
Abstract
Objective:
To examine the clinical factors associated with the effectiveness of stapedotomy in improving hearing sensitivity in Taiwanese patients with otosclerosis.
Methods:
In this retrospective study, we reviewed the medical records of 31 patients (36 ears) with otosclerosis undergoing stapedotomy performed by a single surgeon. Preoperative and postoperative hearing results were analyzed to identify factors associated with hearing outcomes after stapedotomy in the Taiwanese population with clinical otosclerosis.
Results:
Compared with preoperative pure tone averages (PTAs), stapedotomy significantly improved postoperative air conduction (AC) thresholds (P < .0001), bone conduction (BC) thresholds (P = .025), and air-bone gaps (ABGs; P < .0001). Postoperative closure of ABGs less than 10 or 20 dB was achieved in 16 (44.4%) and 33 (91.7%) of 36 surgical ears. Improvement in postoperative AC thresholds and ABGs and the size of preoperative ABGs were significantly correlated (r = .650, P < .001 and r = .745, P < .001, respectively). Gender-stratified analysis indicated a stronger correlation between improvement in postoperative AC thresholds and preoperative ABGs in male patients than in female patients (r = .893, P < .001 and r = .476, P = .014, respectively), and in postoperative and preoperative ABGs (r = .933, P < .001 and r = .626, P < .001, respectively). With the more stringent criteria for surgical success, factors including age (≤50 years), type (conductive, BC ≤25 dB), and degree (PTA ≤55 dB) of preoperative hearing loss led to more favorable outcomes.
Conclusions:
We reported evidence supporting a potential gender difference on hearing outcomes after stapedotomy in Taiwanese patients with otosclerosis. Age, type, and degree of preoperative hearing loss may affect the surgical success rate.
Introduction
Otosclerosis is a hearing disorder resulting from an increasing bone remodeling activity in the remains of the embryonal otic capsule. 1 -5 Clinically, most patients manifest as progressive conductive hearing loss due to stapedial fixation. Some patients develop a mixed hearing loss due to extension of the disease to the cochlear endosteum and spiral ligament 6 that releases proteolytic enzymes into the inner ear. 5,7 Isolated sensorineural hearing loss is exceptional. 8 -10 Approximately one-third of patients with otosclerosis demonstrated a clinical progression of the sensorineural component of hearing loss, 11 and the incidence of vertigo also increased with the duration of hearing loss. 12 Since the introduction of stapedotomy, 13,14 surgical approach has become the primary treatment of conductive hearing loss in otosclerosis. 15
The clinical prevalence of otosclerosis is estimated to be 0.3% to 0.4% in Caucasians. 16 However, histologic otosclerosis identified in temporal bone studies is significantly higher at 2.5% to 12%. 5,16,17 Epidemiological studies showed an ethnic difference in the occurrence of otosclerosis, with the reported incidence of clinical otosclerosis is higher in Hispanics and Caucasians 18 than in Asian 19 and African populations. 20 One population-based study 21 depicted the peak incidence rate in 1970s. After 1970, the incidence of otosclerosis declined. Similarly, due to its low prevalence in Asian population, 22 reported series of stapedotomy for Asian patients with otosclerosis were limited. 23
The etiology of otosclerosis is multifactorial. Previous studies 3,24,25 suggested genetic and environmental predispositions to this abnormality. A recent systematic review 2 enumerated several factors, including genetic, 26 viral, autoimmunity, inflammatory, hormonal, and metabolic mechanisms, that may contribute to the pathogenesis of otosclerosis. Notably, the previous studies 3,12,17,27 also showed that otosclerosis occurs approximately twice more frequently in women than in men. Often, hearing loss is rapidly progressive during pregnancy. However, the etiological role of hormonal substances, namely estrogen, and the gender effect on the hearing outcomes of the stapedotomy has yet to be confirmed. 28 In this study, we retrospectively examined the effectiveness of stapedotomy in improving hearing sensitivity of otosclerotic patients in a Taiwanese population, with an emphasis on the potential effect of gender and other factors on postoperative functional outcomes.
Materials and Methods
This single-center retrospective study was approved by the local institutional review board (CTH-107-3-5-019). Medical records of all patients undergoing primary stapedotomy for clinical otosclerosis at our institution from January 2008 to December 2018 were reviewed.
Data Collection
The data analyzed included patient demographics (age, sex, race) and clinical characteristics. Operative details including operated ear, technique used, findings, complications, and preoperative and postoperative audiometric data were recorded. Postoperative results from audiograms were used as outcome measurements.
Audiometric Evaluation
Audiometric tests were performed using standard procedures in a double-walled soundproof room. Pure tone averages (PTAs) were used as a surrogate for overall hearing sensitivity. Pure tone averages were calculated as the mean thresholds (in dB HL) at the frequencies of 0.5, 1, 2, and 4 kHz in both ears. Both air conduction (AC) and bone conduction (BC) thresholds were routinely evaluated. Air-bone gap (ABG) was calculated by using same time AC and BC measurements. Audiograms were obtained at preoperative and postoperative available follow-up visit. The postoperative audiogram PTAs and ABGs were compared with the preoperative audiogram ones to calculate the change as a hearing outcome of the stapedotomy in the operated ear. Surgical success, as defined by the AAO-HNS, is a postoperative ABG of 10 dB or less. In the study, we used both cutoff values at 10 and 20 dB for the definition of surgical success.
