
Abstract
This study aims to determine the benefit of stapes surgery for otosclerosis in 121 patients with a mixed hearing loss and a preoperative bone conduction (BC) threshold >30 dB. Average postoperative air conduction (AC) improved from 61.5 dB to 34.3 dB. Average air–bone gap closed from 27.1 dB to 6.1 dB. Bone conduction improved from 34.3 dB to 28.2 dB, with 38% of patients achieving a postoperative AC of <30 dB. Glasgow Benefit Inventory scores showed significantly increased quality of life postoperatively in the 88 patients who responded to follow-up, with an average score of 56. There was a mean reduction in daily hearing aid use postsurgery of 5.48 hours, with 56% of patients who responded to follow-up questionnaire no longer needing to use one. When assessing suitability for stapes surgery, surgeons should consider that preoperative BC thresholds may be a poor indicator of the true cochlear reserve and therefore the potential for improvement in AC thresholds and quality of life.
Introduction
Otosclerosis is a condition that affects up to 2% of the population clinically. 1 It is caused by bone remodelling in the otic capsule, 2 leading to a conductive hearing loss with elevated air conduction (AC) thresholds. However, some patients with otosclerosis demonstrate elevated bone conduction (BC) thresholds, implying that there is a sensorineural component in their hearing loss, where otosclerosis has caused poor cochlear function. Importantly though, the Carhart effect 3 is seen in otosclerosis, where an artificial exaggeration in BC thresholds can underestimate the patients’ cochlear reserve. This is seen across all frequencies but particularly at 2 kHz 4 with improvement in BC seen after correcting the cause of the conductive loss. Patients with BC thresholds of >30 dB have not traditionally been considered good candidates for otosclerosis surgery, even if their air–bone gap (ABG) is >25 dB, 5 due to the perceived lack of benefit and persistent need for a hearing aid.
Since the treatment options for otosclerosis-related hearing loss are hearing aids versus stapes surgery, traditional candidacy for stapes surgery would be patients in whom the aim would be to bring them out of hearing aid territory, 6 whereby if an outcome of better than 30 dB in each ear, or 15 dB difference between the 2 ears, is not considered achievable, patients may not benefit. However, it is known that BC measurement can be artificially elevated in patients with otosclerosis preoperatively, which brings into question the validity of this traditional candidacy selection.
Current treatment options for otosclerosis patients are: AC hearing aid use, BC implantation, a combination of stapes surgery and hearing aid use, stapes surgery alone, or in cases of profound hearing loss cochlear implantation may be considered. We aimed to address 2 questions in studying a subgroup of patients with average BC >30 dB: Does a high BC threshold mislead the preoperative assessment for stapes surgery in view of the Carhart effect? Are patients with BC threshold >30 dB good candidates for stapes surgery if hearing aids can be discarded and quality of life (QOL) improved?
This study uses a validated tool, the Glasgow Benefit Inventory (GBI), 7 alongside audiometric data and data on hearing aid use to assess the person-centred QOL improvements conferred by stapes surgery on patients with preoperative BC >30 dB.
Patients and Methods
It is a retrospective study with quality-of-life outcomes measured by questionnaire. One hundred twenty-one consecutive patients were included with otosclerosis who had stapes surgery by the senior author between 2013 and 2017 with presurgical BC pure-tone averages of between 30 dB and 40 dB. The mean age of participants was 49.65 years (ranging from 18-88). Ninety-four females were included and 27 males (M:F ratio = 3.48:1). All 121 patients were included in audiometric analysis. Quality of life follow-up postoperatively was attempted in all patients, the only exclusion criterion was if patients could not be contacted by phone or letter. Of the 121 patients originally identified, 87 responded to QOL follow-up (a 72% response rate), which was undertaken at least 6 weeks postprocedure. In these patients QOL was assessed using GBI, and hours of hearing aid use pre and postsurgery.
Audiometry was collected minimum of 6 months preoperatively and 6 weeks postoperatively with pure tone averages measured at 0.5, 1, 2 and 3 kHz (in accordance with American Academy of Otolaryngology—Head and Neck surgery guidelines), 8 and results obtained for BC, AC, and ABG. The measurements were collected using the recommended procedure from the British Society of Audiology. 9 At a preoperative clinic appointment, candidates were also routinely tested with tuning fork for reversed Rinne test at 256 and 512 Hertz.
