
Abstract
The immune pathogenesis of chronic rhinosinusitis with nasal polyps (CRSwNP) remains obscure. Our aim was to compare humoral immunity and white blood cell counts in patients with CRSwNP and controls. A prospective case–control study was carried out in 37 patients with CRSwNP and 34 controls without CRS. Clinical data were gathered through a systematic interview. Computed tomography scan, skin prick test, spirometry, and immunological parameters (leukocyte differential count, immunoglobulin classes, and immunoglobulin [Ig] G subclasses) in serum specimens were obtained. Statistical analysis was performed using SPSS v.23. The prevalence of chronic lower respiratory diseases was greater in the CRSwNP group (P < .001), but atopic disease had no significant difference. A significantly higher eosinophil (P < .001) and basophil relative count (P = .022) and a lower relative neutrophil count (P = .013) were found among CRSwNP group. Patients with CRSwNP had higher IgG1 (P = .022), but lower IgG2 (P = .014) and IgG3 (P = .018) serum levels compared to controls; IgG4, total IgG, IgA, IgM, and IgE serum levels did not differ between groups, as well as the prevalence of immunoglobulin classes or IgG subclasses deficiency. The variation observed in peripheral relative leukocyte count and the systemic IgG1 subclass shift are similar to what is known to happen in nasal polyp tissue. A unique systemic immune profile seems to be present in patients with CRSwNP.
Introduction
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a common clinical entity, but despite the high prevalence, morbidity, and chronicity, its etiopathogeny remains obscure. 1 Systemic immunological changes associated with CRSwNP may provide important clues to a better knowledge of the involved immune pathways.
Local immune modifications in nasal mucosa have been intensely investigated in CRSwNP. It is known that Western patients with CRSwNP show local tissue immune effects, such as skewing of the inflammatory response in a T helper cell type 2 direction, generation of local polyclonal immunoglobulin E (IgE) antibodies, promotion of eosinophil survival, and mast cell degranulation. 1 In polyps homogenates, it has already been demonstrated significantly higher values of immunoglobulin A (IgA), immunoglobulin G (IgG) and IgE, as well as a higher percentage of IgG class 1 (IgG1), when compared to nasal tissue samples from controls. 2 An immunofluorescent study in nasal polyps from 100 patients has shown a positive labeling for IgG in all specimens, for C3b complement fraction in 80% but negative immunofluorescency for immunoglobulin M (IgM) or IgA. 3
However, data about systemic modification of immune system in CRSwNP are scarce, namely about immunoglobulin classes and subclasses. To our knowledge, the only controlled study to address IgG subclasses serum modifications in CRSwNP included 15 patients and 10 controls, not finding any significant difference. 2
Our main goal was to characterize systemic immunological alterations that occur in patients with CRSwNP compared to controls, namely in leukocyte differential count and humoral immune profile, based on immunoglobulin classes and subclasses dosage.
Materials and Methods
A prospective and observational case–control study was performed according to the established ethical guidelines and approval of Ethics Committee at the Cova da Beira Hospital Centre (deliberation number 82/2015). A signed informed consent was obtained from each participant in the study.
Sample
All the cases were about to undergo endoscopic sinus surgery for CRSwNP refractory to medical treatment (topical long-term and systemic short-term steroids), in a district hospital center, from January 2016 to October 2018. Diagnosis of CRSwNP was established using the definition of EPOS 2012. 1 The cases were selected consecutively from the waiting list and had their disease confirmed endoscopically, by computed tomography (CT) and histological examination of the subsequent surgical specimen. Patients were selected after applying the following exclusion criteria: concomitant benign or malignant sinonasal tumors, chronic rhinosinusitis without nasal polyps (CRSsNP), antrochoanal polyps, polyps associated with fungal rhinosinusitis, primary ciliary dysfunction, cystic fibrosis, acquired immunodeficiency (ie, human immunodeficiency virus; immunosuppressive drugs), autoimmune diseases (eg, systemic vasculitis), or history of or under allergen-specific immunotherapy. No course of systemic corticosteroids was given to patients with CRSwNP at least 3 months before serum specimens collection, and inhalant steroids were only prescribed if needed for asthma control and in combination with long-acting B2-agonists.
Controls were selected from patients in the waiting list for septoplasty, after excluding patients with symptoms and endoscopic or CT signs of chronic rhinosinusitis (CRS), with acquired immunodeficiency, autoimmune diseases, or with history of or under allergen-specific immunotherapy. All the cases and controls were adults (older than 18 years).
Data Collection
Clinical data were gathered through a systematic interview to collect information on demographics, occupational history, and comorbidities. Subjective assessment of upper and lower respiratory disease was obtained through Rhinosinusitis Quality of life survey—Portuguese version (RhinoQOL-pv) 4 and chronic obstructive pulmonary disease (COPD) assessment test (CAT). 5 The CAT test was chosen because it consists of nonspecific questions about lung disease impacts and has already been studied not only for COPD, but also for Asthma. 6 Nasal polyps were classified endoscopically according to Lund criteria, and Lund-Mackay imagiological score was obtained for each participant. These clinical, endoscopic and imagiological evaluations were done 3 months before surgery.
