
Abstract
EPOS 2012 states that investigation is needed to study a possible role for food allergy in the initiation and perpetuation of chronic rhinosinusitis with nasal polyps (CRSwNP). Our main goal was to compare serum levels of food-specific immunoglobulin G (IgG) and IgE antibodies in patients with CRSwNP and controls. A prospective case–control study with 33 patients with CRSwNP and 31 controls without CRS was carried out. Clinical data were gathered through a systematic interview and blood sample was collected. Enzyme-linked immunosorbent assay tests using OmegaDiagnostics kit with 40 food allergens for detection of specific IgG antibodies were performed and food-specific IgE antibodies were determined by immunoassay using ImmunoCAP. Immunoglobulin classes and IgG subclasses levels were also evaluated. Statistical analysis was performed using SPSS v.23. The overall sum of food IgG antibodies was significantly lower in CRSwNP compared to control group, and this difference was also observed for different specific IgG antibodies (corn, soya, grain legumes, pear and apple, berries, citric fruit). In controls, a positive correlation between IgG1 and the sum of food IgG antibodies was seen, but in CRSwNP group a negative correlation was found. In addition, a significant higher level of IgG1 and lower IgG2 and IgG3 was found among patients with CRSwNP. Levels of serum-specific IgE antibodies against multiallergen food mix (fx5) and against shrimp, strawberry, orange, rye, or egg yolk, as well as the sum of food IgE antibodies, did not differ significantly between the groups. These findings suggest that food allergy does not have an important role in CRSwNP etiopathogenesis, whether it is IgG or IgE mediated. Moreover, the observed suppression of specific IgG antibodies against food allergens, its negative correlation with IgG1 and the IgG1 switching in CRSwNP, can be related to deviated IgG responses against other targets (eg, airborne particles) and warrants future investigation.
Introduction
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a common chronic inflammatory disease with high morbidity that results in a significant decrease in patient quality of life. The etiopathogeny of CRSwNP remains obscure, and it is still considered a difficult-to-treat pathology. There is, however, a movement away from the pathogen-driven hypotheses, and an emerging consensus that the persistent inflammation that defines chronic rhinosinusitis (CRS) results from a dysfunctional host–environment interaction, involving various exogenous agents and changes in the sinonasal mucosa. 1 This overall concept is in agreement with the current understanding of the etiopathogenesis of chronic mucosal inflammatory disorders in general, driven by an imbalance between the host, commensal flora, potential pathogens, and exogenous stresses. 1,2 Chronic rhinosinusitis with nasal polyps and asthma (mainly non-immunoglobulin E [IgE]-mediated asthma) frequently coexist in the same patients, 1 and although their etiopathogenesis may be linked, their interrelationship and subjacent mechanisms are unclear.
Food allergy is an adverse food reaction that involves abnormal immune responses to food allergens, which can involve IgE-mediated (immediate food responses) or non-IgE-mediated reactions (delayed food responses). 3 The prevalence of food allergy is known to be higher in patients with allergic rhinitis, 4 and cross-reactivity is known to occur between aeroallergens and food allergens. 5 Moreover, food allergy is known to be a risk factor for asthma development and lower respiratory symptoms may be seen in food-induced allergic reactions in asthmatic patients. 3 In addition, it is known that inhalation of food allergens can induce respiratory symptoms, for example, in occupational asthma in workers handling food products and derivates. 6
A possible role of food allergy in CRSwNP has been raised in 2 case–control studies 7,8 that found 70% and 81% positivity for intradermal food tests in patients with CRSwNP and only 34% and 11% in the control group, respectively. The authors argued that the fact that intradermal food test correlated poorly with serum-specific IgE levels pointed to the involvement of other non-IgE-mediated food hypersensitivities. 8 Meanwhile, EPOS 2012 states that further research is needed to investigate a possible role for food allergy in the initiation and perpetuation of CRSwNP. 1
Controversial evidence exists about IgE food sensitization in patients with CRSwNP, with authors reporting prevalence between 22% and 74% depending on used technique (skin prick test [SPT] vs radioallergosorbent test [RAST]). 9,10 In 2016, a comparative study between patients with CRSwNP and chronic rhinosinusitis without nasal polyps (CRSsNP) using enzyme allergosorbent test (EAST) found no significant difference between food IgE sensitization prevalence, type, and severity, concluding that food atopy is unlikely to be a major factor in nasal polyposis etiopathogenesis. 11 The prevalence of food allergy is difficult to estimate mainly due to diagnosis issues. For example, SPT positivity does not necessarily prove that the food is causal as the positive predictive value is less than 50% but if negative essentially confirms the absence of IgE-mediated allergic reactivity since negative predictive value is greater than 95%. 3 In vitro assays are also useful modalities in food allergy study. Initially, RAST were used, but more recently quantitative measurement of food-specific IgE antibodies such as ImmunoCAP have been utilized and studies have found them to be more predictive of symptomatic IgE-mediated food allergy. 3 Moreover, ImmunoCAP (Thermo Fisher Scientific, Uppsala, Sweden) has the advantage of the lack of interference from allergen-specific immunoglobulin G (IgG) antibodies. 12 However, undetectable serum food-specific IgE levels may be associated with clinical reactions as well and the double-blind placebo controlled food challenge is still considered the gold standard for food allergy diagnosis, but because of its methodological difficulties, it is rarely conducted in clinical practice.