Glasgow Benefit Inventory is a validated QOL questionnaire, comprising of 18 questions, used to assess outcomes from Ear, Nose and Throat procedures. Patients use a Linkert scale to rank each question from 1 to 5, where 1 is a very poor outcome, 5 is a very good outcome, and 3 is no change. The responses are then scaled where an outcome of 5 on every question correlates to +100, and 1 on every question correlates to −100. 7
Stapedotomy was routinely performed under local anaesthesia, 10 using a SMart 360 nitinol fluoroplastic piston (Gyrus ACMI, Inc; Southborough, Massachusetts) to reconstruct the ossicular chain. A potassium titanyl phosphate laser was used for complete posterior crurotomy, as a crucial step in the surgery. 11 Postprocedure hearing was assessed using clinical voice testing, after the tympanic membrane was replaced.
Results
Audiometry
Postoperative ABG was improved in 95.04% (n = 115) of patients, with a significant change of 21.0 dB (Figure 1). Of all, 57.02% (n = 69) of patients achieved a postsurgical AC better than their presurgical BC (overclosed). The highest percentage of overclosure (67.7%, n = 82) was seen at 2 kHz, which aligns with the Carhart notch, where the average postsurgical AC was 6.3 dB lower than presurgical BC. Also, 2 kHz showed the largest improvement (mean: 9 dB) in BC postoperatively (Table 1).
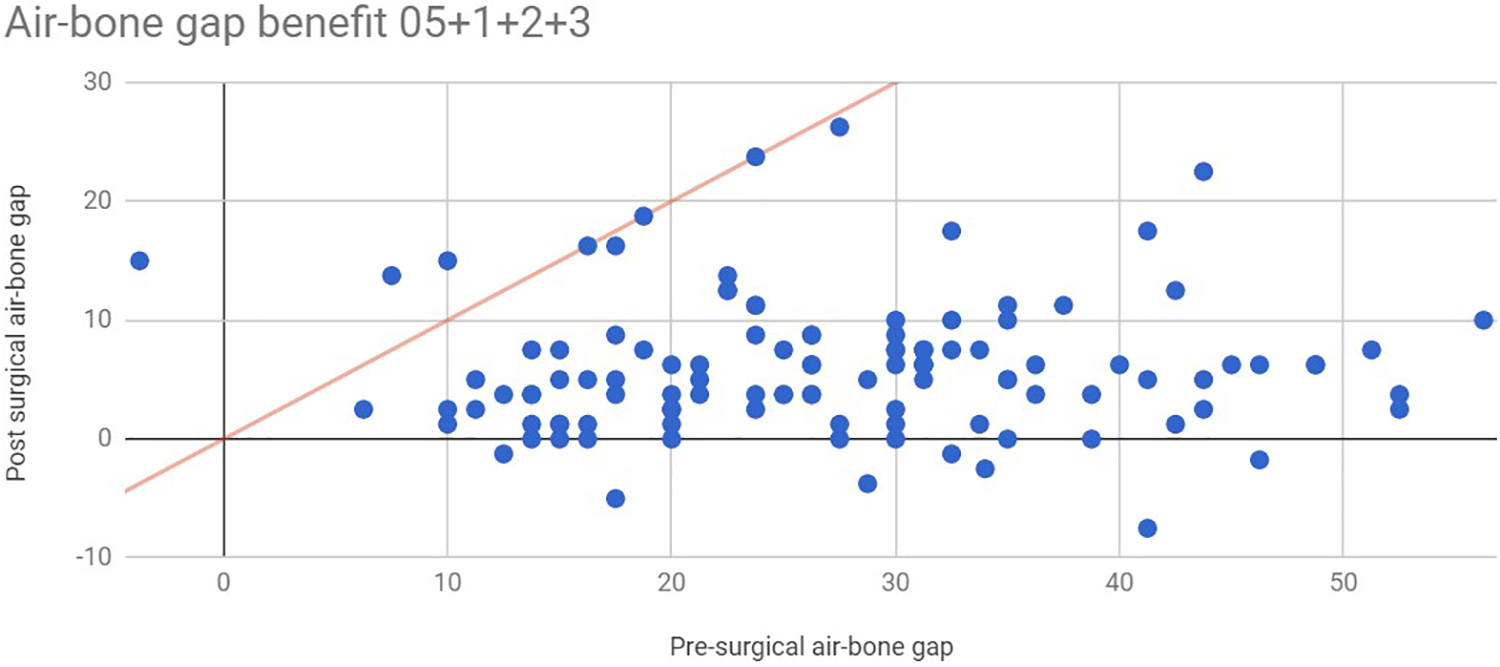
A graph showing pre and postoperative change in air–bone gap (ABG). Each dot represents a patient and the red line represents no change between pre and postoperative ABG.