All patients and controls were submitted to skin prick test, while specific serum IgE antibodies for inhalants were requested as needed. Participants also performed a spirometry test, which is considered an essential assessment of patients with suspected chronic lower respiratory diseases (CLRD). 7 In case of abnormal test result or if patients presented lower respiratory symptoms, the participant was further evaluated by a respiratory physician and subsequent examinations were demanded as needed in order to establish a final diagnosis (eg, bronchial challenge, day-to-day peak expiratory flow variation, imagiological examination). Chronic lower respiratory diseases were classified according to International Classification of Diseases, 10th Revision. 8 Patients with CRSwNP were also subdivided into CRSwNP with CLRD and CRSwNP without CLRD for data analysis. It was decided to classify according to the presence of CLRD and not only asthma, since there is growing evidence for the coexistence of CRS and CLRD other than asthma (eg, COPD). 9 -12
Blood sample was collected to obtain a leukogram, to determine the levels of immunoglobulin classes and IgG subclasses. Laboratory testing was performed 2 weeks before surgery at the same time of preoperative workout. Total white blood cell (WBC) count and 5-part leukocyte differentiation were determined automatically using DxH 800 (Beckman Coulter). The results of differential counts were presented and compared in relative numbers as traditionally done and currently performed in the literature (evidence exists that relative numbers are more accurate than absolute leukocyte differential counts 13 ). Immunoglobulin classes were obtained by immunoturbidity assay using Cobas 6000 analyzer (RocheDiagnostics®, Mannheim, Germany) and levels of immunoglobulin subclasses were obtained through the Optilite turbidimetric analyser (The Binding Site®, Birmingham, United Kingdom). The reference range used for total IgG (700-1600 mg/dL), IgA (70-400 mg/dL), and IgM (40-230) was the one suggested by the International Federation of Clinical Chemistry. 14 Levels of immunoglobulin subclasses were considered to be low if IgG1 <405 mg/dL, IgG2 <169 mg/dL, IgG3 <11 mg/dL, or IgG4 <3 mg/dL according to the laboratory reference values.
Statistical Analysis
Statistical analysis was performed with Statistical Package for Social Sciences (IBM SPSS Statistics for Windows, Version 23.0). Descriptive statistics was used in sample characterization. Nonparametric tests were used for continuous variables since our data did not meet the assumptions needed for parametric tests, namely normal distribution of the dependent variable in each group and homogeneity of variances. Mann-Whitney test was used to compare continuous variables between CRSwNP and controls. A