Recently, IgG antibodies against food antigens have been suggested to cause low-grade inflammation in irritable bowel syndrome, with symptoms improvement after dietary elimination based on specific IgG profile of the patient. 13 This theory, called the “leaky gut syndrome” (LGS), proposes that it is the increased permeability of the gut wall to macromolecules that leads to activation of the immune system, which may initiate production of specific IgG antibodies against food, resulting in chronic inflammation sustained by repeated intake of allergenic foods. 2,14 The LGS and the IgG-mediated food allergy have been investigated in different chronic inflammatory pathologies, such as obesity, 15 type 1 and type 2 diabetes, 16,17 chronic liver disease, 18 chronic kidney disease, 19 chronic heart failure, 20 depression, 14,21 and asthma. 22 The role of IgG antibodies against food remains controversial, namely because they can be detected in healthy individuals and there are no standardized cutoff values. In fact, IgG food detection is still only recommended for investigational purpose and not for individual use. 23 The development of commercial kits with standardized food antigen extraction and purification, using an optimized and validated enzyme-linked immunosorbent assay (ELISA) method, permits to overcome matters of reproducibility and variability.
Our main goal was to compare specific IgG and IgE antibodies dosage against food allergens in patients with CRSwNP and controls, trying to clarify if food allergy can be associated with CRSwNP.
To our knowledge, this is the first study to investigate the hypothesis of IgG-mediated food allergy in CRSwNP pathogenesis and to use ImmunoCAP technology to evaluate IgE food sensitization in CRSwNP.
Patients and Methods
A case–control observational study was performed according to established ethical guidelines and approval of ethics committee at the Cova da Beira Hospital Centre (deliberation number 82/2015). A signed informed consent was obtained from each participant in the study.
Sample
All the cases were about to undergo endoscopic sinus surgery for CRSwNP refractory to medical treatment (topical long-term and systemic short-term steroids), in a district hospital center, from January 2016 to October 2018. Diagnosis of CRSwNP was established using the definition of EPOS 2012. 1 The cases were selected consecutively from the waiting list and had their disease confirmed endoscopically by computed tomography (CT) scan and histological examination of the subsequent surgical specimen. Patients were selected after applying the following exclusion criteria: concomitant benign or malignant sinonasal tumors, CRSsNP, antrochoanal polyps, polyps associated with fungal rhinosinusitis, primary ciliary dysfunction, cystic fibrosis, innate or acquired immunodeficiency (eg, human immunodeficiency virus; immunosuppressive drugs), autoimmune diseases (eg, systemic vasculitis, inflammatory bowel disease), or patients with history of or under allergen-specific immunotherapy. No course of oral corticosteroids was given to patients with CRSwNP at least 3 months before serum specimen collection.
Controls were selected from patients in the waiting list for septoplasty, after excluding patients with symptoms and endoscopic or imagiological signs (in CT scan) of CRS; controls with innate or acquired immunodeficiency, autoimmune diseases, or patients with history of or under allergen-specific immunotherapy were also excluded.
Data Collection
Clinical data were gathered through a systematic interview. Dietary habits were collected using the Portuguese-validated Food Frequency Questionnaire (QFA). 24 Every questioned food item was scored between an intake of 0 (never or less than 1 per month) and 8 (6 or more per month).
Chronic lower respiratory diseases diagnosis was established by a respiratory physician. Blood sample was collected to determine immunoglobulin classes, IgG subclasses levels and specific IgG and IgE against food allergens. Immunoglobulin classes were determined by electrochemiluminescence immunoassay using Cobas 6000 analyzer (Roche Diagnostics, The Binding Site Group, Birmingham, United Kingdom) and IgG subclasses through the Optilite turbidimetric analyzer (Binding Site).
Enzyme-Linked Immunosorbent Assay
Enzyme-linked immunosorbent assay tests for semiquantitative analysis of serum IgG antibodies to 40 food allergens were performed using OmegaDiagnostics (Littleport, Cambridgeshire, United Kingdom) detection kit. A microplate reader with 450-nm filter was used to read the final absorbance of each well. The given concentration of the 2 standards provided on the kit allowed to infer about antibody IgG concentration (arbitrary units/mL [AU/mL]) on each well. Some food antigens are grouped in the same well as food mixtures, confering in total 21 wells (corn; oat; rice; rye; wheat; cow’s milk; egg white; egg yolk; white fish misture [cod, haddock, plaice]; shellfish misture [crab, lobster, prawn]; soya; legume bean misture [haricot, kidney, pea]; mustard mixture [cabbage, broccoli, cauliflower]; gluten, apple, and pear; berries misture [rasperry, strawberry, blackberry]; citrus mixture [orange, lemon, grapefruit]; nut mixture [almond, cashew, hazelnut, peanut]; yeast [bakers and brewer’s]; chicken and turkey; and pork and beef). A positive response was considered if concentration value was ≥8 AU/mL, and the response of the reaction was classified as grade 1+ if ≥8 and <12.5, grade 2+ if ≥12.5 and <25, and grade 3+ if ≥25 AU/mL, according to suggested ranges of the manufacturer.