Surgical Procedures
All procedures were performed by a single surgeon (Kai-Nan Lin) via an endaural or postauricular approach under general anesthesia. After local anesthesia infiltration, a posterior superior tympanomeatal flap was incised and raised to expose the middle ear space. The overhanging posterior tympanic bone was then drilled or curetted for full visualization of the stapes, oval window, footplate, and facial canal. Subsequently, the stapes were inspected and palpated to confirm the diagnosis of otosclerosis. The posterior and anterior crura of the stapes were weakened with a diamond burr. The distance between the footplate and the incus is measured. A 0.6-mm fenestra is drilled in the central portion of the footplate using a Skeeter drill. An appropriate size of titanium piston is then inserted into the fenestra and tightened to the long process of the incus. Following prosthesis insertion, stapes superstructure was removed by separating the incudostapedial joint and cutting the stapedial tendon, the mobility of the ossicular chain rechecked, the tympanomeatal flap replaced to its original position. The canal is packed with Gelfoam soaked in Ofloxacin otic drops, and the incision was closed with 4-0 Vicryl suture.
Statistical Analysis
Descriptive statistics were used to characterize the data. Due to the small sample size, nonparametric methods were used. Preoperative and postoperative PTA values of 0.5, 1, 2, and 4 kHz and pure tone thresholds for AC, BC, and ABG were compared using the Wilcoxon signed-rank test, respectively. Correlation between preoperative audiological parameters and postoperative improvement in AC thresholds and ABGs were analyzed using Pearson correlation. Potential factors associated with surgical success (postoperative ABG of ≤10 or ≤20 dB with or without an AC ≤30 dB) were analyzed using Fisher exact test. Significance was set at P ≤ .05. IBM SPSS Statistics Version 25 (IBM SPSS Statistics) was used for all analyses.
Results
A total of 31 patients (36 ears) underwent stapedotomy with surgically confirmed otosclerosis by a single surgeon. Demographic and clinical characteristics of the patients are shown in Table 1. The mean age of the study group was 51, ranging from16 to 75 years. Among all patients, 23 (26 ears) were female. The study population included more mixed type hearing loss (55.6%, 20/36) than conductive hearing loss (44.4%, 16/36). The majority of the operated ears (77.8%, 28/36) had a moderate or moderate-to-severe degree of preoperative hearing loss. The median follow-up time was 3.5 months (range 2-16 months).
Baseline Characteristics of the Study Population.
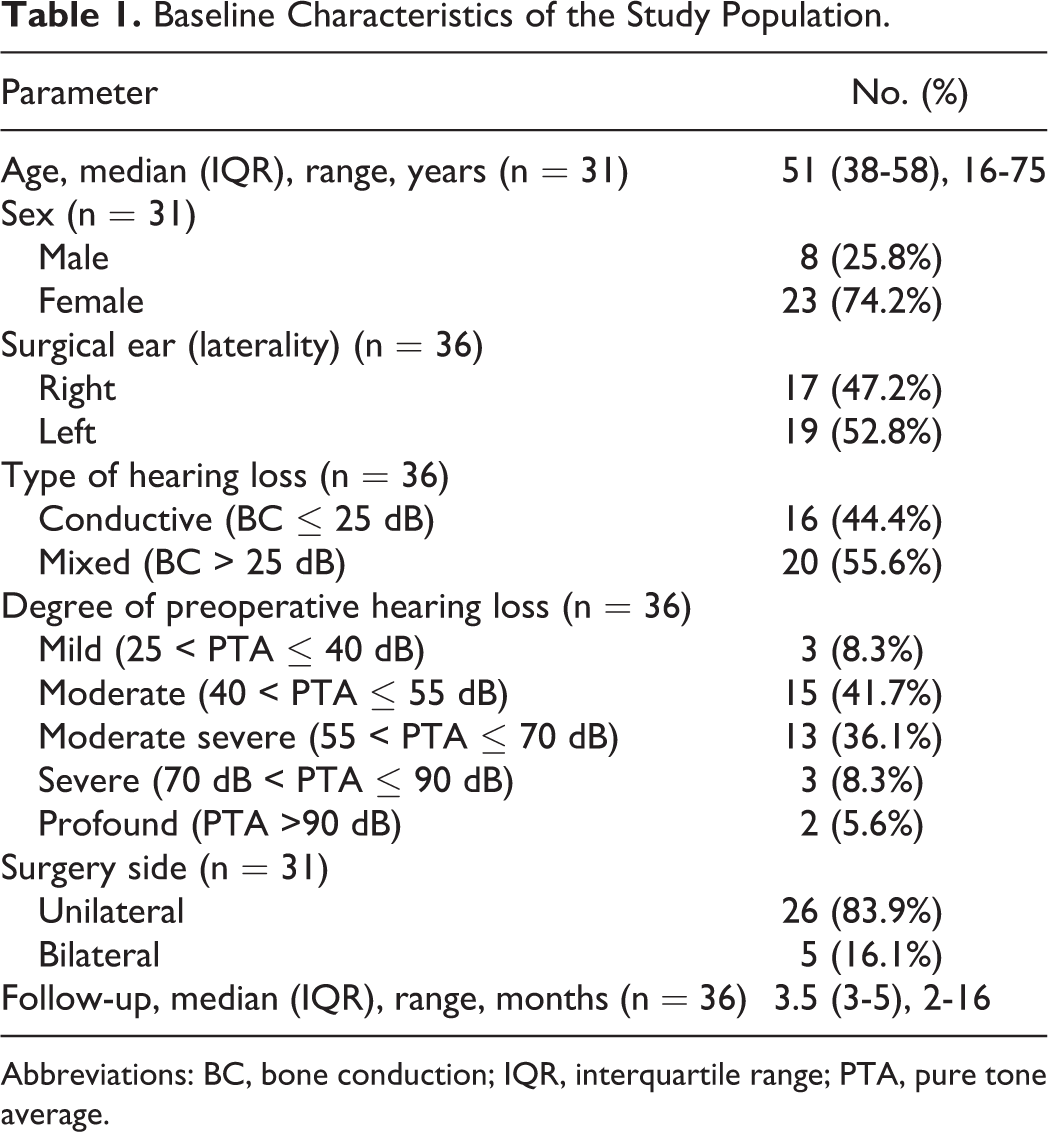
Abbreviations: BC, bone conduction; IQR, interquartile range; PTA, pure tone average.
