
Abstract
Objectives
To evaluate the effectiveness of sound therapy using hearing aids in patients experiencing tinnitus with acquired unilateral sensorineural hearing loss.
Methods
A total of 97 patients with unilateral tinnitus with acquired ipsilateral sensorineural hearing loss were included. Evaluation involved self-report questionnaires administered at entry, 3 months after treatment, and 1 year after treatment.
Results
The mean Tinnitus Handicap Inventory score before treatment decreased significantly (p < 0.01) at 3 months (50.0 ± 24.5-12.7 ± 16.2), and 1 year (53.3 ± 25.5-8.79 ± 13.9), after treatment. Moreover, the visual analog scale score decreased significantly at 3 months (loudness, 69.6 ± 21.9-29.1 ± 27.2; annoyance, 71.1 ± 24.7-22.7 ± 25.5) and 1 year (loudness, 69.8 ± 22.0-21.1 ± 26.1; annoyance, 72.7 ± 25.6-19.4 ± 27.6). Approximately 80-90% of patients noticed improvements in tinnitus annoyance and loudness, as determined by their responses to the questionnaires of subjective symptom improvement.
Conclusions
Hearing aids are remarkably effective for patients with unilateral tinnitus with acquired ipsilateral sensorineural hearing loss.
Introduction
Acquired unilateral sensorineural hearing loss, which is characterized as sensorineural hearing loss in one ear and preserved normal or near normal hearing in the contralateral ear, consists of several etiologies. The majority of hearing loss is sudden sensorineural hearing loss (SSNHL), with other etiologies such as Ménière’s disease. Unilateral sensorineural hearing loss is associated with a variable but often severe hearing handicap such as reduced ability to localize sounds and difficulties with discrimination in background noise. 1
In addition to the hearing handicap, a large number of patients with unilateral hearing loss experience tinnitus, which is one of the most frequent secondary symptoms. In patients with SSNHL, which is a major cause of unilateral hearing loss, Chiossoine-Kerdel et al 2 documented tinnitus in 67% of patients, with moderate to severe tinnitus handicap in 29% of patients. Other trials reported the incidence rate of tinnitus as high as 73-84% in patients with SSNHL.3-5 Similar to the hearing handicap, tinnitus in these patients has a serious impact on well-being and quality of life (QoL).2,6 Although the underlying etiology of tinnitus in patients with hearing loss is still under discussion, one hypothesis is that the reduction or shortage of auditory input changes the neural activity, which results in the perception of tinnitus.7,8 Therefore, supplementing the decrease in peripheral input using hearing instruments should be effective for tinnitus in patients with hearing loss, and it is recommended in several guidelines.9,10 Recently, several studies have investigated the effectiveness of cochlear implantation as a treatment for tinnitus in patients with single side deafness, which indeed is limited to patients with severe to profound hearing loss.11-13 However, to the best of our knowledge, no study has investigated the effectiveness of sound therapy using hearing aids in patients with unilateral hearing loss including those with mild to moderate hearing loss.
Recently, our group reported the effectiveness of hearing aids in patients with bilateral chronic tinnitus with bilateral hearing loss. 14 Furthermore, effectiveness in patients with chronic tinnitus with average hearing levels of <30 dBHL and no inconvenience due to hearing loss was also reported. 15
Therefore, our study aimed to evaluate the effectiveness of sound therapy using hearing aids in patients with unilateral tinnitus with acquired ipsilateral hearing loss.
Patients and methods
Participants
A total of 97 patients (46 men, 51 women) with unilateral tinnitus with ipsilateral acquired sensorineural hearing loss (pure tone average threshold at 0.5, 1, 2, and 4 kHz greater than 30 dB for the worse hearing ear) who visited the Department of Otolaryngology, Saiseikai Utsunomiya Hospital (Utsunomiya, Japan) between April 2007, and September 2020 were included in this study. Participants with bilateral tinnitus or contralateral tinnitus on the hearing loss side were excluded.
Diagnosis
All participants underwent a medical examination by otolaryngologists, including patient history and examination of the external and middle ear. Pure-tone audiometry was manually performed by a clinical technologist for all participants. An AA-76 or AA-H1 audiometer (Rion, Tokyo, Japan) was used for the examination. Magnetic resonance imaging (Siemens Healthineers, Erlangen, Germany) and otoacoustic emissions (Interacoustics, Middelfart, Denmark) were performed to exclude patients with retrocochlear lesion such as acoustic neuroma. Patients with other diseases that required alternative treatment were also excluded.