ImmunoCAP Food Allergen Test
Specific IgE antibodies for food antigens were determined by immunoassay using ImmunoCAP Food Allergen tests by Thermo Fisher Scientific (Uppsala, Sweden) for the following food allergens: fx5—egg white, milk, fish, wheat, peanut, and soybean; f24—shrimp; f44—strawberry; f33—orange; f5—rye; and f75—egg yolk. Positive results were considered if serum concentration was above 0.35 KUA/L.
Statistical Analysis
Statistical analysis was performed with Statistical Package for Social Sciences (IBM SPSS Statistics for Windows, version 23.0). Descriptive statistics was used in sample characterization. Mann-Whitney U test for independent samples was used to compare continuous variables between the 2 groups. Pearson χ2 test (or Fisher exact test when appropriate) was used to test association between categorical data. A nonparametric Spearman correlation was used to examine the relation between quantitative variables.
A P value <.05 was considered statistically significant.
Results
Sixty-four individuals were included: 33 patients with CRSwNP and 31 controls. Demographics, body mass index (BMI), and QFA scores of patients with CRSwNP and controls are presented and compared in Table 1. There were no significant differences between CRSwNP and control groups based on age, gender distribution, and BMI. According to QFA total score and subscores, no significant difference in the food consumption pattern was observed between groups.
Comparison of Sample Demographics, Body Mass Index (BMI), Presence of CLRDs (Chronic Lower Respiratory Diseases), Food Frequency Questionnaire (QFA) Score, and Subscores Between Patients With CRSwNP and Controls (N = 64).a
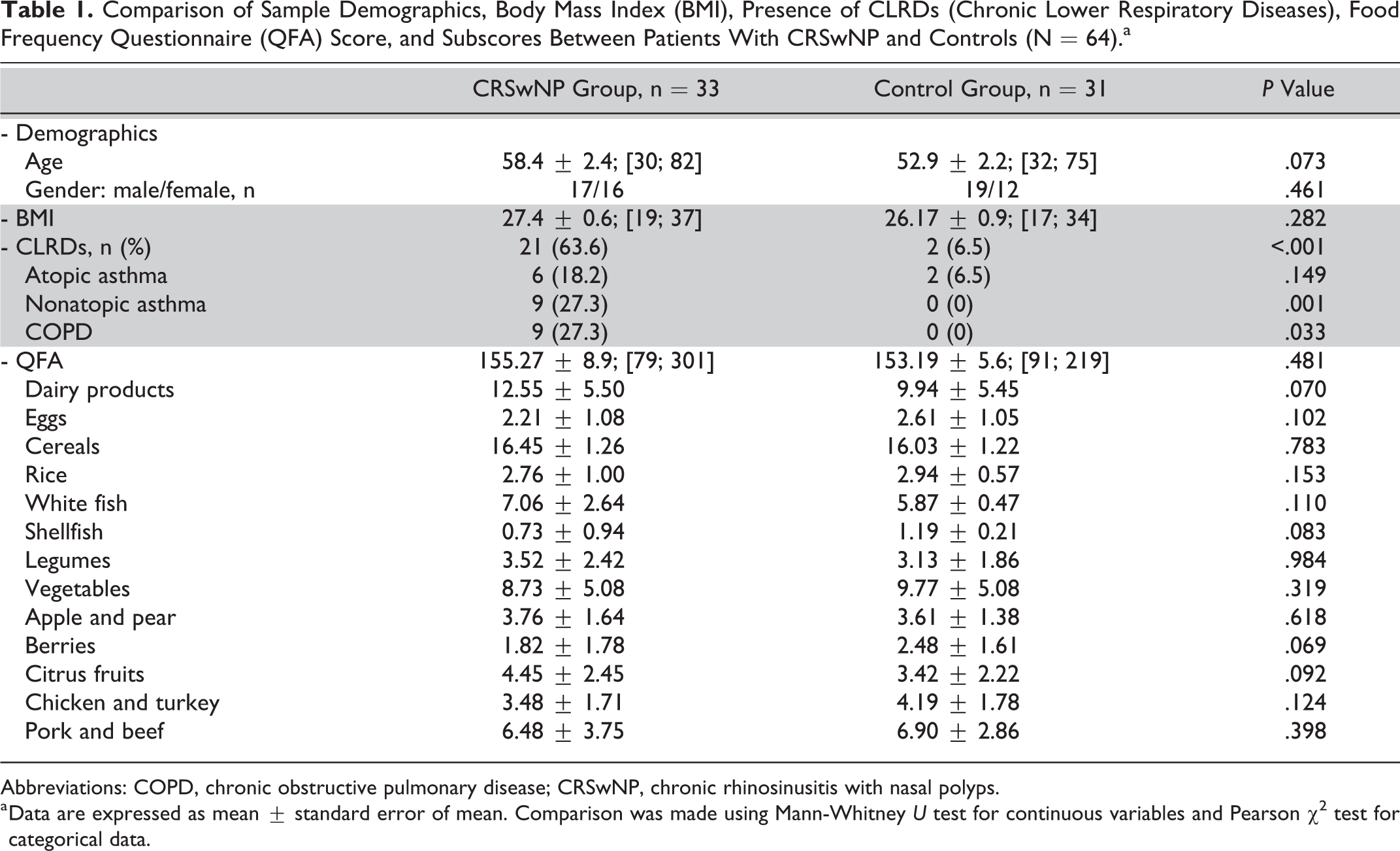
Abbreviations: COPD, chronic obstructive pulmonary disease; CRSwNP, chronic rhinosinusitis with nasal polyps.
a Data are expressed as mean ± standard error of mean. Comparison was made using Mann-Whitney U test for continuous variables and Pearson χ2 test for categorical data.