Compared with preoperative PTAs, stapedotomy led to a significant improvement in postoperative AC thresholds (P < .0001), BC thresholds (P = .0248), and ABGs (P < .0001; Figure 1). Postoperative measurements of AC thresholds, BC thresholds, and ABGs as a function of frequency were significantly lower (all P < .001; Figure 2). Overall, 16 (44.4%) and 33 (91.7%) operated ears achieved an ABG of ≤10 and ≤20 dB, respectively. Adding postoperative AC thresholds of 30 dB or less in the success criteria, the success rate declined significantly (8/36, 22.2% and 14/36, 38.9%, respectively; Table 2). Significant correlation was found between improvement in postoperative AC thresholds (Figure 3A) and ABGs (Figure 4A) and the size of preoperative ABGs (r = 0.650, P < .001 and r = 0.745, P < .001, respectively). Gender-stratified analysis depicted a stronger correlation between improvement in postoperative AC thresholds and preoperative ABGs (r = 0.893, P < .001 and r = 0.476, P = .014, respectively) in male patients than in female patients (Figure 3B and C). Likewise, correlation between improvement in postoperative ABGs and preoperative ABGs was stronger in male patients than in female patients (r = 0.933, P < .001 and r = 0.626, P < .001, respectively; Figure 4B and C). Further analysis showed that the baseline preoperative hearing thresholds including AC thresholds, BC thresholds, and ABGs were of no significant difference between genders (Supplemental Tables 1 and 2). With the more stringent criteria for surgical success, factors including age (≤50), type (conductive, BC ≤25 dB), and degree (PTA ≤55 dB) of preoperative hearing loss led to more favorable outcome (Table 2). No patient exhibited sensorineural hearing loss or other adverse complications following stapedotomy.
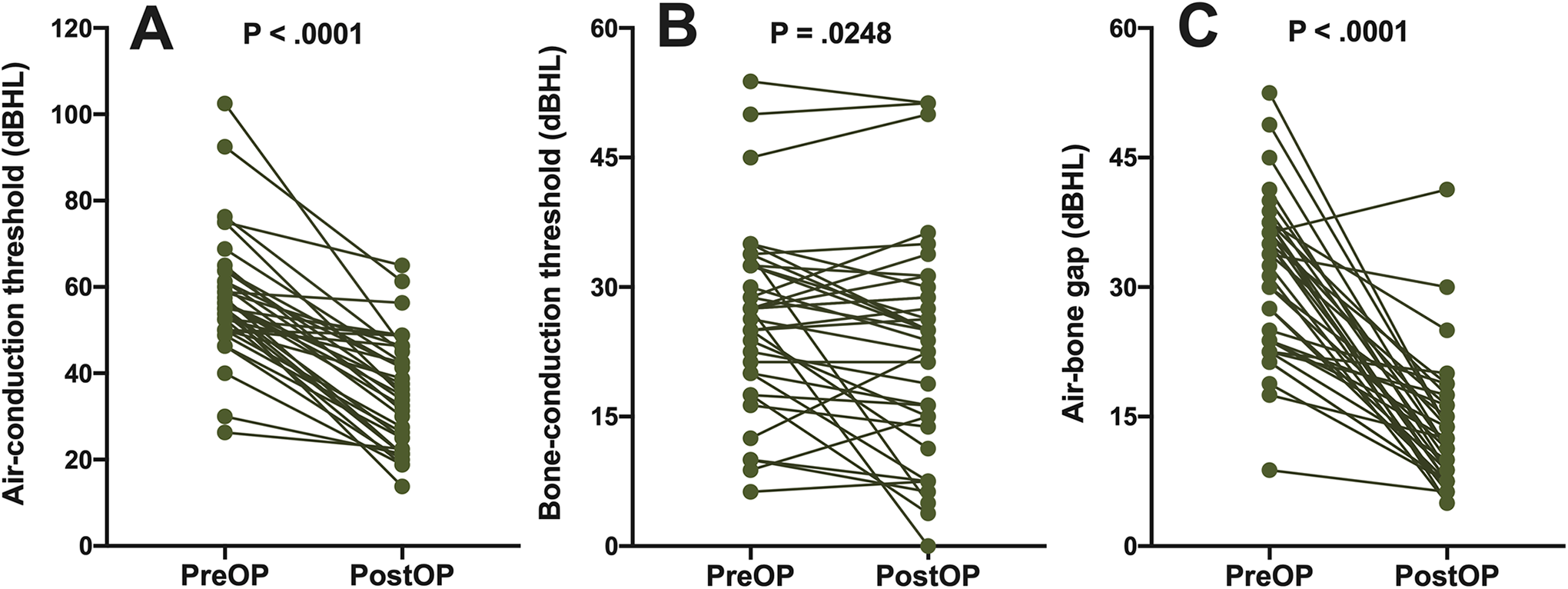
Preoperative and postoperative air conduction (A), bone conduction (B) pure tone average thresholds, and air-bone gap (C) for stapedotomy. dB HL indicates decibel hearing level.