subanalysis with Kruskal-Wallis test was performed to compare continuous variables between 3 groups (control group without CLRD, CRSwNP without CLRD, and CRSwNP with CLRD), and Dunn post hoc test was carried out for multiple pairwise comparisons. Chi-square test (or Fisher exact test/likelihood ratio test when needed) was used to test association between categorical data. A P value <.05 was considered as statistically significant.
Results
Seventy-one individuals completed the study: 37 patients with CRSwNP and 34 controls. Demographics, comorbidities, and occupational dust exposure of CRSwNP and controls are presented and compared in Table 1. All participants were Caucasians.
Characterization of Sample Demographics, Comorbidities, and Occupational Dust Exposure.a
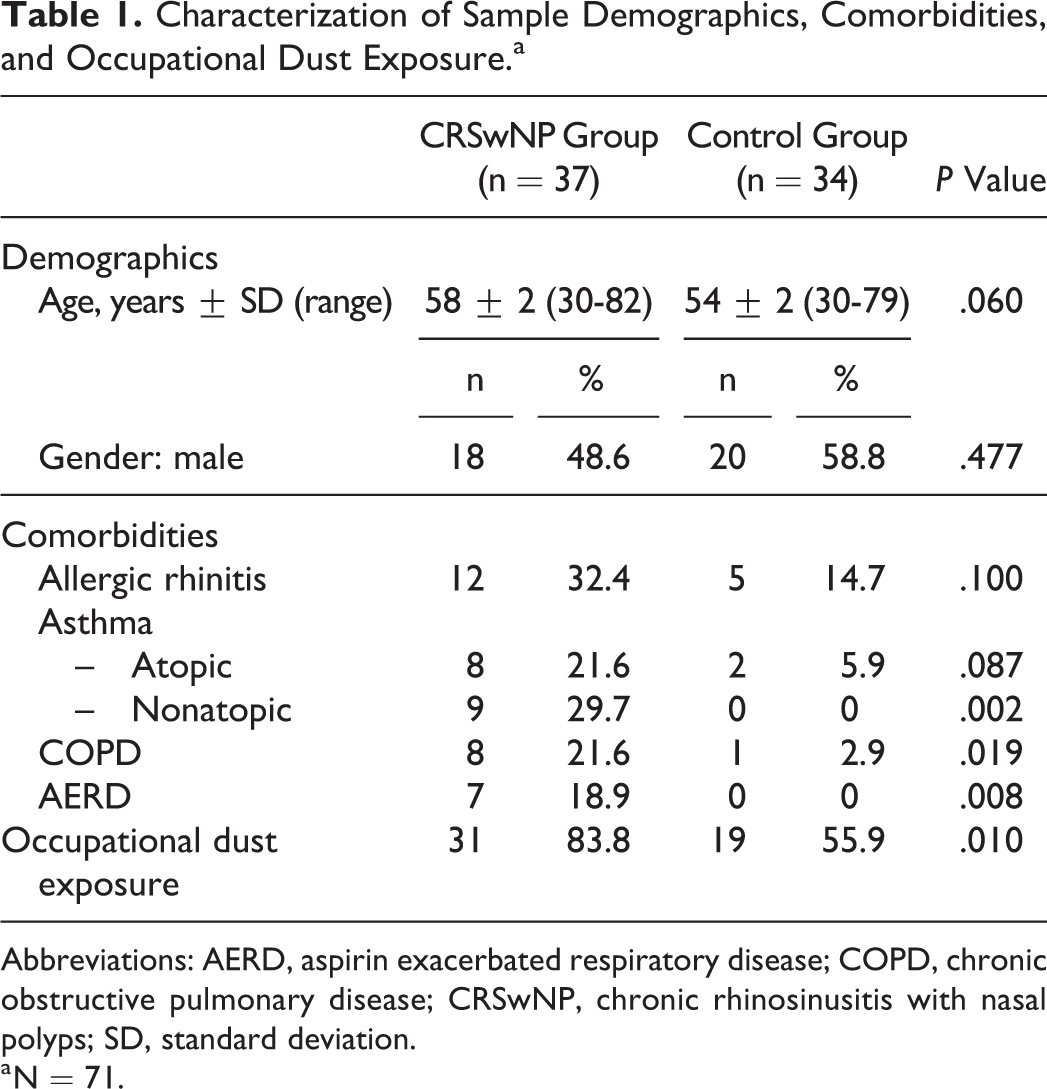
Abbreviations: AERD, aspirin exacerbated respiratory disease; COPD, chronic obstructive pulmonary disease; CRSwNP, chronic rhinosinusitis with nasal polyps; SD, standard deviation.
a N = 71.
RhinoQOL-pv and CAT total mean scores were significantly higher among the CRSwNP group (60.4 ± 3.5 and 15.9 ± 1.7, respectively) versus the mean values for the control group (49.3 ± 2.7 and 7.3 ± 1.2; P = .010 for RhinoQOL-pv and P = 1 × 10−4 for CAT, Mann-Whitney test).
Twenty-five (67.6%) patients with CRSwNP presented concomitant CLRD (Table 1) which, compared with the control group (3 individuals, 8.8%), means a higher prevalence of pulmonary diseases (P = 0.17 × 10−7, Fisher exact test). Aspirin exacerbated respiratory disease (AERD) was more prevalent among CRSwNP group (Table 1), with 16.2% of CRSwNP presenting the Samter’s triad (6 cases). In CRSwNP group, 21 (56.7%) of 37 were under treatment with inhaled steroids with β2-agonists; whereas in the control group, only 1 patient was being treated with inhaled steroids.
Twelve (32.4%) individuals from the 37 patients with CRSwNP and 5 (14.7%) individuals from the control group had atopic disease, without a statistically significant difference (P = .100, Fisher exact test).
Nasal polyps were classified endoscopically as grade I in 5 (13.5%) cases, grade II in 11 (29.7%) cases, and grade III in 21 (56.8%) cases, according to Lund criteria, and the mean Lund-Mackay imagiological score was 15.22 ± 0.78. All nasal specimens of patients with CRSwNP showed tissue eosinophilia (>10/hpf).
The analyzed systemic immunological parameters are presented and compared in Table 2. In respect to leukogram, patients with CRSwNP had significant lower levels of relative neutrophil count but higher values of relative eosinophil and basophil counts. Concerning humoral immunity, CRSwNP showed an IgG1 subclass switching, with reduced levels of IgG2 and IgG3. No significant differences were observed for total IgG, IgA, IgM, and IgE serum levels.