Table Showing AC and BC Thresholds Pre and Postsurgery, and Comparisons.
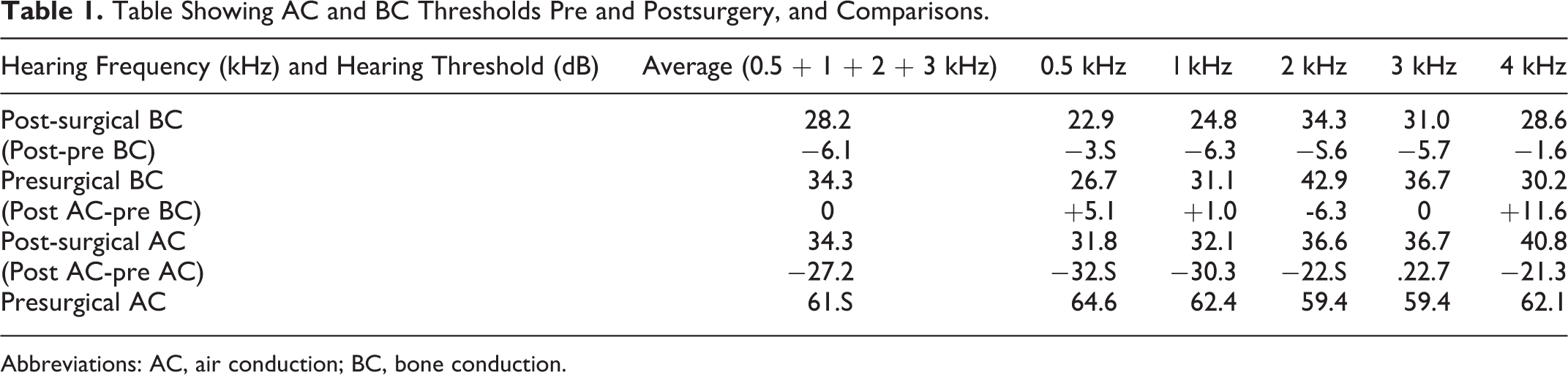
Abbreviations: AC, air conduction; BC, bone conduction.
In this cohort of patients, the mean apparent (preoperative) ABG was 27.1 dB, however the proven ABG (preoperative AC–postoperative BC) was 33.2 dB. Three patients showed no change in ABG postoperatively, and 3 showed a decrease postoperatively.
Of all, 72.5% of patients showed a postoperative improvement in BC, with 64% showing improved BC thresholds to better than 30 dB after surgery (Figure 2). The average improvement in BC thresholds was 6.1 dB: from 34.3 dB to 28.2 dB postsurgery. As expected, the largest decrease in postsurgical hearing thresholds was AC where there was an average decrease in 27.2 dB from 61.5 dB to 34.3 dB. An improvement in AC thresholds were demonstrated across all frequencies on average.