Chronic lower respiratory diseases were more prevalent in patients with CRSwNP (21 patients, 63.6%) than that in the control group (2 participants, 6.5%), in a statistically significant way (P < .001, Fisher exact test; Table 1). In CRSwNP group, 16 (48.4%) participants were under treatment with inhaled steroids with β2-agonists, whereas in the control group, only 2 (6.4%) were being treated with inhaled steroids.
Using the ELISA tests for serum IgG antibodies to 40 food allergens analysis, we found the overall sum of IgG levels to be significantly lower in patients with CRSwNP compared to the control group (P = .013) and this difference was also observed for specific IgG antibodies against corn (P = .009), soya (P = .002), grain legumes (P = .004), pear and apple (P = .0025), berries (P = .0005), and citric fruit (P = .007; Figure 1). Moreover, the prevalence of patients with positive food IgG antibodies was significantly lower in patients with CRSwNP (48.5%) compared to the control group (74.2%; Table 2). The overall sum of specific food IgG antibodies did not correlate significantly with BMI (P = .719) or age (P = .228).
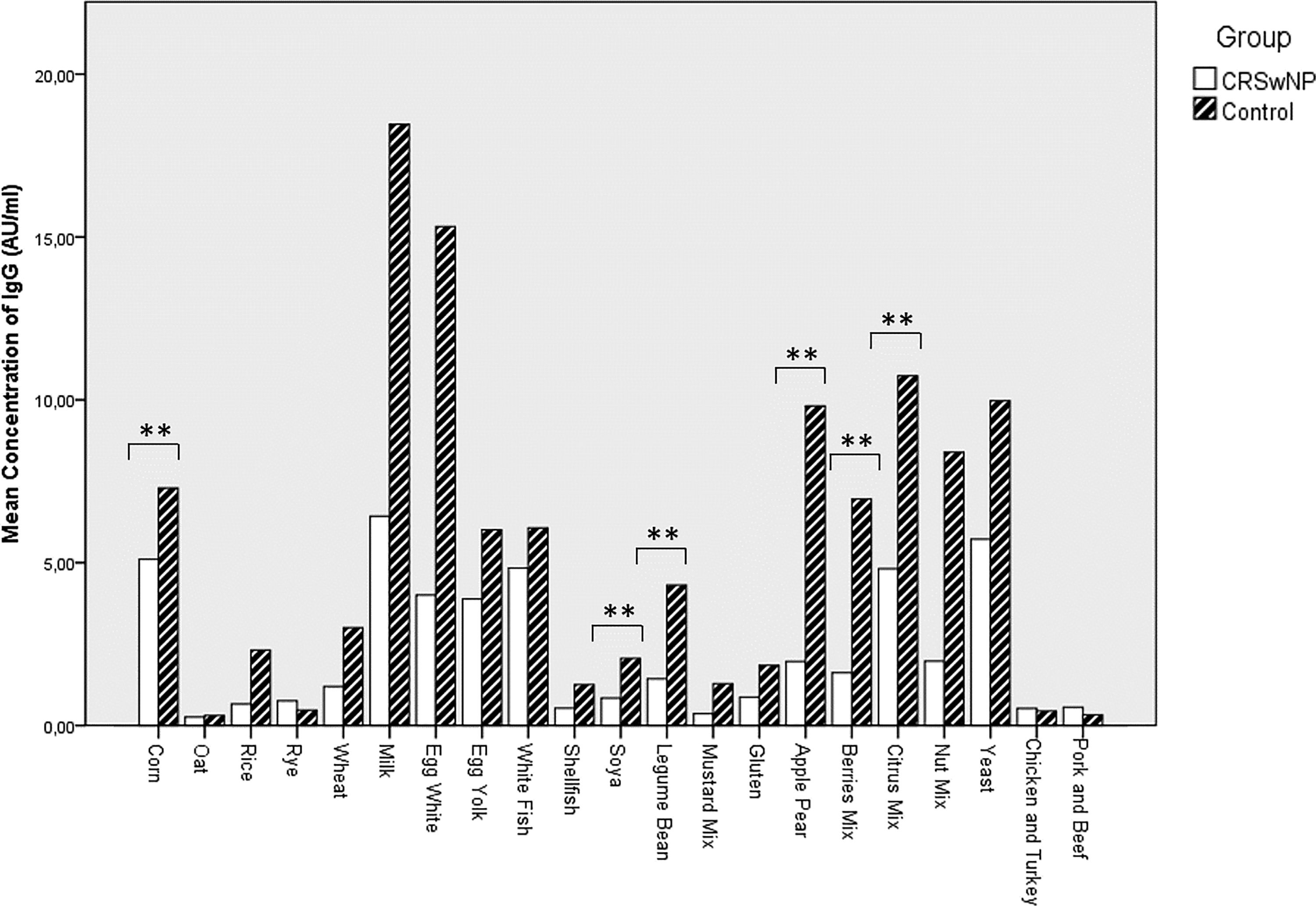
Comparison of the mean concentration values of specific IgG antibodies for different food allergens in patients with CRSwNP and controls, obtained in ELISA test. N = 64. **P < .01 using Mann-Whitney U test. CRSwNP indicates chronic rhinosinusitis with nasal polyps; ELISA, enzyme-linked immunosorbent assay; IgG, immunoglobulin G.