Comparison of Systemic Immunological Parameters.a
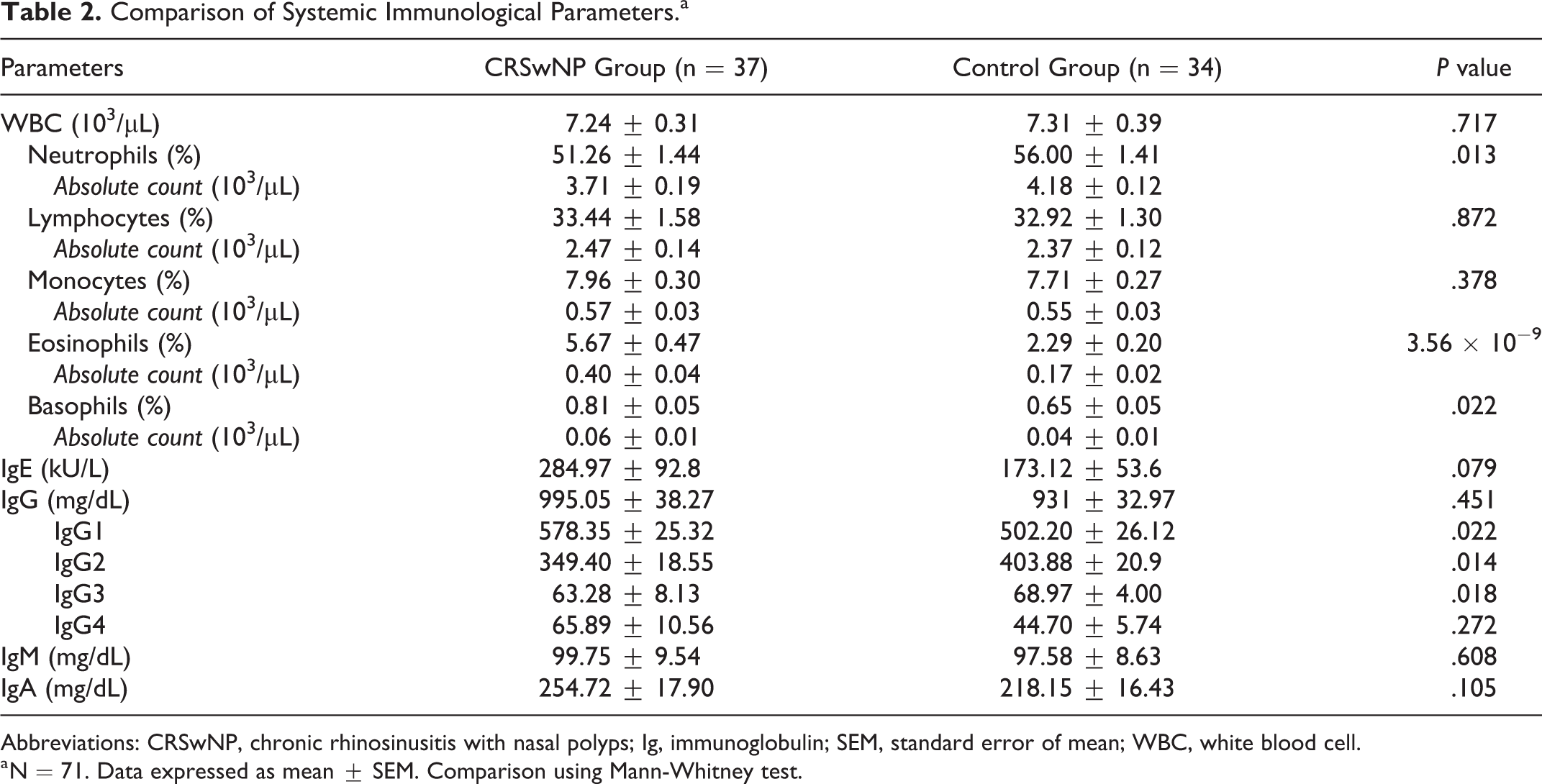
Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; Ig, immunoglobulin; SEM, standard error of mean; WBC, white blood cell.
a N = 71. Data expressed as mean ± SEM. Comparison using Mann-Whitney test.
In addition, we tried to find out if patients with AERD diverge from the remaining patients in the CRSwNP group but no significant differences about these immunological variables were detected. When we exclude these 6 patients with AERD from the CRSwNP group, we still found a significant difference concerning higher eosinophil and basophil relative count (P = 5.41 × 10−9 and P = .020), higher IgG1, and lower IgG3 concentration values (P = .048 and P = .044), between CRSwNP without AERD and control groups.
A Kruskal-Wallis test (N = 68) was also run for these continuous variables considering 3 different groups: control group without CLRD, CRSwNP without CLRD, and CRSwNP with CLRD. Patients from the control group with CLRD (n = 3) were not included in this subanalysis because of their limited number. Neutrophil (P = .031) and eosinophil relative count (P = 1.5 × 10−7), and IgG1 (P = .027), IgG2 (P = .015), and IgG3 (P = .028) differed significantly between the groups. For relative eosinophil count and IgG1 concentration levels, there was a crescendo trend in their mean values between control group without CLRD, CRSwNP without CLRD, and CRSwNP with CLRD; and an inverse pattern (decrescendo) was observed for relative neutrophil count and IgG2 and IgG3 (Figures 1 and 2).
