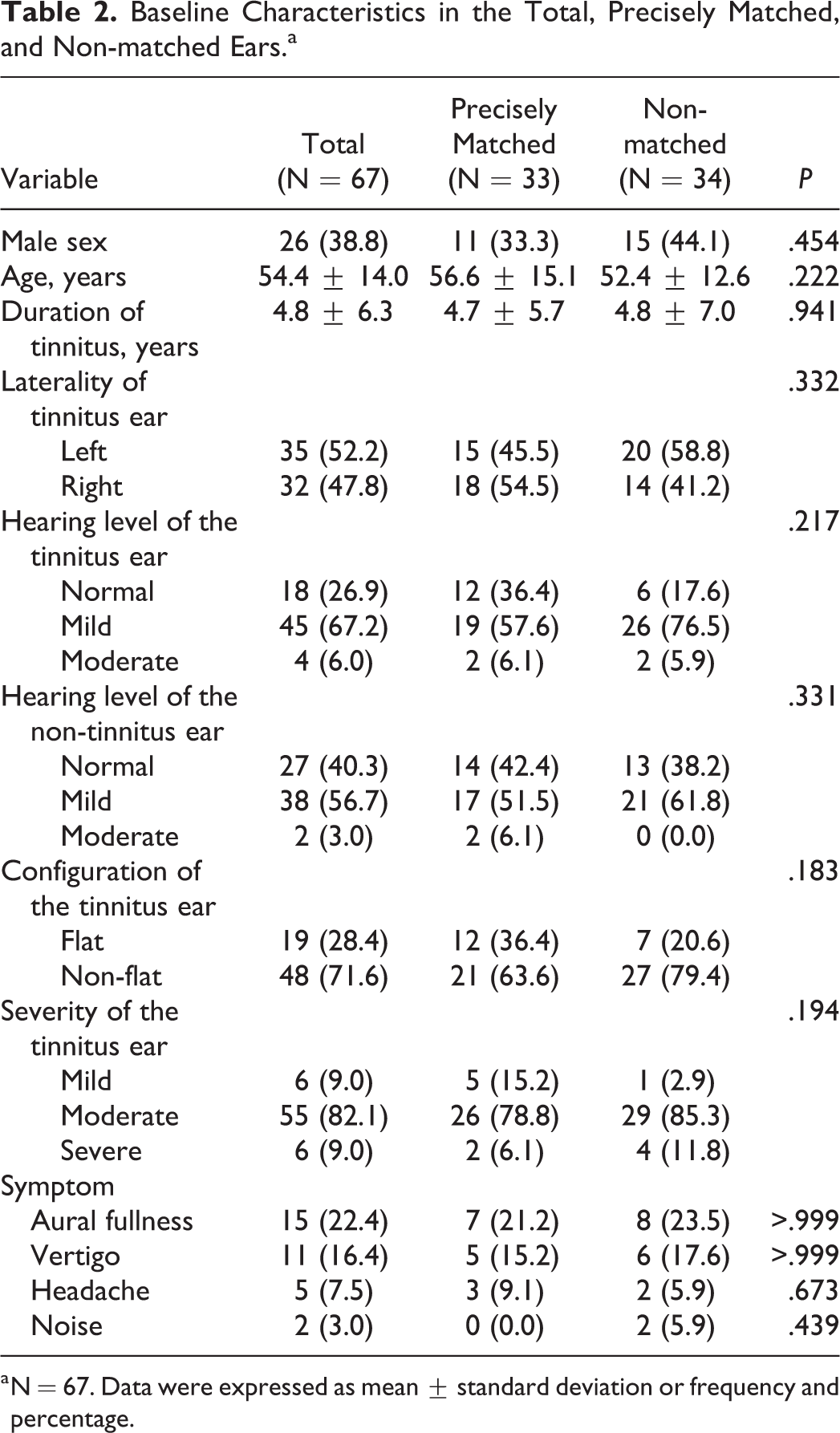
a N = 67. Data were expressed as mean ± standard deviation or frequency and percentage.