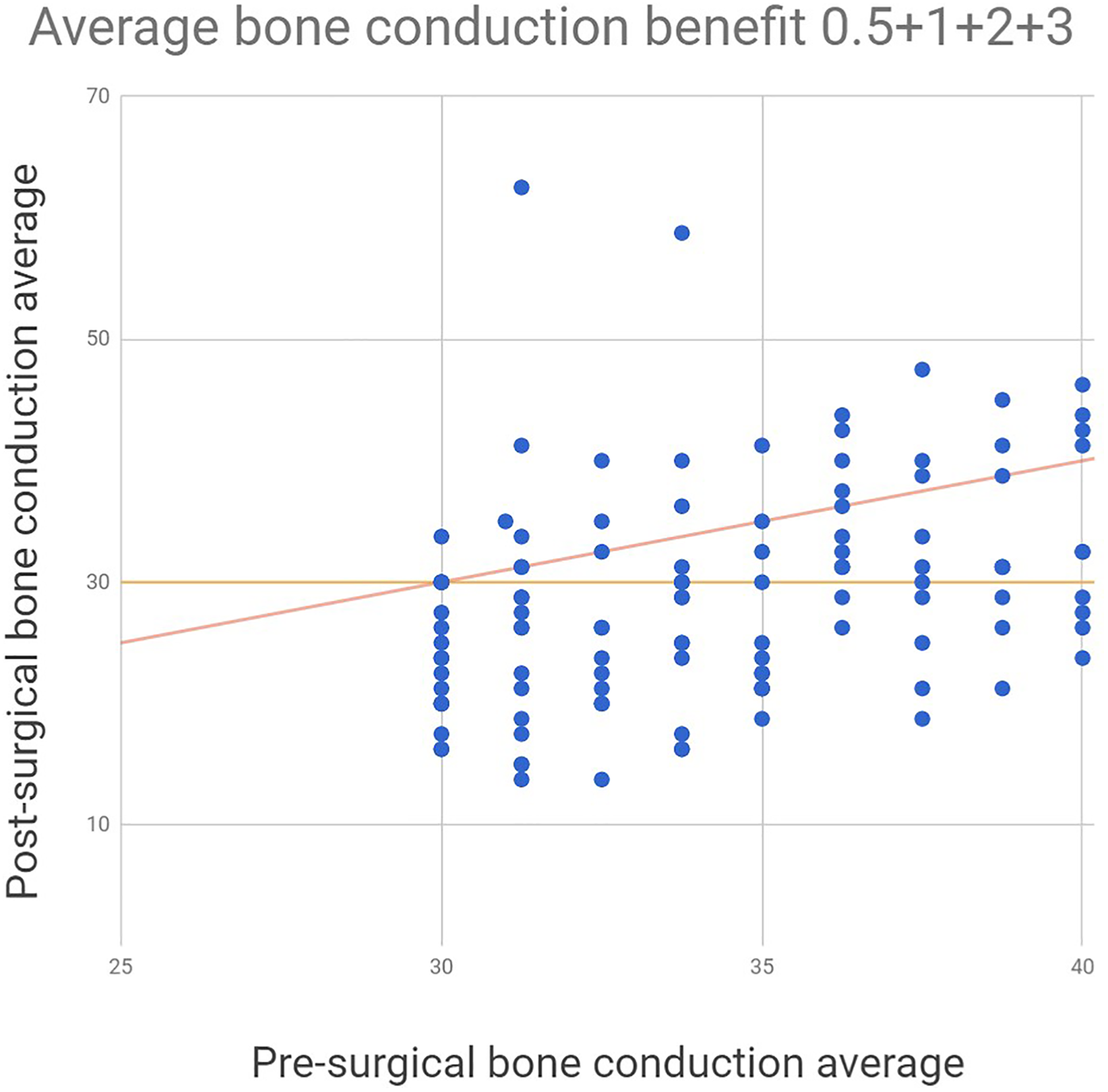
A graph showing pre and postoperative change in mean bone conduction (BC) thresholds. Each dot represents a patient and the red line represents no change between pre and postoperative BC threshold.
One patient had profound hearing loss postoperatively with the average AC conduction threshold increasing from 27.5 to 77.5 dB.
Quality of Life
A total of 95.4% of patients reported an increase in their GBI score, with 83.9% reporting a significant increase in their GBI scale of >30 (Figure 3). The average GBI score was +56. 5.