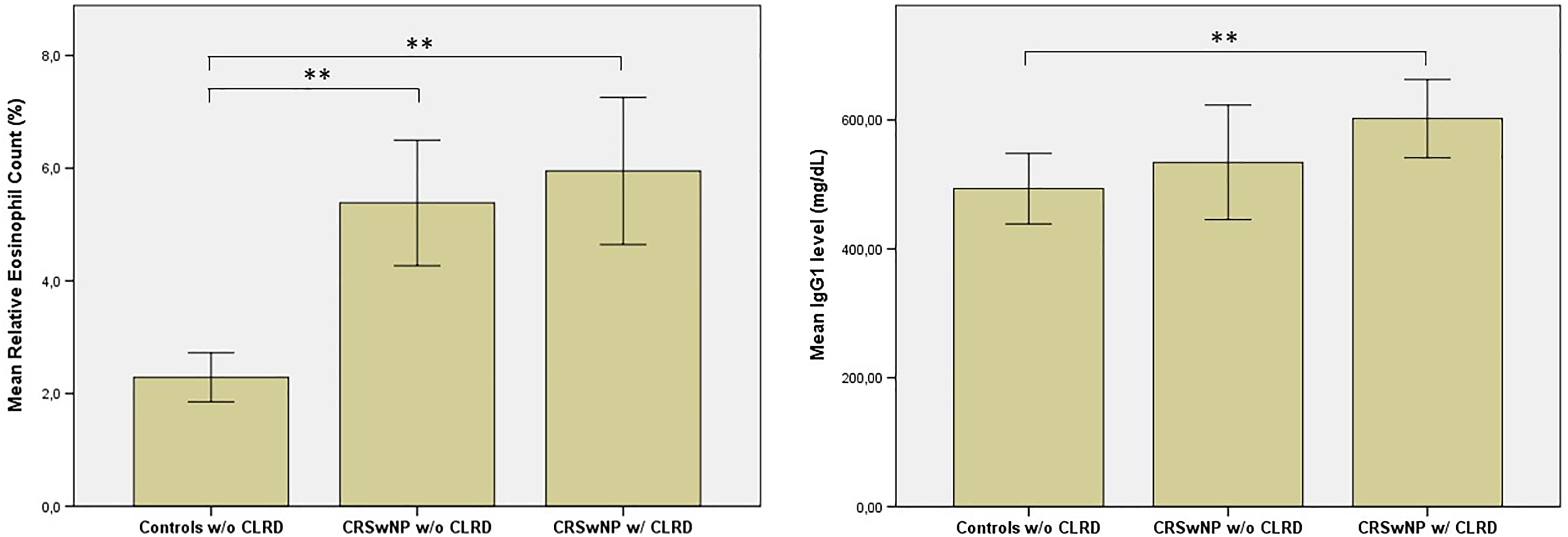
Mean relative eosinophil count (%) and serum concentration levels of IgG1 in controls without chronic lower respiratory diseases (controls w/o CLRD), in patients with CRSwNP without CLRD (CRSwNP w/o CLRD), and in patients with CRSwNP with CLRD (CRSwNP w/ CLRD). N = 68. Significance levels are marked as “*” if P < .05 and “**” if P < .01. Kruskal-Wallis test (P < .001 and P = .037, respectively) was performed and pairwise comparisons were made using Dunn post hoc test. CLRD indicates chronic lower respiratory diseases; CRSwNP, chronic rhinosinusitis with nasal polyps; IgG1, immunoglobulin G class 1; w/, with; w/o, without.
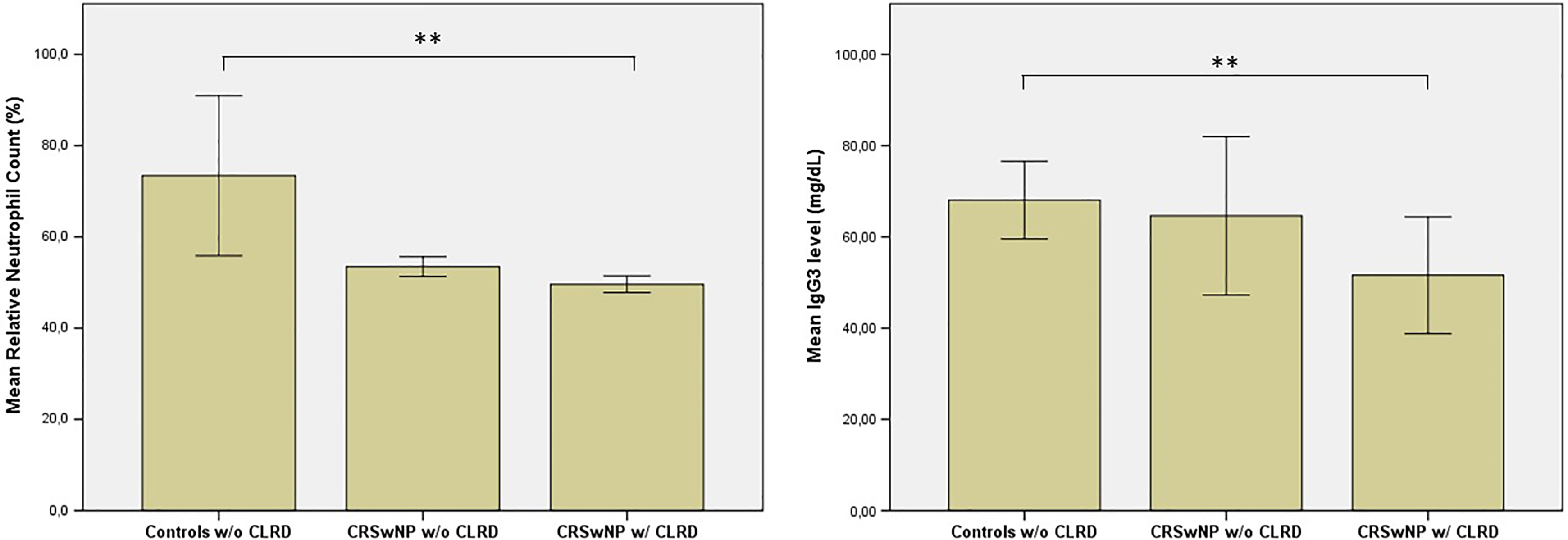
Mean relative neutrophil count (%) and serum concentration levels of IgG3 in controls without chronic lower respiratory diseases (controls w/o CLRD) and in patients with CRSwNP without CLRD (CRSwNP w/o CLRD). N = 68. Significance levels are marked as “*” if P < .05 and “**” if P < .01. Kruskal-Wallis test was performed (P = .031 and P = .018, respectively) and pairwise comparisons were made using Dunn post hoc test. CLRD indicates chronic lower respiratory diseases; CRSwNP, chronic rhinosinusitis with nasal polyps; IgG3, immunoglobulin G class 3; w/o, without.