Comparison Between Serum Levels of Specific Food IgG Antibodies and Prevalence of Test Positivity Between Patients With CRSwNP and Controls (N = 64).a
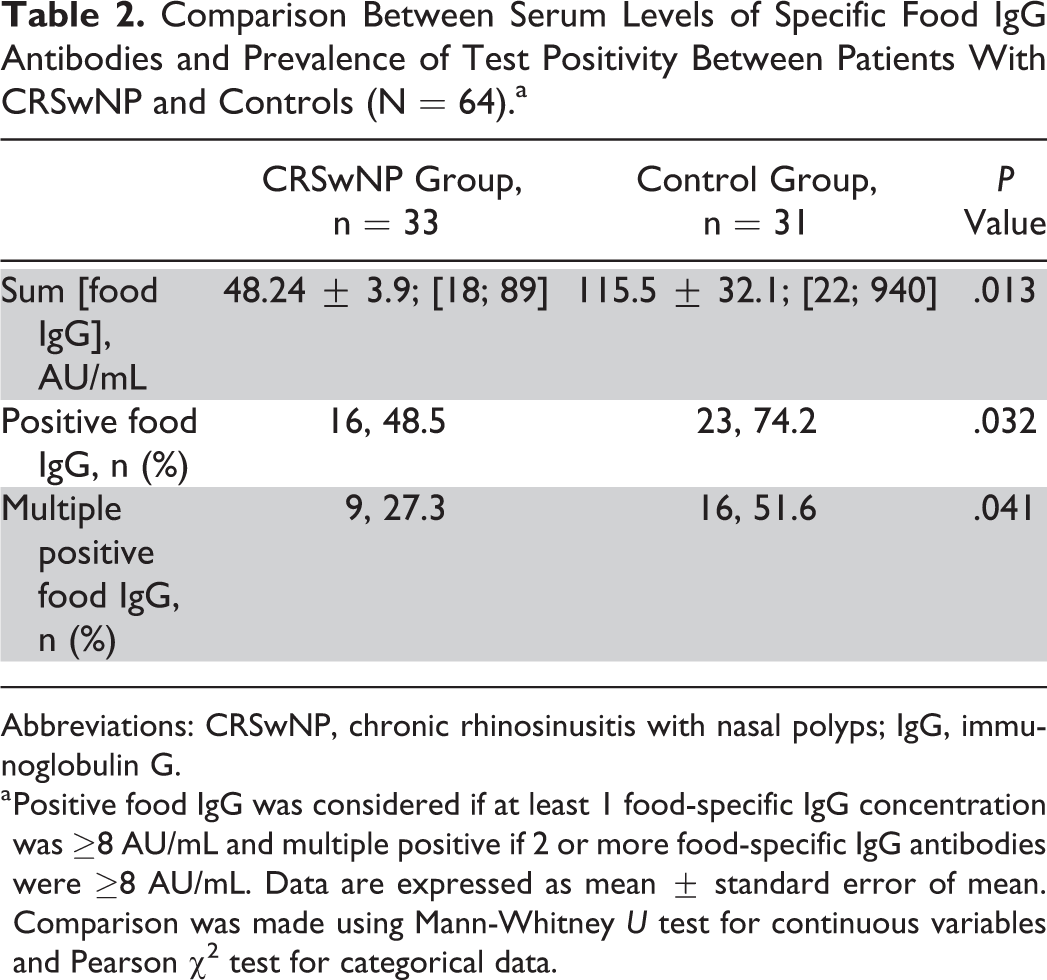
Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; IgG, immunoglobulin G.
a Positive food IgG was considered if at least 1 food-specific IgG concentration was ≥8 AU/mL and multiple positive if 2 or more food-specific IgG antibodies were ≥8 AU/mL. Data are expressed as mean ± standard error of mean. Comparison was made using Mann-Whitney U test for continuous variables and Pearson χ2 test for categorical data.
No correlation between specific food IgG antibodies and the frequency of consumption that particular food was observed: IgG antibodies against cow’s milk and dairy products consumption frequency (P = .710); IgG antibodies against egg white and egg consumption frequency (P = .505); and IgG antibodies against wheat and cereals consumption frequency (P = .676), among others. In global, considering the all sample, the specific IgG antibodies against food with higher mean concentration values in our sample were cow’s milk (12.25 AU/mL), egg white (9.49 AU/mL), citrus fruits (7.68 AU/mL), bakers and brewer’s yeast (7.78 AU/mL), and corn (6.17 AU/mL).