Pure Tone Audiometry and ABR Parameters in the Tinnitus and Non-tinnitus Ears.a
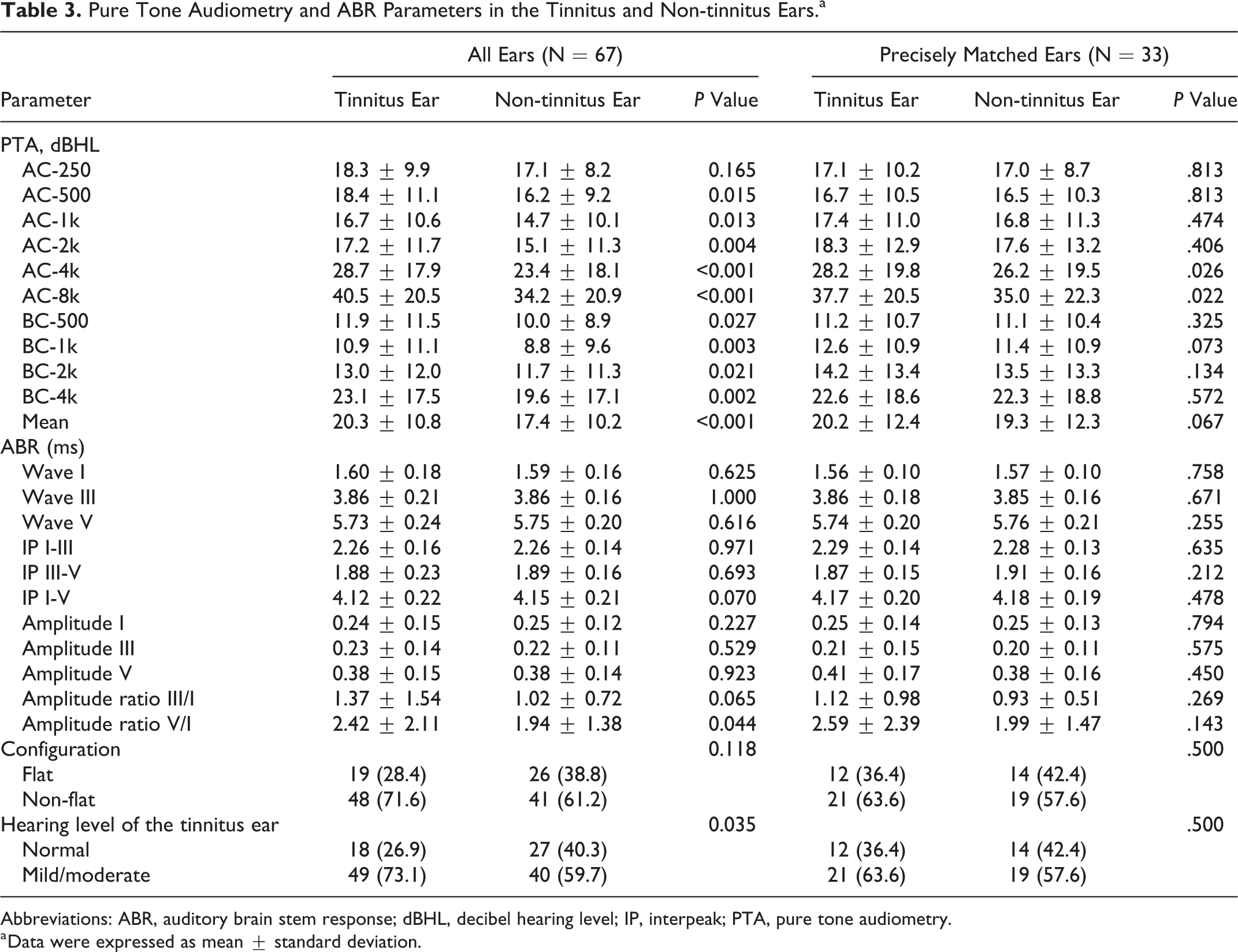
Abbreviations: ABR, auditory brain stem response; dBHL, decibel hearing level; IP, interpeak; PTA, pure tone audiometry.
a Data were expressed as mean ± standard deviation.