Relating to humoral immunodeficiency (Table 3), we did not find a higher prevalence of immunoglobulin classes (5 cases, 13.5%) or subclasses deficiency (7 cases, 18.9%) compared to our control group (3 [8.8%] and 7 [20.6%] cases, respectively). No cases of common variable immunodeficiency were diagnosed in the entire sample. One (2.9%) case among CRSwNP and 2 (5.4%) cases among controls had an IgAGMD plus IgG1-3 deficiency (combination of selective classes [IgA, IgG, or IgM] plus IgG subclasses deficiency).
Prevalence of Immunoglobulin Classes and Subclasses Deficiency.a
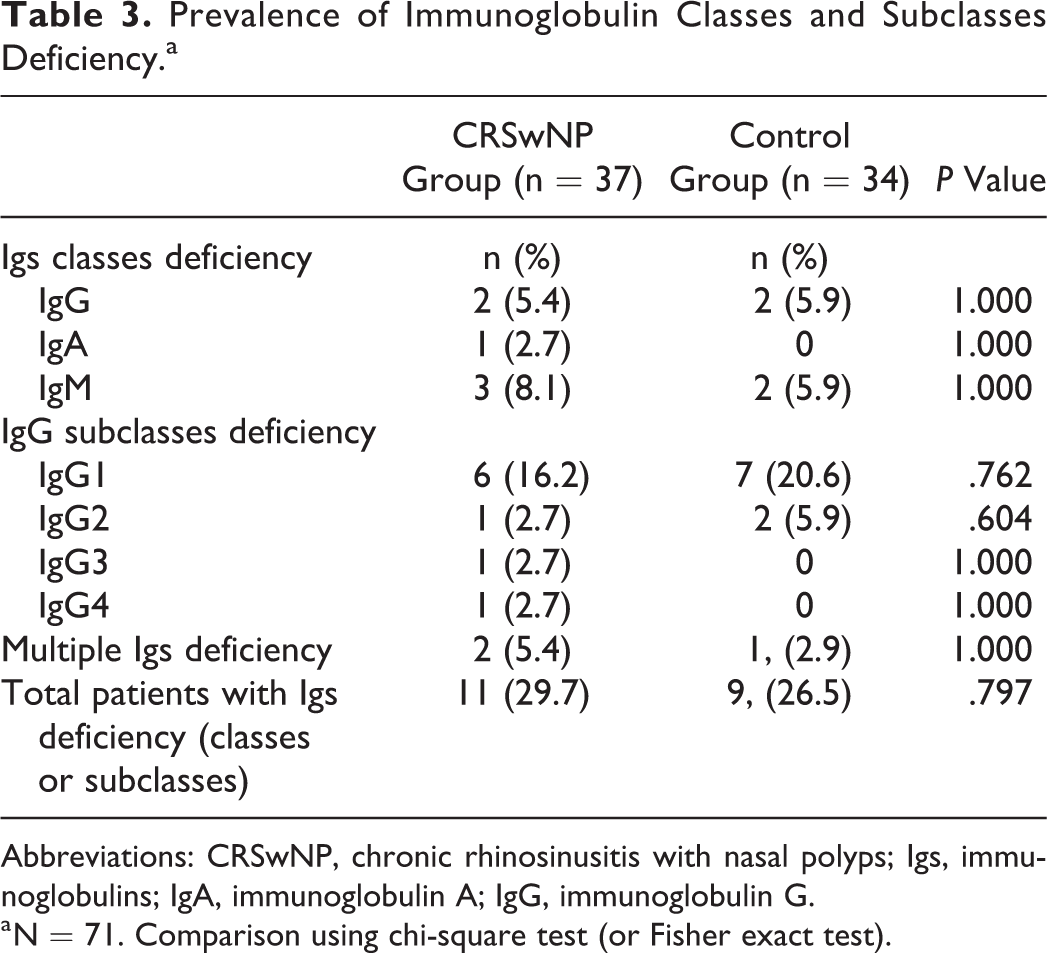
Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; Igs, immunoglobulins; IgA, immunoglobulin A; IgG, immunoglobulin G.
a N = 71. Comparison using chi-square test (or Fisher exact test).
Discussion
Our case and control groups had no significant differences concerning baseline demographic features, such as race, gender, or age.