Treatment
First, all the participants were provided with educational counseling by an otolaryngologist and an audiologist. The counseling included the mechanism of tinnitus onset and recognition in accordance with the auditory pathway, the mechanism of tinnitus worsening in accordance with the non-auditory pathway (distress network), and the mechanism and efficacy of hearing aids against tinnitus. 14
Sound therapy using a hearing aid was initiated after the counseling, at least 6 months following the onset of hearing loss. Hearing aids were provided only for the worse ear in all participants. All hearing aids used were digital and were fitted by audiologists at our department with a specific fitting procedure in Japan, as described in our previous studies.14,15 The gain was verified by the functional gain calculated from the aided and unaided soundfield thresholds. Hearing aid output sound level was also measured using the HA1-2cc coupler. At all frequencies, the compression ratio was set from 1:1.3 to 1:1.7. The final target gains of 0.5, 1, and 2 kHz were set to half gain, and gains of 0.25 kHz and 4 kHz were set so that they would gradually decrease (approximately 5 dBHL) relative to the previous three gains on the aided hearing threshold. 14 None of the patients used other hearing instruments such as sound generators.
During the first 3 months, patients were examined weekly or biweekly. At each examination, a hearing aid fitting was performed. We started from 70% of the target gain and gradually increased the gain of the hearing aid (1-3 dBSPL per visit) so that the gain would reach the target gain at 3 months after the start. Thereafter, the examination was performed every 3 months. Medical examination and condition check of the hearing aid were conducted at each visit.
Evaluation of treatment efficacy
The tinnitus evaluation consisted of three questionnaires: the Japanese version of the Tinnitus Handicap Inventory (THI), 16 the visual analog scale (VAS) for loudness and annoyance, and questionnaires on subjective symptom improvement for tinnitus loudness and annoyance. The THI is a 25-item questionnaire designed to assess the patient’s perceived handicap attributed to their tinnitus. The response options for each item comprise three levels: yes (4 points), sometimes (2 points), and no (0 point). The points are added together, and the total THI score is computed. The range of the total THI score is 0 to 100, with a higher score indicating a greater handicap. The severity grade is categorized by the total score as following: no handicap (0-16), mild handicap (18-36), moderate handicap (38-56), and severe handicap (58-100). Additionally, reduction of 20 points or more is considered clinically significant change. The VAS is a questionnaire to assess the participants’ subjective tinnitus loudness and annoyance by placing a mark on a horizontal 100-mm line. On the left end of the line, “No tinnitus present” was stated, and on the right end was “The worst tinnitus you can feel.” The VAS score was acquired by measuring (in mm) the distance from the left end of the line to the point marked by the participant. The range of the VAS score is also 0-100, with a higher score indicating a greater loudness or annoyance. For the subjective symptom improvement questionnaire, the participants rated the degree of changes in tinnitus loudness and annoyance according to five categories: “worse,” “no change,” “slightly improved,” “much improved,” and “almost disappeared.”
The questionnaire data were obtained at the start of the treatment, at 3 months after treatment, and 1 year after treatment.
Statistical analysis
Data were analyzed using SPSS version 26 (IBM, Armonk, NY). For each questionnaire, the scores at entry and those obtained 3 months following the initiation of treatment were compared using the paired t-test. Analysis of variance was performed with post-hoc Bonferroni test for the comparison of the scores at entry and those obtained at 3 months and 1 year. The significance level was set at a p-value of < 0.05.
Ethics approval
This study was approved by the Ethics Committee of the Saiseikai Utsunomiya Hospital (approval number: 2020-19, date: June 5, 2020). Procedures and information collection from the patients’ medical records were performed in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans. Written informed consent was obtained from all study participants.
Results
Participants’ characteristics
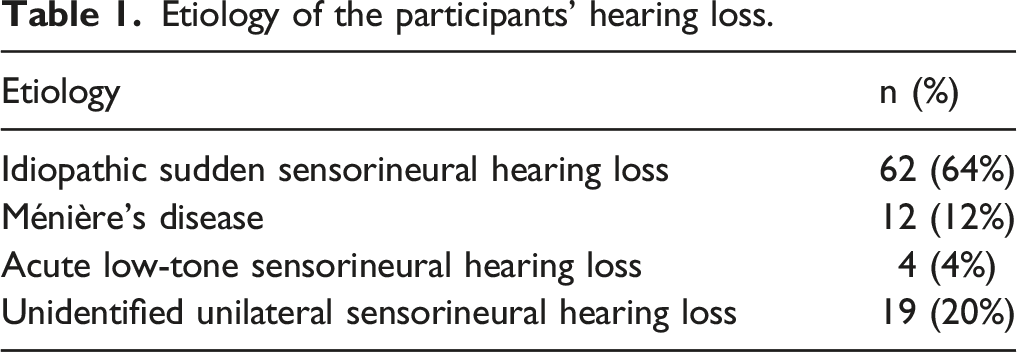
Etiology of the participants’ hearing loss.