No correlation between total serum IgG level and sum of specific IgG against food was observed (P = .748). However, considering subclasses and the 2 sample groups, we found a negative correlation between IgG1 serum levels and sum of food-specific IgG concentration values in patients with CRSwNP and a positive correlation between IgG1 serum levels and sum of food-specific IgG concentration values in controls (Table 3).
Correlation Between the Overall Sum of Food Specific IgG Concentration and Total IgG and IgG Subclasses Levels in the Serum Among Patients With CRSwNP and Controls (N = 64).a
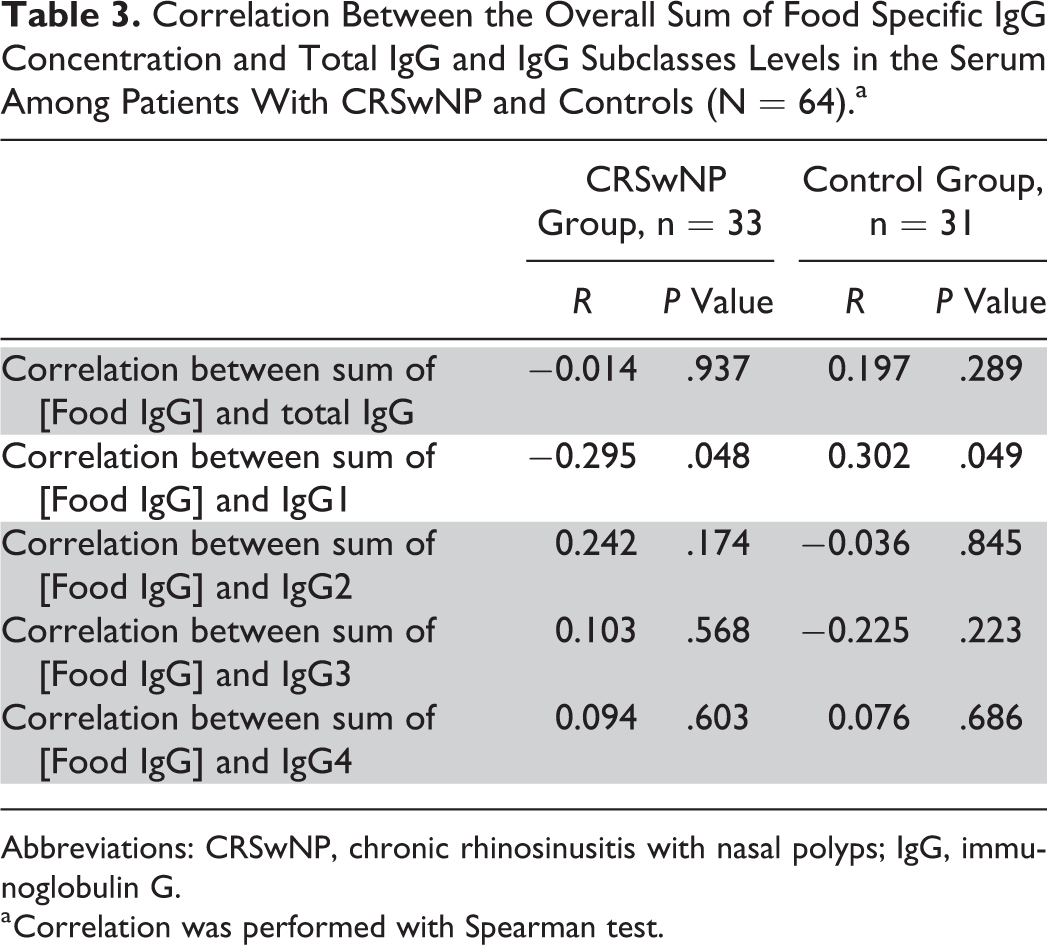
Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; IgG, immunoglobulin G.
a Correlation was performed with Spearman test.
Moreover, in CRSwNP, a statistically significant higher level of IgG1 subclass in the serum was detected compared to controls (P = .041) and lower levels of IgG2 (P = .048) and IgG3 (P = .014). Concerning total IgG and IgG4 subclass levels, no difference was identified.
No significant difference in IgE food sensitization was observed in relation to the overall sum of specific food IgE concentrations or the prevalence of positive IgE values between CRSwNP and control group (Table 4). Concerning specific food IgE dosage, no significant differences were observed for fx5: egg white, milk, fish, wheat, peanut, and soybean (P = .271); shrimp (P = .629); strawberry (P = .207); orange (P = .509); rye (P = .585); or egg yolk (P = .066).