Comparing comorbidities (Table 1), the prevalence of allergic rhinitis and atopic asthma did not differ significantly between cases and controls. In addition, the prevalence of atopy was 32% in the CRSwNP group, which is close to the range values of the reported prevalence of atopy in the general population (20%-30%). 15 These results corroborate previous studies 16 -18 that support the involvement of non–IgE-related mechanisms on CRSwNP etiopathogenesis.
On the contrary, there was a statistically significant higher prevalence of nonatopic asthma and COPD (both classified as CLRD) among patients with CRSwNP compared with controls. In total, 67.6% of patients with CRSwNP had a concomitant diagnose of CLRD, and this value is in accordance with a recent study which reported a CLRD prevalence (asthma plus COPD) of 72.5%. 19 However, the COPD prevalence reported on that study (7.5%) was lower than the 21.6% found in our study. The association between CRSwNP and asthma is well established, but the association of CRS and COPD despite being suggested has been much less investigated. 11 In 2011, a study in 90 patients with COPD demonstrated that 53% had concomitant symptoms of rhinosinusitis and 64% had signs of CRS in CT scan. 20 A study made in Norway in 2015 (the HUNT study-MRI: The Nord-Trøndelag Health Study with magnetic resonance imaging), with patients with COPD, asthma, and controls submitted to MRI, showed that the probability of paranasal sinus opacification was 6 times higher in COPD and 2-fold higher in patients with asthma compared to the control group. 21 In addition, there are clinical research studies showing a high prevalence of sinonasal symptoms in patients with COPD (75%) 22 and an inverse correlation between nasal patency evaluated by rhinomanometry and pulmonary airflow obstruction (FEV1%), and therefore to COPD disease severity. 9 The true prevalence of CRSwNP among patients with COPD needs future investigation using endoscopic-based approaches. Our study took place in Castelo Branco District, within the Interior Centre Region of Portugal, an area internationally known for its textile industry, mainly wool manufacturing, potentially explaining the high prevalence of COPD in our CRSwNP sample. Another important point is that asthma and COPD may be difficult to distinguish, especially in patients with history of tobacco consumption or exposure to noxius particles or gases, and in the elderly individuals, who often have overlapping clinical features of both diseases. 23
=In Western patients, it has been suggested that CRSsNP is more distinctly a neutrophilic process, while CRSwNP is more eosinophilic, based on the relative degree of nasal tissue infiltration. 1 It was interesting to observe that in CRSwNP the peripheral relative counts of eosinophils and neutrophils had the same behavior to what happens locally. There was a significant reduction in the relative neutrophil count among CRSwNP, with a decrescendo tendency if comorbid CLRD was present and the opposite occurred with the eosinophil count.
Similarly to other published study, 2 concentration values of serum IgG, IgA, IgM, and IgE did not show a significant difference between CRSwNP and controls. But contrary to that study, where no significant difference about serum IgG subclasses concentration values was observed, 2 in our study we found higher IgG1, but lower IgG2 and IgG3 serum levels in CRSwNP compared to controls, and these variations were more pronounced if CLRD were present. In patients with asthma, it has already been studied that IgG subclasses in bronchoalveolar lavage (BAL) and epithelial lining fluid are significantly higher than in controls, mainly due to increased leakage from blood, with IgG1 quotient between BAL fluid and serum concentrations having the highest value and IgG3 the lowest. 24 Similar studies should be done in CRSwNP, in nasal lavage fluid and tissue homogenates, to shed light in this subject. Meanwhile, an immunofluorescent study in nasal polyps from 100 patients has already shown a positive labelling for IgG in all specimens, for C3b complement fraction in 80% and negative immunofluorescency for IgM or IgA3. Van Zele et al demonstrated that nasal tissue homogenates showed significantly higher concentrations by immunonephelometry of IgG, IgE, and IgA in CRSwNP and also found by enzyme-linked immunosorbent assay that the percentage of IgG1 subclass was significantly higher among tissue homogenates in CRSwNP compared to controls. 2 A recent study in patients with CRSwNP and AERS also pointed to the importance of local IgG1 against staphylococcus enterotoxins (SEE), showing that this antibody can enhance the activity of anti-SEE IgEs as conventional antibodies or as “superantibodies” through complementary determining regions and framework regions to SEEs in SEE-anti-SEE IgE-FcεRI complexes. 25
We hypothesize that systemic IgG1 subclass switching is involved in CRSwNP pathogenesis and may be an important link to lower airway diseases, as there is a progression toward increasing mean plasmatic values in those patients. This is interesting, since each IgG subclass has a unique profile, for example, soluble protein antigens and membrane proteins primarily induce IgG1 switching. 26 This subclass is also important in antibody response to allergens, has the longest serum half-life, is capable of complement activation by C1q binding, and is the main IgG subclass to cross placenta and mucosal barrier. 26
Moreover, there are previous studies showing that IgG1 has a strong binding affinity to the neonatal Fc receptor (FcRn) compared to the other subclasses. 27,28 This receptor was originally identified in suckling rats as the receptor involved in IgG transport across the intestinal epithelium into the bloodstream but has now been demonstrated to be expressed in many adult tissues and cell types, 29 with predominant expression in respiratory system. 30 Recently, this receptor has also been identified in human nasal epithelium. 31 Apart from regulating and extending the serum half-life of IgG, FcRn orchestrates IgG-based immune responses at mucosal sites, contributing to immunosurveillance at host-environment interfaces within the adult organism. 32
In addition, in vitro studies with serum from patients with asthma showed that antigen-specific IgG1 and IgG3 antibodies can induce eosinophil degranulation, and that IgG-depleted serum but not IgE-depleted serum abolished this degranulation. 33 A possible link between IgG1 and tissue and peripheral eosinophilia has to be addressed in future investigations, since inflammation seen in CRSwNP can be reliant on IgG-dependent eosinophil-mediated cytotoxicity.