Mean pure tone thresholds (air conduction) of the participants.

Mean ± SD (dB).
Degree of hearing loss of the participants.
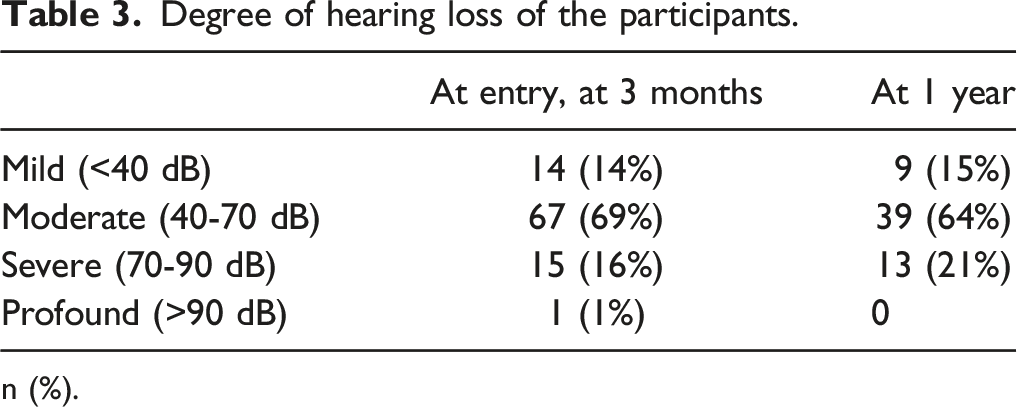
n (%).
Severity grade of tinnitus of the participants at entry.
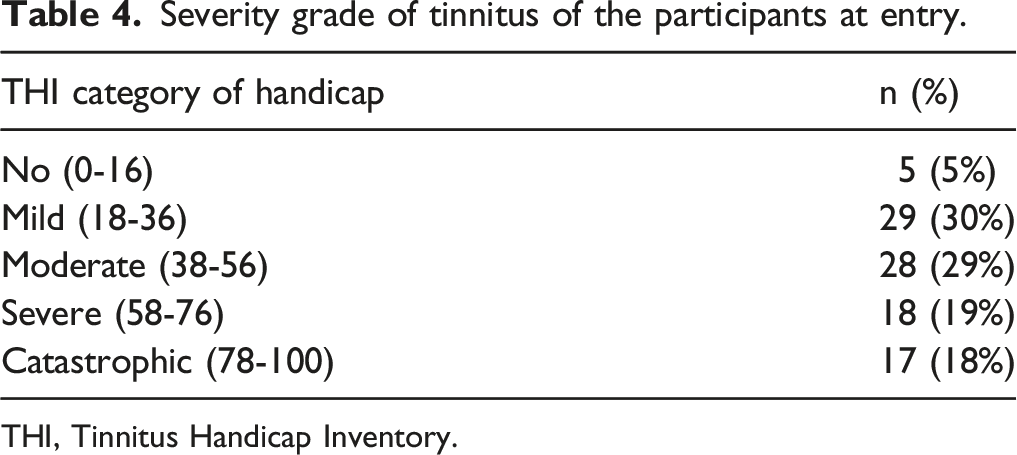
THI, Tinnitus Handicap Inventory.
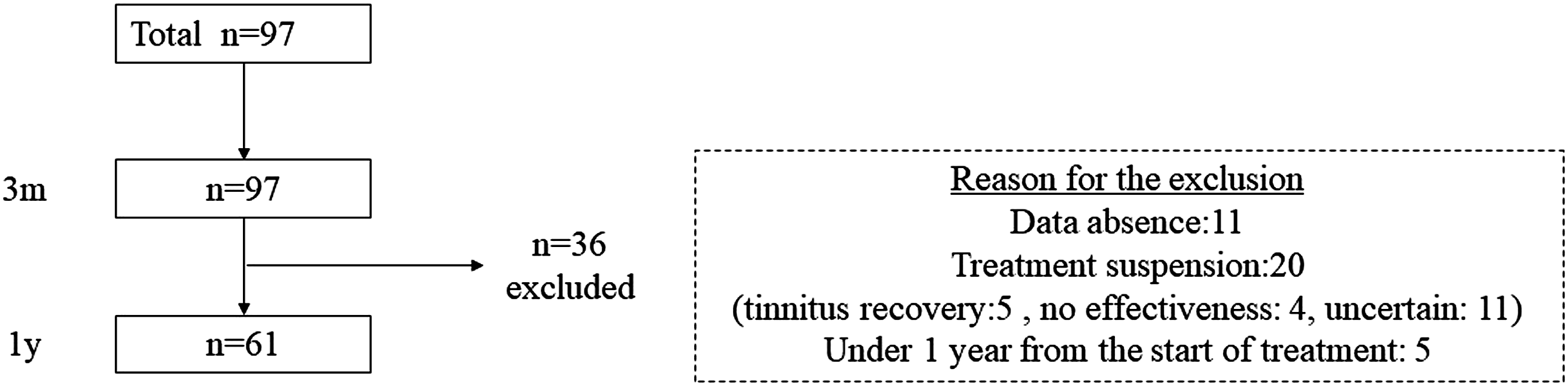
Flow diagram of the study process. Thirty-six participants were excluded from the analysis at 1 year.