Relationship Between Disease Duration, Age, and ABR Difference of Tinnitus Ear Minus non-tinnitus Ear.a
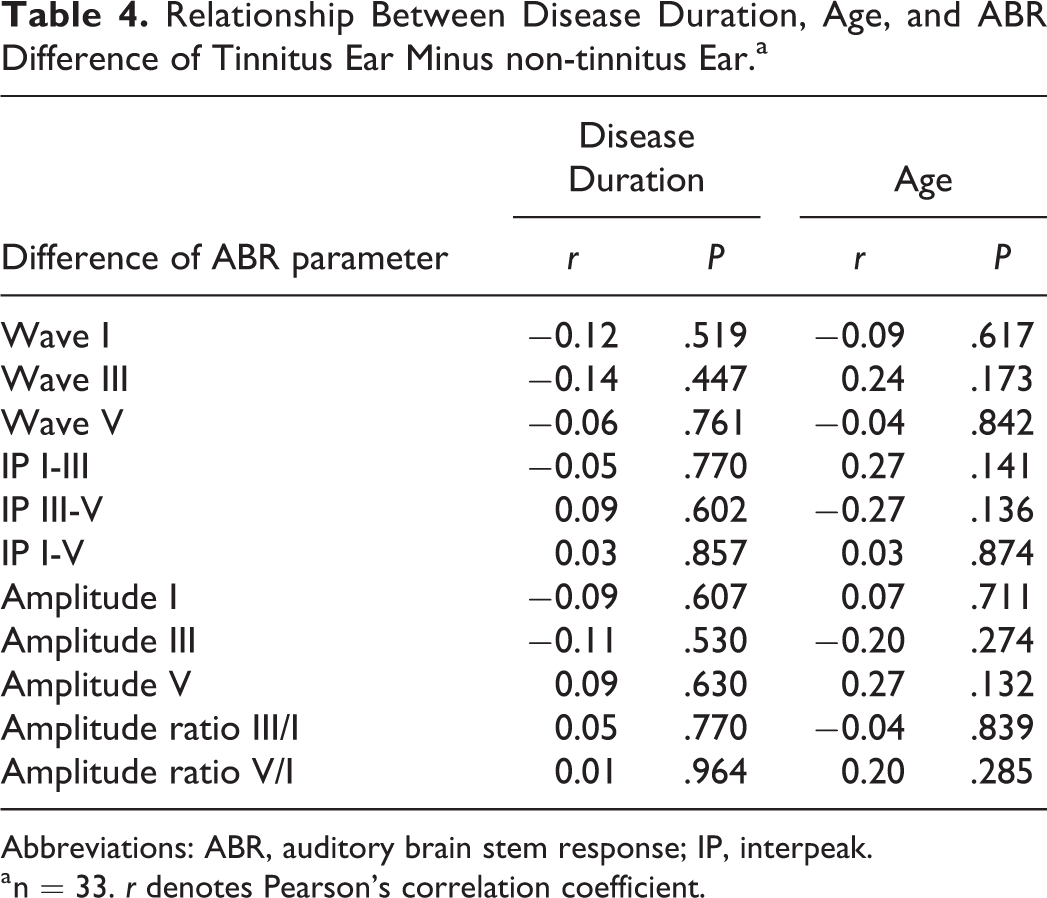
Abbreviations: ABR, auditory brain stem response; IP, interpeak.
a n = 33. r denotes Pearson’s correlation coefficient.
Discussion
Poorly matched controls will often arrive at misleading results. The ABR changes found in earlier studies may be resulted from other confounding factors but not tinnitus itself. More recent studies showed less of a difference between tinnitus and non-tinnitus ears. 1,2,12 This is probably associated with more detail and closely matched with the age, sex, and hearing threshold of each individual. Our study also confirmed that loosely and precisely matched study groups would lead to different results (Table 4). Nevertheless, even a closely matched design still inherits an individual difference between patients.
Our study does not emphasize patients having tinnitus with “normal” hearing. In fact, all thresholds below 25 dB do not stand for no defect in the auditory pathway. Selectively extended high-tone hearing loss or synaptopathy may result in damage in the auditory system without altering the hearing threshold. Instead, the essence is to compare unilateral tinnitus with the non-tinnitus ear in bilateral “symmetric hearing” patients, which suggests an almost identical measurable condition of the 2 ears, and yet patients complained of tinnitus localized to 1 ear. We did not perform an ultra-high frequency hearing measurement or a noise hearing test in this study. Although there is statistical difference between a 4-k threshold and an 8-k threshold between tinnitus and non-tinnitus ears, only a less than 5-dB difference has no clinical significance in the behavioral study. Additional, the ABR parameters were not affected by minor difference of PTA threshold and showed no statistical significance. This bias may also result from the small sample size.