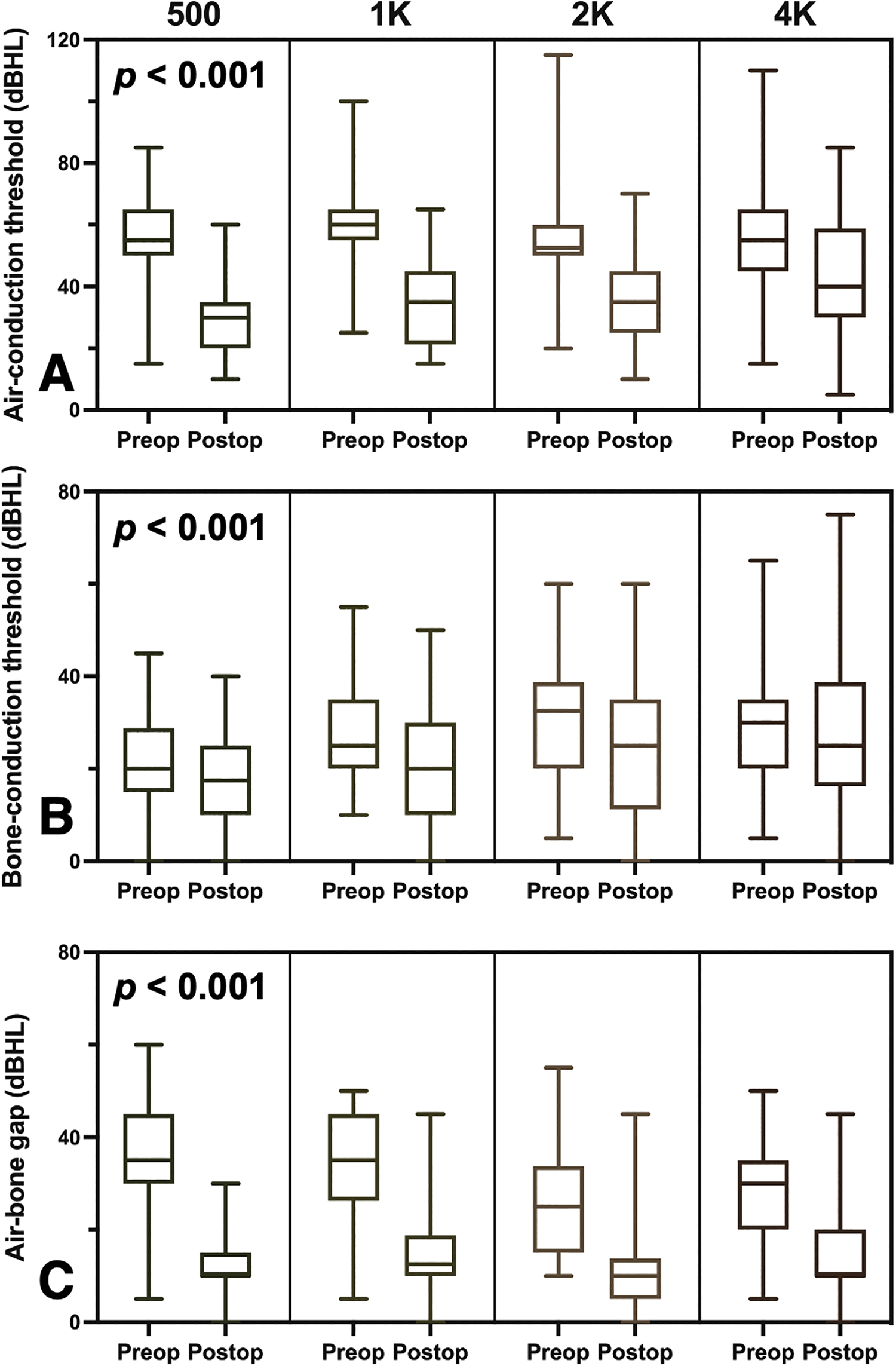
Preoperative and postoperative measurements of air conduction (A), bone conduction (B) pure tone average thresholds, and air-bone gap (C) as a function of frequencies of 0.5, 1, 2, and 4 kHz. Wilcoxon signed-rank test showed a significant difference in air conduction thresholds, bone conduction thresholds, and air-bone gap (all P < .001). dB HL indicates decibel hearing level.