Tinnitus handicap inventory
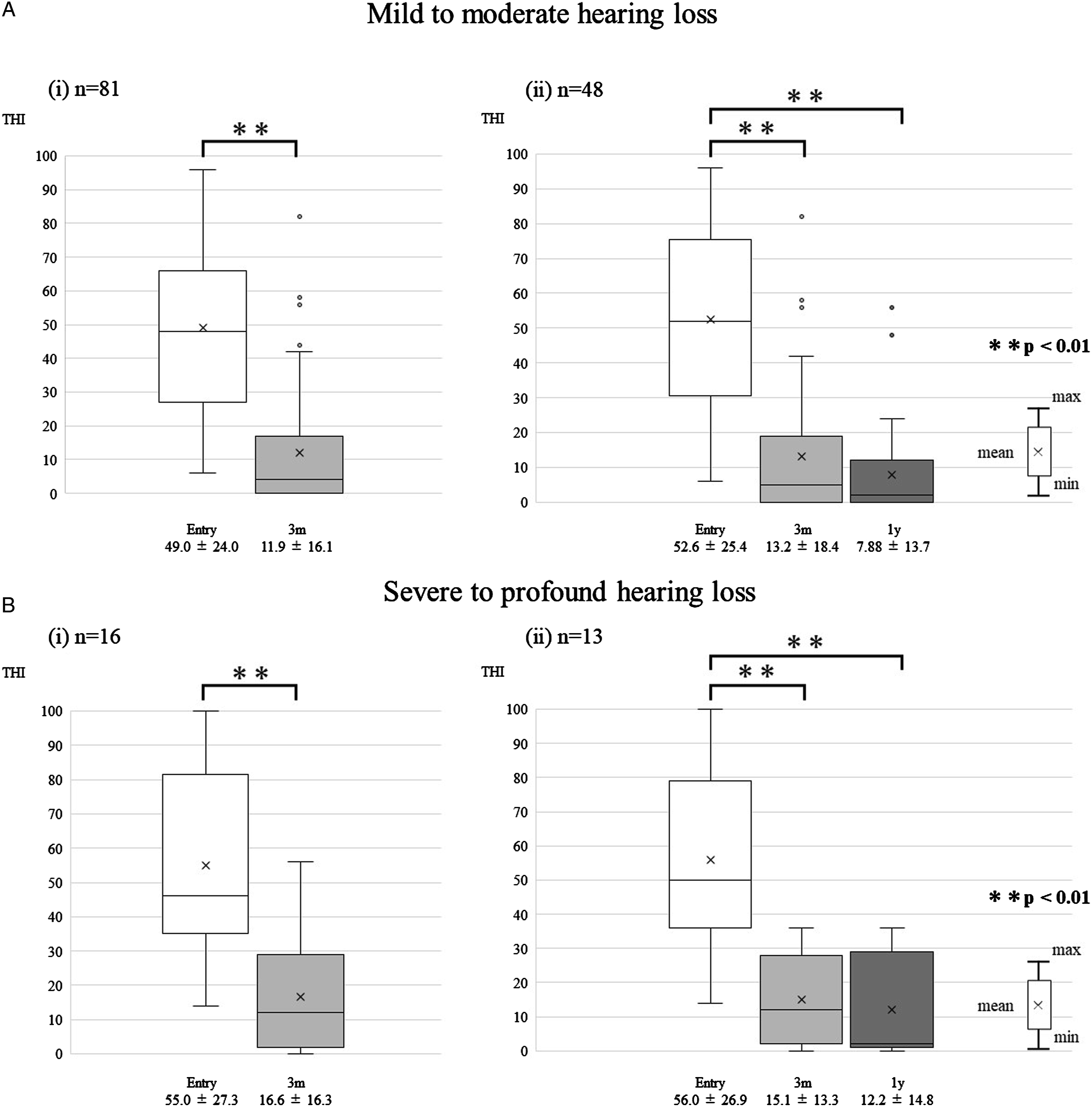
Figure 2 shows the THI scores of the participants. Significant reduction was found when comparing the THI score at treatment initiation (50.0 ± 24.5) with the THI score following 3 months from the start of treatment (12.7 ± 16.2) (p < 0.01). In the 1-year analysis, the THI score (8.79 ± 13.9) remained significantly lower than that at treatment initiation (53.3 ± 25.5) (p < 0.01) with no significant difference with that at the following 3 months (13.6 ± 17.3) (p > 0.05). A total of 78.0% of the participants at 3 months and 88.5% at 1 year demonstrated a clinically meaningful improvement compared with that at treatment initiation. The results according to the degree of hearing loss are presented in Figure 3. Despite the degree of hearing loss, the THI score decreased significantly