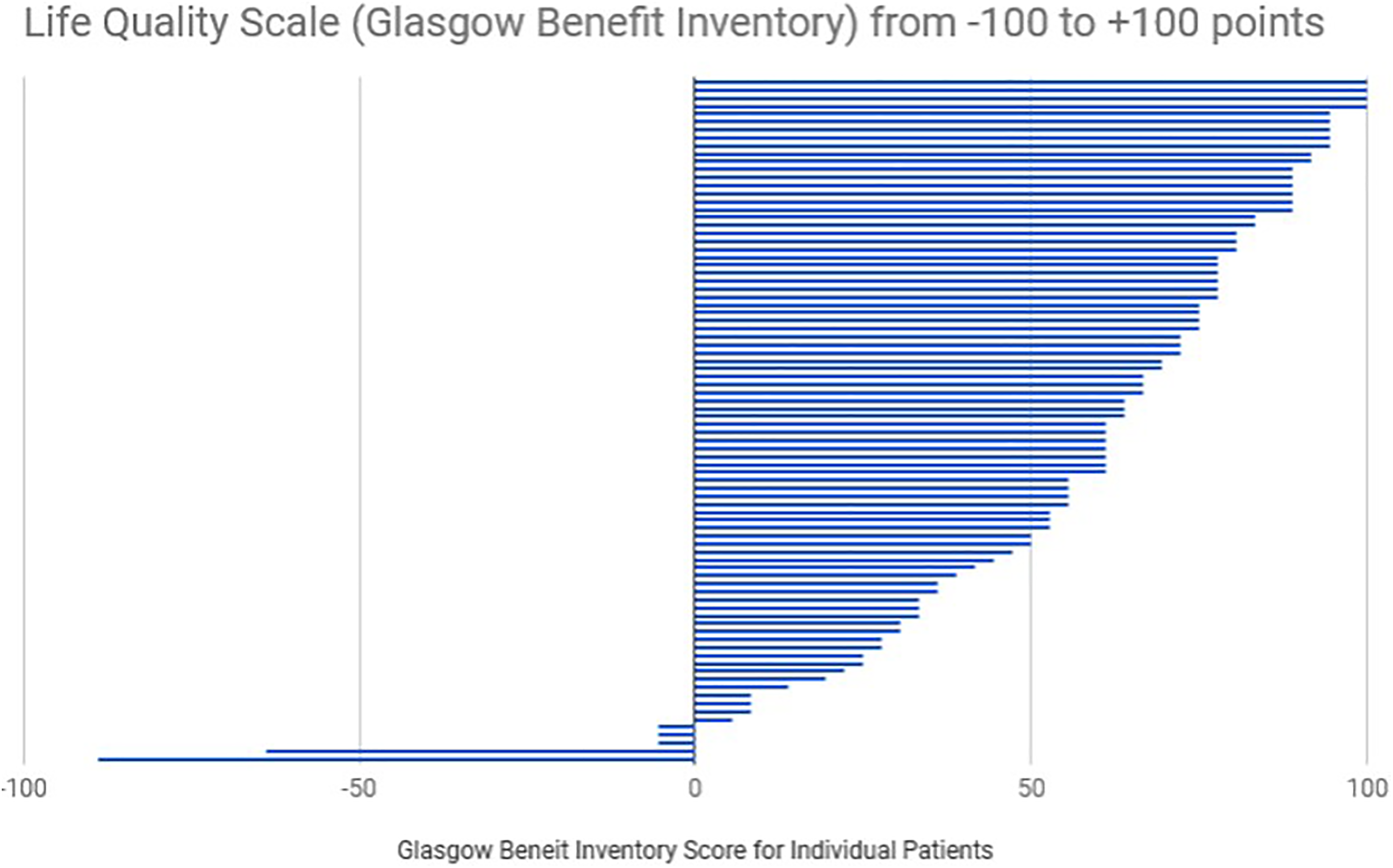
A bar chart showing Glasgow Benefit Inventory results from all patients that responded to quality of life follow-up.
Only 5.7% (5) patients saw a decrease in their QoL points: One patient had a prosthetic piston that was too long and needed revision, following which they had severe sensorineural hearing loss and tinnitus. One patient initially had excellent hearing postoperatively, however hearing became worse over the following year—thought to be caused by further adhesions in the middle ear (which were identified and divided by laser intraoperatively). One patient was found to have an eroded long process of the incus intraoperatively which was built up using OtoMimix bone cement. Two patients had no operative complications and initial audiometric thresholds showed postoperative improvement—a clear explanation of their perceived hearing problems could not be found.