The higher rate of occupational dust exposure among patients with CRSwNP compared to controls corroborates the important role of this factor in the etiopathogenesis of CRSwNP and CLRD, as already suggested by previous studies. 17,34 Evidence points to a risk factor for CRS that is mainly due to the inhalation of lower molecular weight (LMW) particles (<5 kDa) which, contrary to high-molecular weight) particles that induce a well-known IgE-mediated immune response, induce airway inflammation through mechanisms that are far less known. 16,17 It can include the classical “irritant response” plus LMW sensitization of the adaptive immune system by acting as haptens (attached to large carriers such as airway proteins). 16,35,36 An investigation about sensitization to methylene diphenyl diisocyanate (MDI), an LMW particle, in a car upholstery factory found that the prevalence of MDI-induced occupational asthma/eosinophilic bronchitis was strongly associated with the presence of serum-specific IgG antibodies to an MDI–human serum albumin conjugate. 37
All these recent findings seem relevant to understand the systemic immune profile results that we found. It will be necessary future studies to compare FcRn expression among CRSwNP and controls and its relationship with IgG1 subclass switching in this disease. Following the concept of “one airway, one disease,” this IgG1-mediated immune response in patients with CRSwNP may be a key piece in understanding its interrelation with CLRD, namely nonatopic asthma and COPD and to clarify the role of occupational dust exposure, specifically LMW particles, in their etiopathogenesis.
Our prevalence results of IgG subclasses (18.9%) and immunoglobulin classes (13.5%) deficiency in CRSwNP are similar to the previous reported values in the literature for CRS (5% to 50% for IgG subclasses deficiency and 13% for IgG, IgA, or IgM antibody deficiency). 38 However, since no significant difference was detected between our CRSwNP and control groups (8.8% and 20.6%, respectively), it seems unlikely that immunoglobulin class and subclass deficiencies are important factors in CRSwNP etiopathogenesis. Larger prospective and controlled studies about this topic are needed.
Our study has some limitations: a limited sample size from a single institution, the use of patients waiting for septoplasty as controls, and a high percentage of CRSwNP under inhalant steroids. Nonetheless, this is to our knowledge the largest controlled study to analyze IgG subclasses. To surpass the potential bias effect caused by corticosteroids influence on WBC count, systemic steroids were not prescribed within 3 months before serum specimen’s collection. However, patients who needed steroids plus long-acting β2-agonists for their asthma control were permitted to keep their long-term medication. These inhalant associations are considered to have negligible systemic side effects. 39 Although, if we consider a potential effect of steroids intake on our hematological findings, it would be in the opposite way of our observed results (higher total leukocyte count, 40 higher relative neutrophil count, 41 lower relative eosinophil 42 and lymphocyte count, lower levels of total IgG/IgA/IgE and IgG1 and IgG2 subclass deficiencies 43 ). This means that our observed differences in immunological profile might have been even more pronounced if patients with CRSwNP were not taking inhalant corticosteroids. Moreover, immunological differences found between CRSwNP and patients submitted to septoplasty would be probably even bigger if we used a randomly selected group of non-CRS individuals from the general population, as it is known that patients undergoing septoplasty also have significant nasal symptoms, in association with some degree of nasal inflammation. This investigation deserves further replication in larger samples and with patients from other institutions. In a bigger sample, a multivariate regression analysis would be of added value to identify the variables that have an independent correlation with the disease, allowing at the same time to control the effect of multicollinearity and outliers.
Conclusion
A distinct systemic immunologic profile in patients with CRSwNP concerning leukogram and humoral immunity was observed. Changes in peripheral leukocyte count and the systemic IgG1 subclass shift are similar to what is described to happen in nasal polyp tissue. The observed differences were more marked if CLRD were present. These variations may be involved in CRSwNP pathogenesis and a possible role for IgG1-mediated response must be investigated.
Footnotes
Authors’ Note
Rafaela Veloso-Teles contributed to study design, data collection, statistical analysis, discussion, and revision. Rui Cerejeira, Rosa Roque-Farinha, and Christian von Buchwald contributed to study design, discussion, and revision. This study was performed according to the principles of the Declaration of Helsinki Institution at which the work was performed: Cova da Beira Hospital Centre.
Acknowledgments
The authors thank Professor Søren Jacobsen, M.D., D.M.Sci, from Department of Rheumatology at Rigshospitalet (Copenhagen, Denmark) for is valuable comments and suggestions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.