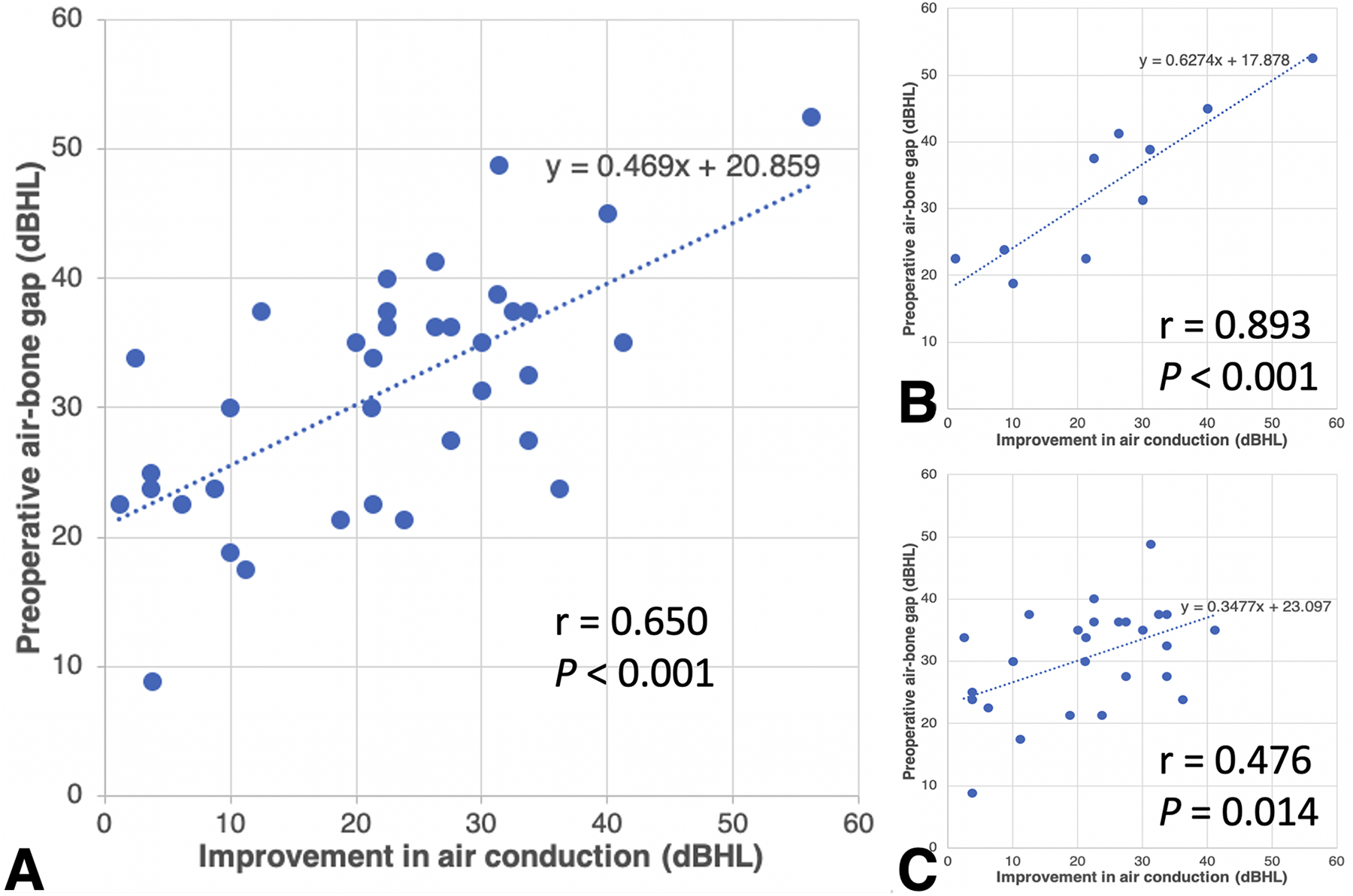
Significant correlation between improvement in postoperative air conduction (AC) thresholds (A) and the size of preoperative air-bone gaps (r = 0.650, P < .001). Subgroup analysis demonstrated a stronger positive correlation between improvement in postoperative AC thresholds and preoperative air-bone gap (ABGs) in male patients (B) than in female patients (C) (r = 0.893, P < .001 and r = 0.476, P = .014, respectively). The slope rate of the linear regression line is higher in male patients than in female patients (0.627 vs 0.348). dB HL indicates decibel hearing level.