Hours of Hearing Aid Use
Forty-nine (56%) patients went from using a hearing aid to not needing one following surgery (Figure 4). Mean hearing aid use presurgery was 6.52 hours a day compared to 0.93 postsurgery. Two patients went from never needing a hearing aid, to using one. However, both patients had no operative complications and initial audiometric thresholds showed postoperative improvement.
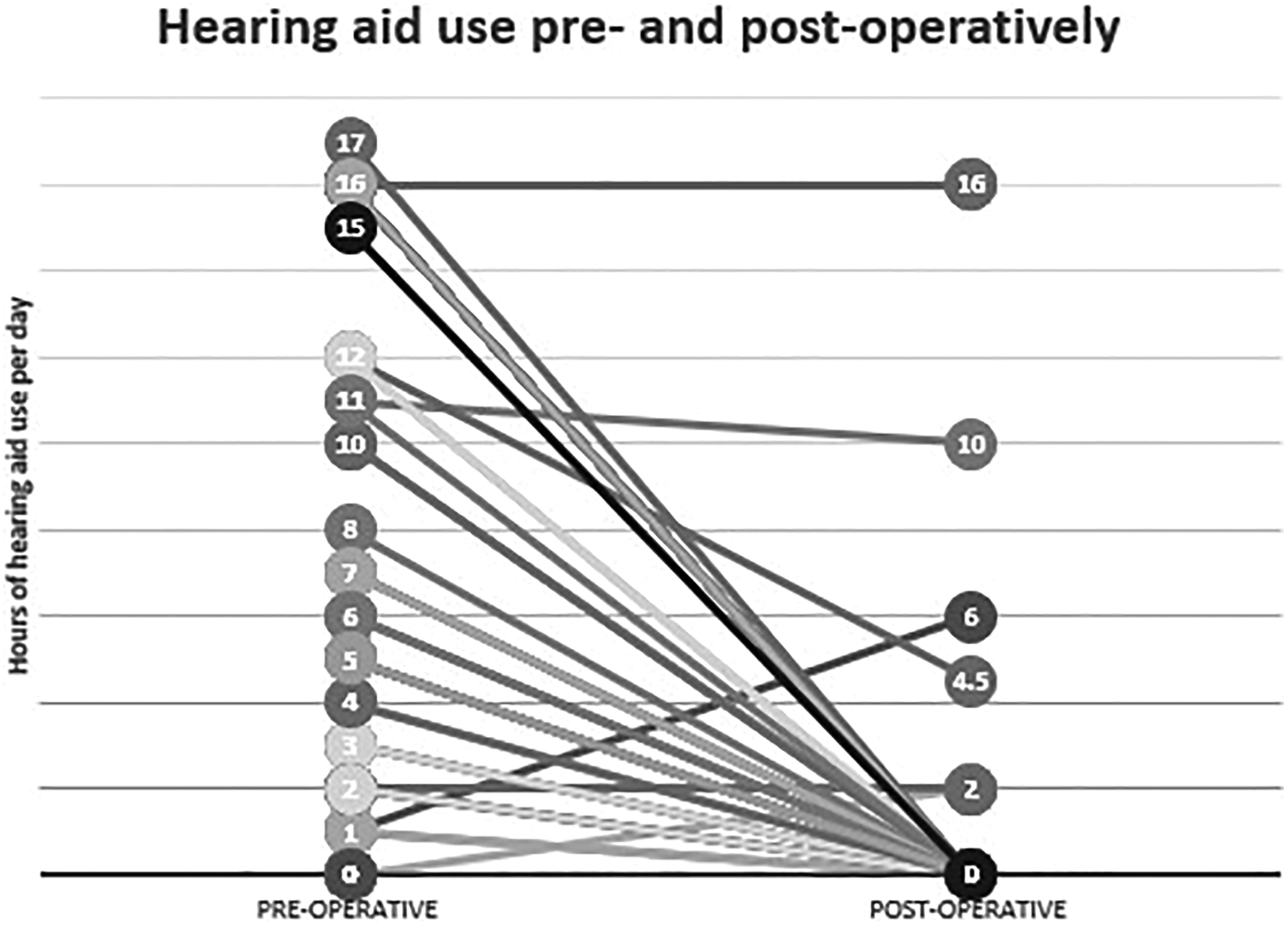
A graph showing how hours of hearing aid use per day has changed pre and postoperatively for patients.