at the following 3 months and 1 year than at treatment initiation (p < 0.01). Furthermore, there was no evident difference in the results according to etiology. The Tinnitus Handicap Inventory score before and after treatment. The THI score decreased significantly both at 3 months (A) and at 1 year (B) after treatment initiation **p < 0.01. The Tinnitus Handicap Inventory score of the participants according to the degree of hearing loss (A: mild to moderate, B: severe to profound). Despite the degree of hearing loss, the THI score decreased significantly both at 3 months and 1 year after treatment initiation **p < 0.01.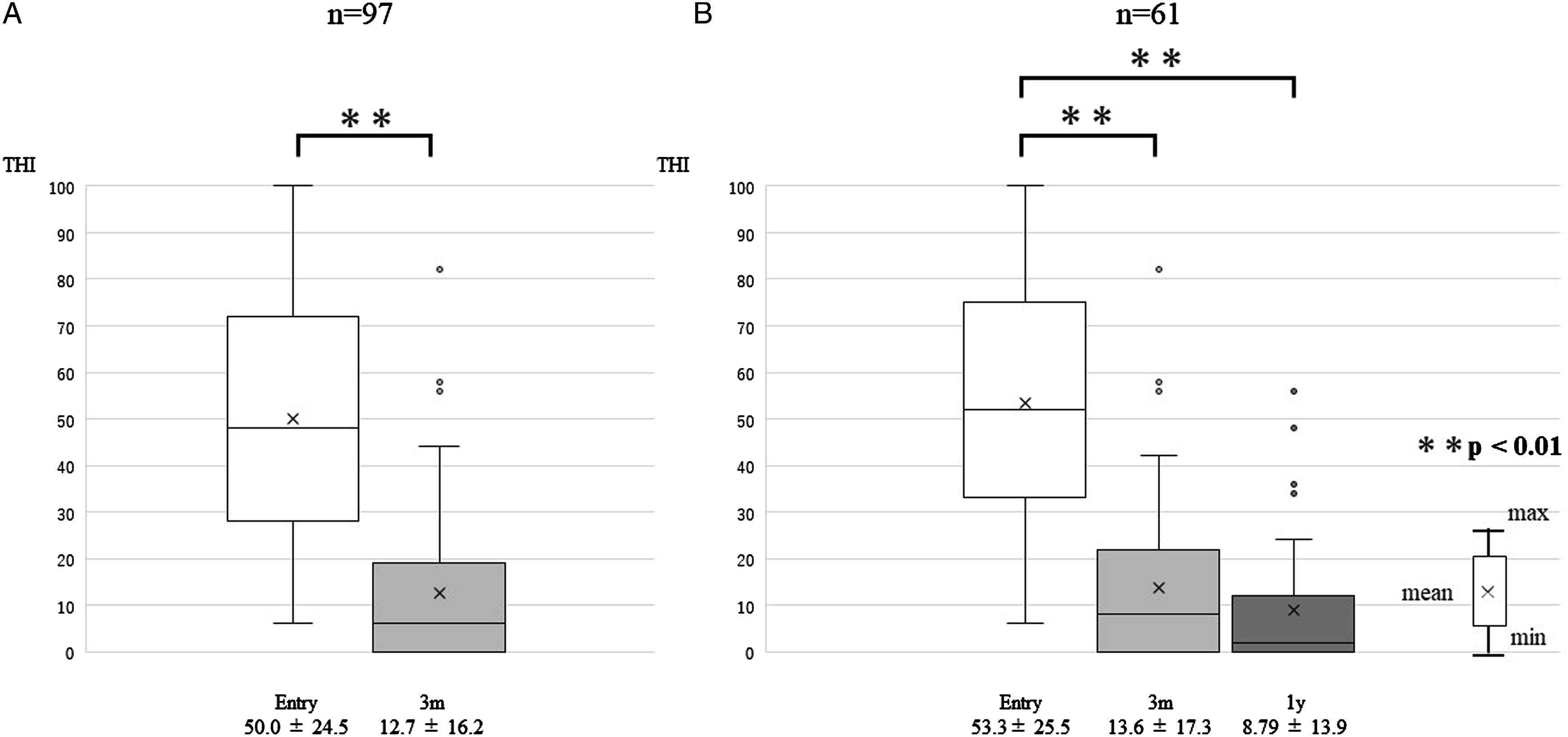
Visual analog scale score
Figure 4 shows the VAS scores for tinnitus loudness and annoyance of the participants. Significant reduction was observed when comparing the VAS score for