Our result is similar to recent studies: There was no difference of ABR parameters between tinnitus and non-tinnitus ears. We should notice that Guest et al 2 did an inter-subjects comparison between normal hearing individuals, which inherits the risk of overlooking other environmental factors that may contribute to tinnitus. For example, history of noise or ototoxic agent exposure is not easy to recall when filling out the questionnaire. Shim et al 12 performed a within-subject comparison, but still focused on normal hearing individuals. Our data proved that a within subjected symmetric hearing comparison would reach the same result, whether the individuals had normal hearing or not.
Several articles in the literature proposed that tinnitus originated from hyperactivity of the cochlear nucleus according to animal studies. 13,14 However, the auditory pathway deficit after insult was different between species. 15 We should be careful in translating the result of animal studies to humans. In our series, the wave IIIs amplitude or latency are not different between tinnitus and non-tinnitus ears. Thus, our results in human ABR do not support their experimental results in animal studies.
There is no significant ABR difference between tinnitus and non-tinnitus ears in symmetric hearing patients in our group, implying the possibility of cortical and subcortical abnormalities that involve the generation of tinnitus. Our result may support the non-auditory gating theory, but further studies of functional evaluation is required.
The limitations of our study include a lack of the ultra-high frequency hearing measurement in the retrospective study. Thus, we cannot completely exclude hidden asymmetric hearing loss in those frequencies. Subclinical damage including retrocochlear pathology not detectable by ABR cannot be excluded as well. A prospective study in a larger population is considered for further investigation. Also, a higher center of frequency of the ABR stimuli may unveil the difference of the wave III between tinnitus and non-tinnitus ears. Further studies with different center frequencies of stimuli may discover a subtle change between the diseased and normal ears. Still another limitation of our study is the small sample size, the precisely matched group only included 33 patients. Future study should enroll more patients to achieve a better statistical analysis.
Conclusion
There is no significant ABR difference between tinnitus and non-tinnitus ears in symmetric hearing patients with or without hearing loss. The within-subject comparison diminishes possible environmental factors affecting the auditory pathway. Therefore, we concluded that, in certain patients, tinnitus is not simply originated from the defect of the peripheral auditory system. The results also confirm the contemporary viewpoints, such as the gate control theory, 16,17 that a higher level of the brain may involve in the generation of tinnitus.
Supplemental Material
Supplemental_Table_1_20191028 - Within-Subject Analysis of Auditory Brain Stem Responses in Adults With Unilateral Tinnitus
Supplemental_Table_1_20191028 for Within-Subject Analysis of Auditory Brain Stem Responses in Adults With Unilateral Tinnitus by Pey-Yu Chen and Tien-Chen Liu in Ear, Nose & Throat Journal
Supplemental Material
Supplemental_Table_2_by_configuration_20191029 - Within-Subject Analysis of Auditory Brain Stem Responses in Adults With Unilateral Tinnitus
Supplemental_Table_2_by_configuration_20191029 for Within-Subject Analysis of Auditory Brain Stem Responses in Adults With Unilateral Tinnitus by Pey-Yu Chen and Tien-Chen Liu in Ear, Nose & Throat Journal
Supplemental Material
Supplemental_Table_3_by_hearing_level_20191029 - Within-Subject Analysis of Auditory Brain Stem Responses in Adults With Unilateral Tinnitus
Supplemental_Table_3_by_hearing_level_20191029 for Within-Subject Analysis of Auditory Brain Stem Responses in Adults With Unilateral Tinnitus by Pey-Yu Chen and Tien-Chen Liu in Ear, Nose & Throat Journal
Footnotes
Authors' Note
The findings of this study were presented at the First World Tinnitus Congress and XII International Tinnitus Seminar; May 22-24, 2017; Warsaw, Poland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.