Comparison Between the Overall Sum of Serum Levels of Specific Food IgE Antibodies and the Prevalence of Test Positivity Between Patients With CRSwNP and Controls (N = 64).a
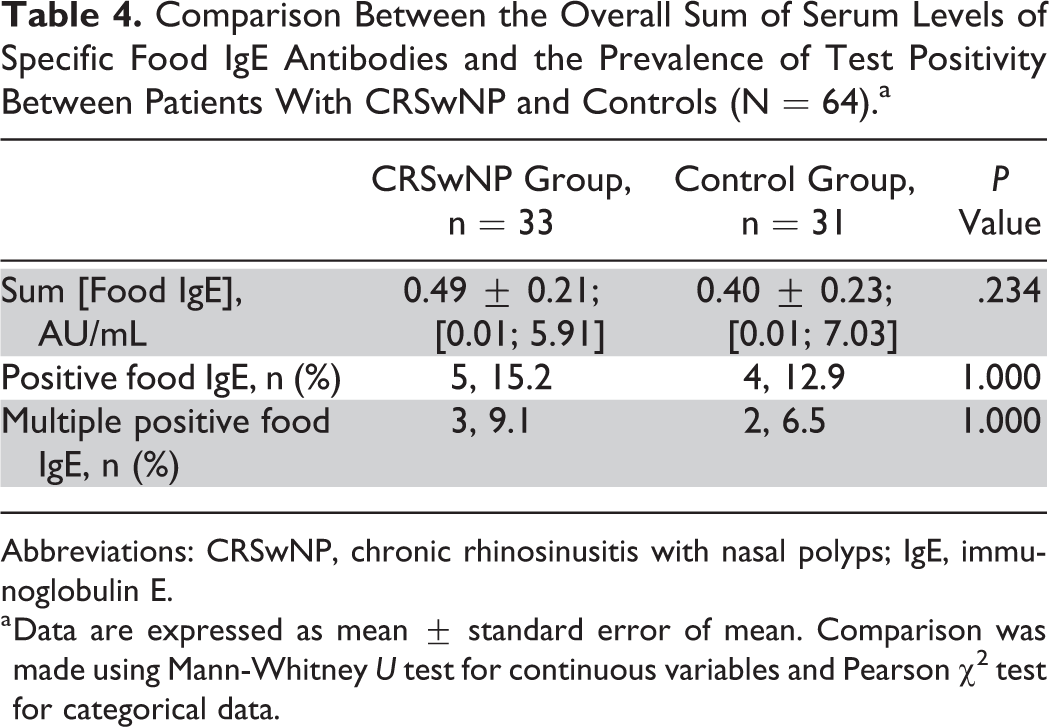
Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; IgE, immunoglobulin E.
a Data are expressed as mean ± standard error of mean. Comparison was made using Mann-Whitney U test for continuous variables and Pearson χ2 test for categorical data.
A positive correlation between total serum IgE levels and total specific IgE against food was observed (P = 5.12 × 10−9). Total IgE serum levels were significantly elevated in patients with CRSwNP compared to controls (P = .03). No correlation between the overall sum of specific IgG and IgE antibodies against food was observed (P = .936).
Discussion
Our results do not support the existence of an important role for food allergy in CRSwNP pathogenesis, independently of being an IgE- or IgG-mediated immune response. As already stated, the possible role of food allergy in CRSwNP has been raised in 2 case–control studies 7,8 that found 70% and 81% positivity for intradermal food tests in patients with CRSwNP and only 34% and 11% in the control group, respectively, with statistically significant differences. Meanwhile, some authors have criticized the value of intradermal food tests, namely for their increased risk of systemic reactions comparatively with SPT, noncorrelation to specific IgE levels, and high frequency of false-positive results. 25 Moreover, these 2 case–control studies have been carried out in the same investigational center and until now no replication of their results has been published elsewhere.
Regarding IgE-mediated food hypersensitivity, we did not find any significant difference in ImmunoCAP results considering IgE food serology test positivity or even in the sum of specific IgE class against food between CRSwNP and controls, in accordance to a previous publication that used EAST technique. 11 In that study, published in 2016, a positive correlation between total serum IgE level and sum of specific IgE antibodies against food was observed, 11 as we also found in this investigation. We report here prevalence of IgE food sensitization in patients with CRSwNP (15%) and in controls (13%), which are similar to the values described by Lill et al 10 (22% in CRSwNP and 14% in controls). Lill et al reported that patients with CRSwNP had higher rates of IgE positivity for milk compared to controls using RAST. However, this result was not replicated in other studies so far and the fact that they did not find any control with IgE positivity for milk must be seen with caution since milk has been reported as one of the most frequently food allergens in IgE dosage screenings in general population. 26 We did not find significant difference comparing fx5-multifood allergen panel (that includes milk) or in single specific IgE antibody dosage for milk in case of fx5 positivity. The discrepancy in the prevalence of IgE-mediated food allergy among CRSwNP between published studies might be due to different methodologies used, such as food allergy SPT, intradermal food allergy test, RAST, or EAST. The ImmunoCAP is considered to have higher sensitivity and better diagnostic capacity compared to RAST, 27 and this study was to our knowledge the first to use this technique in CRSwNP.
Concerning IgG-mediated food hypersensitivity, our results did not show higher antibodies dosage in CRSwNP, otherwise revealing an immune suppression of IgG response against food allergens in CRSwNP. The overall sum of food-specific IgG antibodies concentration was significantly reduced in CRSwNP comparing to controls and was not correlated with BMI or age. Moreover, a statistically significant reduction in IgG concentration against particular foods, such as corn, soya, legume beans, pear and apple, berries, and citric fruits, was observed in the CRSwNP group, irrespective of food-type consumption. We hypothesize that this suppression of IgG-mediated immune response against food allergens could be the result of deviated IgG responses to other agents (eg, airborne particles) in CRSwNP, which must be clarified in future investigations. In accordance with this hypothesis, it is interesting to note that in the CRSwNP group, a significant inverted correlation was observed between the sum of food-specific IgG antibodies and IgG1 subclass level in serum, as opposed to the control group in which a positive correlation was found. Moreover, we observed that patients with CRSwNP showed a subclass switching toward IgG1, with significant higher values of this IgG subclass and lower levels of IgG2 and IgG3, compared to controls.