tinnitus loudness at treatment initiation (69.6 ± 21.9) with the score at 3 months after treatment initiation (29.1 ± 27.2) (p < 0.01). In the 1-year analysis, the score (21.1 ± 26.1) remained significantly lower than that at treatment initiation (69.8 ± 22.0) (p < 0.01). Similarly, the VAS score for tinnitus annoyance decreased significantly at 3 months (71.1 ± 24.7-22.7 ± 25.5) (p < 0.01) and 1 year (72.7 ± 25.6-19.4 ± 27.6) (p < 0.01) after treatment initiation. The visual analog scale (VAS) score for tinnitus loudness (A) and annoyance (B) before and after treatment. The VAS score decreased significantly both at 3 months and at 1 year after treatment initiation **p < 0.01.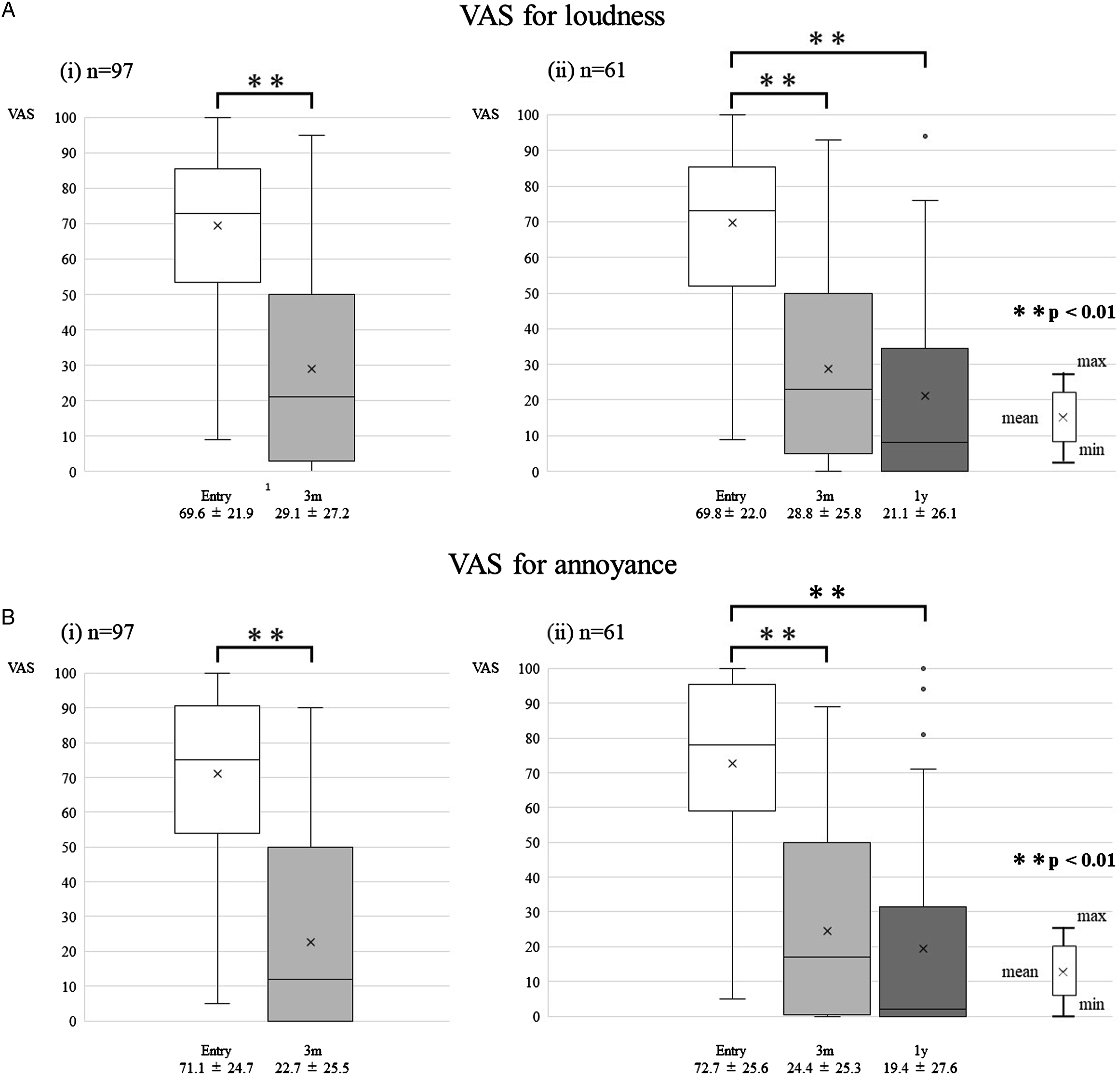
Questionnaires on subjective symptom improvement