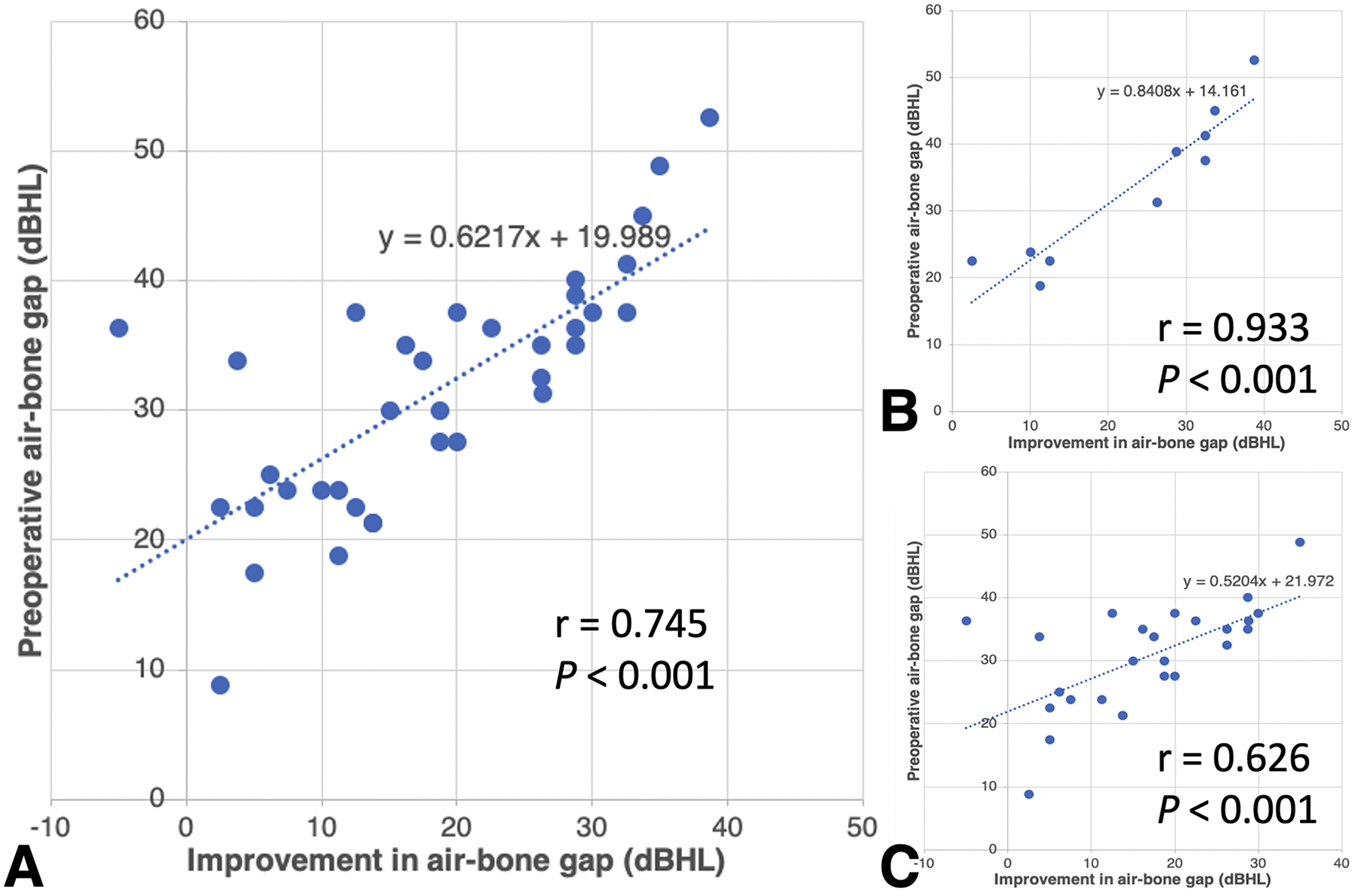
Significant correlation between improvement in postoperative air-bone gaps (A) and the size of preoperative air-bone gaps (r = 0.745, P < .001). Subgroup analysis demonstrated a stronger positive correlation between improvement in postoperative air conduction (AC) thresholds and preoperative ABGs in male patients (B) than in female patients (C) (r = 0.933, P < .001 and r = 0.626, P < .001, respectively). The slope rate of the linear regression line is higher in male patients than in female patients (0.841 vs 0.520). dB HL indicates decibel hearing level.
Subgroup Analysis According to Postoperative Success Rate.
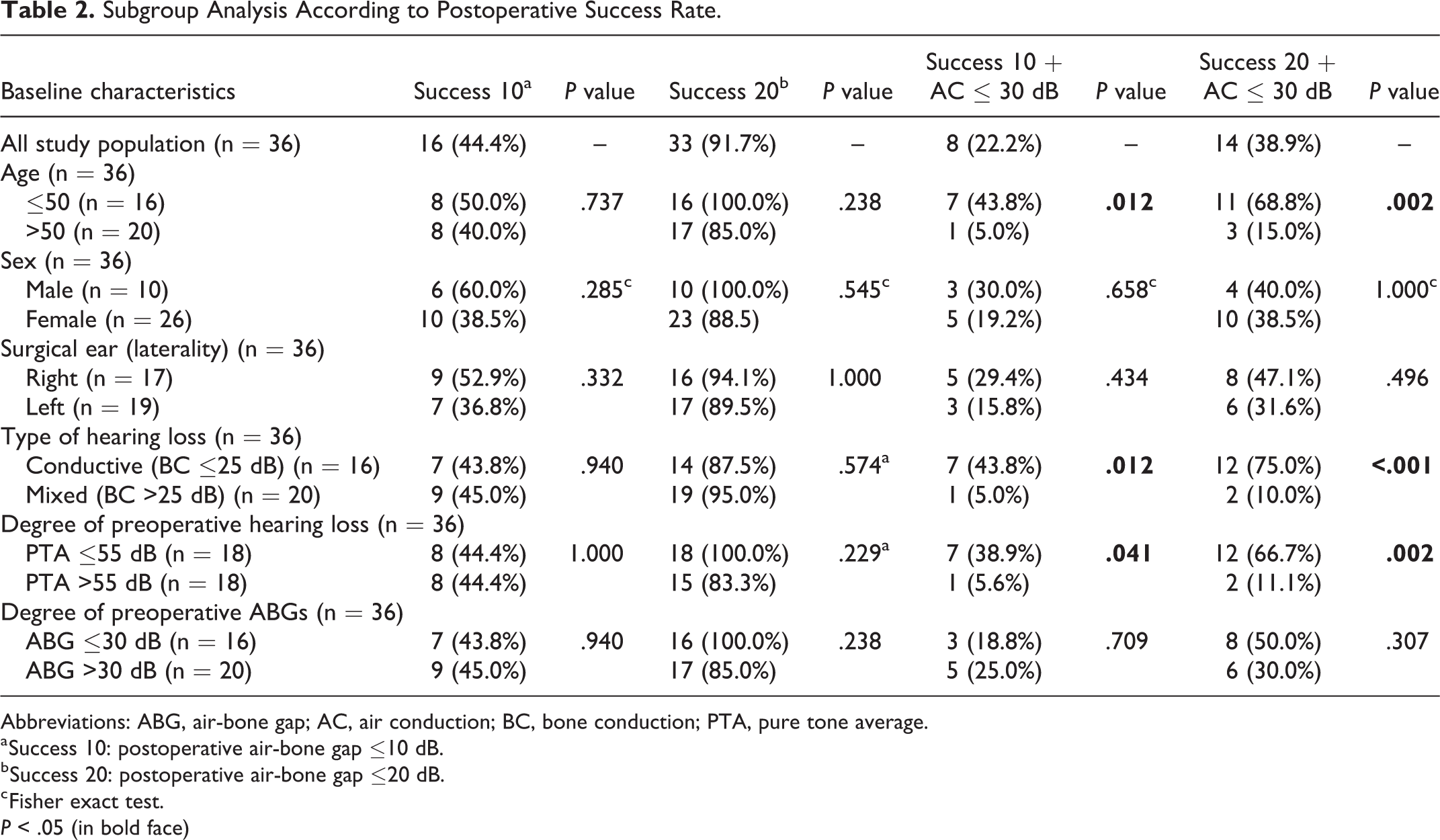
Abbreviations: ABG, air-bone gap; AC, air conduction; BC, bone conduction; PTA, pure tone average.
a Success 10: postoperative air-bone gap ≤10 dB.
b Success 20: postoperative air-bone gap ≤20 dB.
c Fisher exact test.
P < .05 (in bold face)
Discussion
This study confirms that stapedotomy is safe and effective procedure leading to improved hearing sensitivity for Asian patients with otosclerosis. Age, type, and degree of preoperative hearing loss may affect the surgical success rate. Male patients with otosclerosis demonstrated a stronger correlation between improvement in postoperative AC thresholds and ABGs and the size of preoperative ABGs. Hearing outcomes after stapedotomy seem to be more predictable in male patients than those in female patients. The discrepancy may help clinicians to recommend stapedotomy in patients of different genders with variable degree of preoperative hearing loss.
Otosclerosis occurs in 5% to 9% of all hearing losses and 18% to 22% of all conductive hearing losses 17,29 in Caucasians. By contrast, while the incidence of histological otosclerosis is comparable to that among Caucasians, the incidence of clinical otosclerosis is much lower in Asian countries. 22 According to the recordings of the National Health Insurance Research Database in Taiwan, approximately 100 cases of stapes surgery are performed each year. 23 This reflects an annual incidence rate of 0.0004%. Stapedotomy is considered a preferred surgical modality to correct the conductive hearing loss in this disorder. 30 Surgical success, as defined as a postoperative closure of ABG within 10 dB, are achieved in 70% to 90% of patients with otosclerosis in Caucasians. 