Discussion
Audiometry and the Carhart Effect Misleading Preassessment Findings
All patients in the study had a preoperative BC threshold of 30 to 40 dB, and a mean raised ABG of 27.1 dB preoperatively (Table 1). However, we have been able to show that this is, at least in part, due to the Carhart effect underestimating the patients’ cochlear reserve. This has been demonstrated by the fact that postoperative AC thresholds became better than that of the preoperative BC threshold (overclosed; Table 1). This would have been impossible if the BC was a representation of the true cochlear reserve in these patients. This has been further demonstrated by the pure-tone averages for BC thresholds in our patients improving by 6.1 dB on average postoperatively.
The highest percentage of overclosure (67.7%, n = 82) was seen at 2 kHz, which aligns with the Carhart notch. Also, 2 kHz showed the largest threshold improvement (mean: 9 dB) in BC postoperatively.
Therefore, our cohort demonstrated an overestimation of their sensorineural hearing loss preoperatively due to the Carhart effect, and the BC thresholds should not be relied upon for an accurate representation of true cochlear reserve.
We have also been able to show the unreliability of preoperative ABG measurements, with a 6.1 dB mean difference between the apparent and proven ABG. The large disparity between these measurements show that these patients have an underestimated ability for AC improvement and ABG closure postoperatively.
As previously mentioned, patients with BC thresholds of >30 dB are not traditionally considered good candidates for otosclerosis surgery, even if their ABG is >25 dB. 5,6 However, this study suggests that candidates for surgery 6 should be considered in the context of a potential Carhart effect. The mean postoperative BC threshold for our patient group was 28.2 dB.
We anticipate that our results obtained at 6 weeks are, if anything, an underestimate of final hearing thresholds and should continue to improve further in the postoperative period. 12
Quality of Life and Hearing Aid Findings
In the United Kingdom, current management of otosclerosis is centred between AC hearing aid use and stapes surgery. Aside for the cost of providing patients with hearing aids before or at the same time as stapedotomy there are also QOL considerations. It is recognized that patients find getting used to hearing aids difficult, 13 including perceived stigma attached, reduced self-confidence 14 and a seeming acceptance to oneself of aging. 15
The GBI score uses a validated questionnaire 7 to assess QOL after surgery and includes questions such as whether patients feel more confident at work and during social interactions, more independent and less likely to need the help of their relatives or their doctor since having the operation. In this study, we have seen 95.4% of patients reporting an increase in their GBI score, with 83.9% reporting a significant increase in >30. In addition, 56% of patients went from using a hearing aid to not needing one after surgery.
Some patients who stopped using a hearing aid postoperatively still had an AC threshold above 30 dB, which would often require hearing aid use. We believe that the decision by patients to not wear hearing aids postoperatively is likely multifactorial. Patients often report finding them a hassle to wear, with cosmetic impacts on self-image, along with practical impacts such as maintainance. 13 Wearers also report an unpleasant occlusion effect from using hearing aids, where the aid occludes the ear canal and increases the volume of the wearers voice in the lower frequencies. 16 Finally, we believe that patients’ listening skills have likely enhanced during their time with worse hearing, and as a result are able to hear well at thresholds other may find difficult.
With such a demonstrated positive effect on QOL and a reduced need for hearing aid use, we would recommend that surgeons wait to see patients’ postoperative results before recommending a form of hearing aid, even when preoperative BC is >30 dB.
Clinical Applicability and Conclusion
This study demonstrates that otosclerosis patients with a BC threshold >30 dB have improved audiometric data poststapedotomy, an improved QOL overall, and a decreased need to wear hearing aids. Many patients in this nontraditional candidate group choose to discard their hearing aid postoperatively and this should be considered when counselling patients for surgery. When assessing suitability for stapes surgery, surgeons should consider that preoperative BC thresholds may be a poor indicator of the true cochlear reserve and therefore potential for surgical benefit.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.