Figure 5 shows the results of the questionnaires on the subjective symptom improvement. In total, 86% of patients rated improvement in loudness as “slightly improved” or higher at 3 months and 87% at 1 year; 91% patients rated improvement in annoyance at 3 months and 93% at 1 year. For loudness and annoyance, no patients rated “worse” at 3 months and 1 year after treatment initiation. Results of the subjective symptom improvement questionnaire for tinnitus loudness (A) and annoyance (B). The percentage of patients who rated “slightly improved” or higher were 86% at 3 months and 87% at 1 year for loudness. For annoyance, the percentage was 91% at 3 months and 93% at 1 year.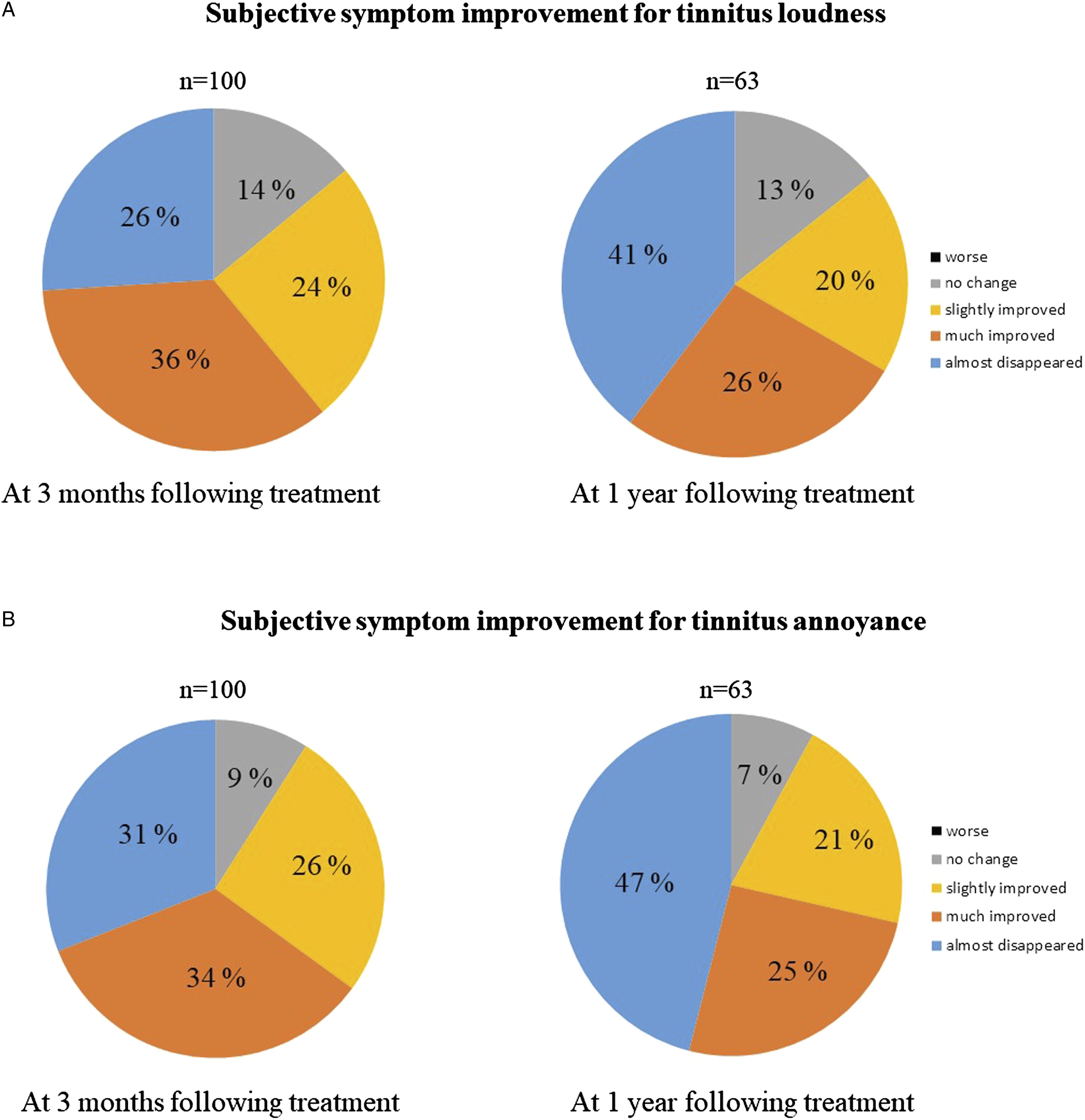
Discussion
The results of the current study showed remarkable and longitudinal effect of sound therapy using hearing aids for unilateral tinnitus in patients with acquired ipsilateral sensorineural hearing loss.