29,31 -33 Although there is currently no direct comparison of hearing outcomes following stapedotomy among different ethnicities, individual Asian series demonstrated a lower success rate than that in Western Countries. 23 We report a surgical success rate of 44.4% (16/36) in our series. However, our suboptimal success rate (closure of ABG within 20 dB postoperatively) of 91.7% is comparable to other reports in the literature. 29,31 Adding postoperative AC thresholds of 30 dB or less in the success criteria, the success rate declined significantly. The relatively low surgical success rate after stapedotomy in our populations may be explained by a low incidence rate with limited surgeon experience, a small and tortuous external auditory canal with narrow surgical field, 23 the use of smaller diameter prosthesis, 34 and undetermined optimal surgical timing. 35
Only few studies reported both audiometric data and functional outcomes such as quality of life assessment in patients undergoing stapedotomy. Lailach et al 36 approached those patients receiving stapes surgery with audiometric evaluation and disease-specific questionnaires. Despite a good correlation between audiometric parameters and subjective hearing function, they identified that audiometric data alone were not a sufficient indicator for postoperative social and mental well-being. Currently, most stapes surgery studies reported “surgical” success only base on a postoperative ABG ≤10 dB, without consideration of other important patient-related issues, namely functional hearing outcomes, patients’ satisfaction, the impact on their quality of life, and long-term need for wearing a hearing aid. In our series, the success rate taking into account of postoperative ABG ≤10 and ≤20 dB was 44.4% and 91.7%, respectively. When we adopt more stringent criteria involving also a postoperative AC threshold ≤30 dB, the success rate declines significantly to 22.2% (8/36) and 38.9% (14/36), respectively. Which means theoretically, at least 61.1% of patients are eligible for hearing-aid assistance after the stapes surgery. Therefore, we suggest that, when reporting stapedotomy-related postoperative hearing gains, at least the incidence rate of postoperative AC threshold ≤30 dB should be incorporated into the criteria of surgical success rate in future studies to eliminate possible selective outcome reporting bias.