There is recent evidence suggesting that occupational exposure to dust can be related to the occurrence and persistence of CRS 28,29 and specifically to CRSwNP phenotype. 30,31 These studies point to a risk factor for CRS that is mainly due to the inhalation of lower-molecular-weight (LMW) particles (<5 kDa) which, contrary to high-molecular-weight particles that induce a well-known IgE-mediated immune response, induce airway inflammation through mechanisms that are far less known. It can include the classical “irritant response” plus LMW sensitization of the adaptive immune system by acting as haptens. 28,31,32 High-molecular weight agents are generally proteins from animal and vegetal origin while LMW agents include a wide variety of organic and inorganic compounds. In contrast to protein allergens, LMW agents are incomplete antigens (ie, haptens) that must bind to carrier macromolecules to become immunogenic. For example, LMW agents causing occupational asthma are typically highly reactive electrophilic compounds that are capable of combining with hydroxyl, amino, and thiol functionalities on airway proteins. 33 The innate chemical reactivity of most LMW agents has largely hampered the investigation of immunological mechanisms, owing to uncertainty about the antigens that elicit immunological responses. 33 The understanding of the interaction between LMW particles and respiratory proteins can lead to the identification of antigenic determinants involved in CRSwNP and non-IgE-mediated asthma and to the development of hapten-specific monoclonal antibodies to clarify the subjacent immunologic mechanisms.
Immunoglobulin G1, which was significantly elevated in the CRSwNP group, is an important subclass in antibody response to soluble protein antigens, membrane proteins, and allergens; has the longest serum half-life; is capable of complement activation by C1q binding; and is the main IgG subclass to cross placental and mucosal barriers. 34 The neonatal Fc receptor (FcRn), the receptor involved in IgG transport across mucosa barriers, has been demonstrated to be expressed in many adult tissues and cell types, including nasal mucosa, 35 has a strong binding affinity of IgG1 to FcRn compared to other subclasses, 36,37 and in animal models, it has been demonstrated a predominant expression in the airways compared to the intestine, skin, liver, spleen, and skeletal muscle. 38 In both human asthmatics and animal models of allergy, it has been showed that allergen-specific IgG-mediated response can contribute to Th2-mediated inflammation, 39 the predominant type of inflammation seen in Western patients with CRSwNP. 1 One study in patients with asthma has showed that IgG1 ratio between bronchoalveolar fluid and serum concentrations had the highest value among IgG subclasses. 40 Another study in patients with CRSwNP demonstrated that the relative concentration of IgG1 subclass was significantly higher among nasal tissue homogenates in CRSwNP compared to controls. 41 It is possible that an augmented IgG1 response mounted in airways could make the immune system more tolerant to food allergens in the intestinal mucosa, mainly to protein food antigens.
To our knowledge, this is the first investigation concerning food-specific IgG antibody levels in CRSwNP. Since food IgG sensitization seems to be reduced compared to controls, it seems unlikely to be an important factor in nasal polyposis pathogenesis. Our results showed an association between CRSwNP and an immune suppression of IgG response against food allergens, and additional studies are needed to confirm and explain this phenomenon. The use of a randomly selected group of patients with non-CRS from the general population as a control group would be of benefit in future investigations.
Our study has some limitations, namely a relatively small sample size from a single institution, the use of patients waiting for septoplasty as controls, and a high percentage of CRSwNP under inhalant steroids, which can bring together some bias to interpretation of immunological parameters. Nonetheless, patients were taking a combination of inhaled steroids with long-acting β2-agonists that allows asthma control at lower corticosteroids doses, with negligible systemic side effects. 42
In conclusion, our findings suggest that food allergy does not have an important role in CRSwNP etiopathogenesis, neither through IgE-mediated mechanisms nor through IgG-mediated hypersensitivity. Moreover, we observed a suppression in development of IgG sensitization against food allergens in patients with CRSwNP, which may be related to deviated IgG responses against other important targets (eg, airborne particles). Supporting this theory is the fact that an IgG1 subclass switching was observed in patients with CRSwNP and its values were negatively correlated to the sum of food-specific IgG concentration values.
Footnotes
Authors’ Note
Rafaela Veloso-Teles contributed to study design, data collection, statistical analysis, discussion, and revision. Rui Cerejeira, Rosa Farinhaand, and Christian von Buchwald contributed to study design, discussion, and revision. Débora Rodrigues did data collection and revision. This study was performed according the principles of the Declaration of Helsinki. The work was performed at Cova da Beira Hospital Centre.
Acknowledgments
The authors thank Conceição Faria, MD, director of clinical pathology department of Cova da Beira Hospital Centre, for laboratory availability for this investigation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.