While the underlying etiology of tinnitus remains controversial, we consider the mechanism of tinnitus recognition and worsening to be divided into the auditory and non-auditory pathways, which are neurologically synchronized. 14 The onset of tinnitus via the auditory pathway is triggered by reduction in the peripheral input owing to hearing loss and subsequent compensatory activation in the auditory center.7,8,17 Hearing aids are effective in inputting sound in the frequency range, in which the peripheral input was decreased, and directly suppressing the increase in auditory center activity. Sound generators are often used in the treatment of tinnitus, such as tinnitus retraining therapy. However, for directly inputting sound in only the necessary frequency range, hearing aids are desirable, especially for patients with functional hearing in the affected ear and those whose hearing threshold differs by frequency.
Comparison of the current study with previous studies.
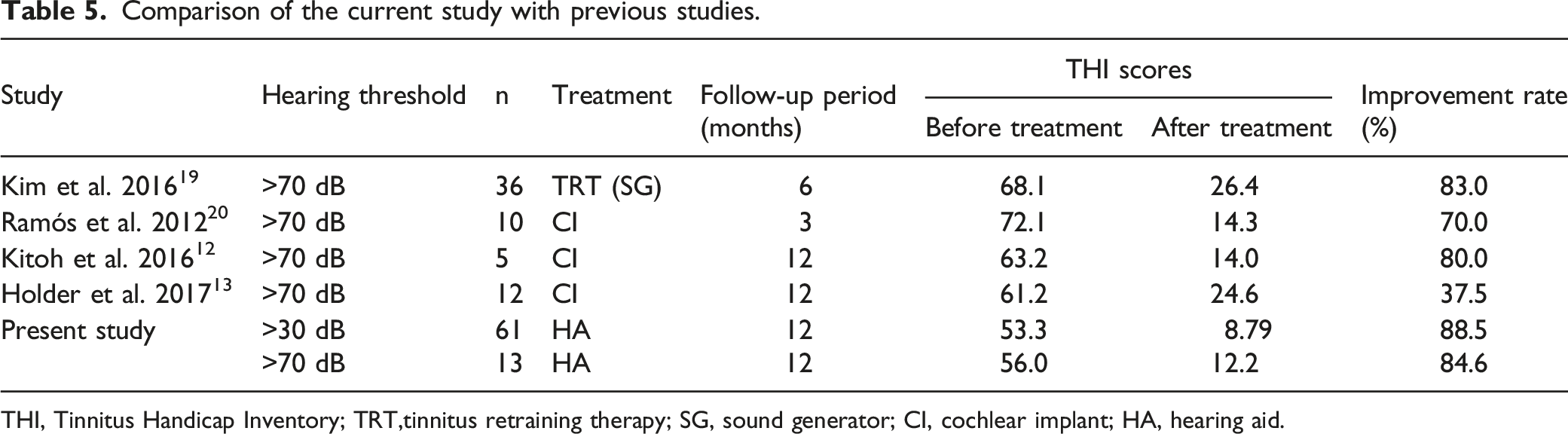
THI, Tinnitus Handicap Inventory; TRT,tinnitus retraining therapy; SG, sound generator; CI, cochlear implant; HA, hearing aid.
There are several limitations to the current study. First, there was a large degree of heterogeneity among the participants. For example, there was great variation in the degree of hearing loss. Although we have conducted the analysis categorizing the degree of hearing loss (mild to moderate/severe to profound), the sample size, especially of participants with severe to profound hearing loss, was small. Furthermore, the etiology of the participants’ hearing loss varied extensively. The annual changes in tinnitus severity would be different among etiologies, especially for those with high recurrence rate such as patients with Ménière’s disease. Future studies including analysis with the stratification of the hearing level and etiology are warranted. Second, the study did not include a control group. We consider educational counseling to be necessary for effective sound therapy using hearing aids. However, it remains unclear whether the effects seen in this study are due to both of these factors or only one of them. Additionally, the possibility that tinnitus simply recovered naturally in the course of time cannot be ruled out. For higher evidence levels, randomized studies with comparison with a control group and a group receiving only educational counseling are required. This limitation is referred to in other studies including clinical guidelines.9,15,18
Conclusion
The results of the present study demonstrate that sound therapy using hearing aids is remarkably effective for patients with unilateral tinnitus with acquired ipsilateral sensorineural hearing loss.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.