Although the beneficial effect of stapedotomy on hearing and the relatively low incidence of permanent complications have been confirmed in many studies, 32,37,38 individual series analyzing preoperative predictors for a successful hearing outcome have yielded inconsistent results. 23,33,37,39 -41 For example, preoperative size of ABG has been reported as an independent predictor for favorable surgical outcomes. Ueda et al, 41 Khorsandi et al, 33 and Yeh et al 23 reported that a smaller preoperative ABG was associated with a higher chance of better postoperative ABG closure. They attributed this phenomenon to round window involvement of the otosclerotic lesions that cannot be corrected by stapedotomy. 42 However, Virk et al 43 conducted a review regarding the role of imaging in the diagnosis and management of otosclerosis and concluded that the otosclerotic findings of the high-resolution computed tomography of the temporal bone beyond the oval window is associated with an increased risk of sensorineural hearing loss, instead of conductive hearing loss, which might result in smaller preoperative ABGs. In contrast, our data are more compatible with those from Marchese et al 40 and Bittermann et al 37 who demonstrated a significant correlation between preoperative ABG ≥30 dB and a higher postoperative hearing gain (≥10 dB). We suggested that this discrepancy was the result of various criteria that were used for surgical success. In addition, a smaller preoperative ABG might have a greater chance to achieve a postoperative ABG of ≤10 dB if we use this definition as the only criteria for surgical success.
Although our study did not show a significant difference in surgical success rate between those with preoperative ABG ≥30 dB and <30 dB, our results demonstrated a correlation between improvement in postoperative AC thresholds and ABGs and the size of preoperative ABGs, which indicated that a larger preoperative ABG is associated with a greater gain in postoperative AC thresholds and ABGs. Furthermore, subgroup analysis of this phenomenon revealed a gender difference. Although clinical otosclerosis has been confirmed to be a female predominant disease, gender effect on the surgical outcomes is still debated. Our data showed that based on comparable preoperative AC, BC thresholds, and ABGs, male otosclerosis patients exhibited a more predictable surgical outcome than female patients. Hormonal, 44 osteoporosis (bone metabolism), 45 or other genetic factors 26 in female patients with otosclerosis may cause variations in otic capsule pathology that subsequently influence the surgical results than those in male patients. Clinicians may use this result to inform patients more precisely about expected postoperative audiometric outcomes.
In Table 2, we demonstrated our changing results of clinical predictors for surgical success when using different criteria of surgical success. Considering functional outcomes, we suggested that more stringent criteria should be used, namely a postoperative ABG ≤10 dB and AC threshold of ≤30 dB. With this definition of surgical success, we were able to identify several favorable clinical predictors such as younger age (≤50 years), conductive hearing loss (instead of mixed type hearing loss), better preoperative AC thresholds (≤55 dB) in Taiwanese patients with otosclerosis counseling for surgical intervention.
Strengths and Limitations
The main strength of the study is that a single otologist performed all the surgeries. When evaluating the outcomes of stapedotomy, technical consistency would minimize confounders. However, several possible limitations should be addressed: first, a small sample size may limit the significance of some of the statistical comparisons conducted in the study. However, a post hoc analysis revealed a statistical power (1-β) of 1.00 based on the α level of .05, sample size, and calculated effect size in the study. Second, a wide range of follow-up time was observed, which may influence the reported outcomes. For example, one patient had a postoperative audiometric evaluation 16 months after the surgery. However, the same results remained when we remove the data from that patient. Third, the gender effect did not directly translate to a significantly higher success rate in the male patients. However, readily available preoperative audiometric data may provide surgeons and patients of different gender with reasonable expectations about surgical outcomes. Additionally, as a retrospective study design, causal relationships are not determined. Finally, this study included only Taiwanese populations, the generalizability of the results may be limited. Future prospective studies with a large sample size and multiple ethnicities to examine this phenomenon are needed.
Conclusions
We report evidence to support a possible gender effect on the hearing outcomes after stapedotomy in an Asian population with clinical otosclerosis. Compared to female patients, male patients with otosclerosis demonstrated a stronger correlation between improvement in postoperative AC thresholds and ABGs and the size of preoperative ABGs. Age, type, and degree of preoperative hearing loss may affect the surgical success rate. Mechanisms underlying the effect on predicting hearing outcomes based on preoperative audiological data warrant future prospective study.
Supplemental Material
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211037645 - Factors Associated With Hearing Outcomes After Stapedotomy in Taiwanese Patients With Clinical Otosclerosis
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211037645 for Factors Associated With Hearing Outcomes After Stapedotomy in Taiwanese Patients With Clinical Otosclerosis by Pei-Hsin Chen, Kai-Nan Lin, Hsiu-Yin Lin, Rui-Bin Yu, Pi-Yun Liu, Wan-Ting Shih and Jeng-Wen Chen in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
Jeng-Wen Chen had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Kai-Nan Lin, Hsiu-Yin Lin, and Jeng-Wen Chen contributed to study concept and design. Pei-Hsin Chen, Rui-Bin Yu, Pi-Yun Liu, and Wan-Ting Shih contributed to acquisition, analysis, or interpretation of data. Pei-Hsin Chen and Jeng-Wen Chen contributed to drafting of the manuscript. Rui-Bin Yu and Jeng-Wen Chen contributed to statistical analysis. Kai-Nan Lin and Hsiu-Yin Lin contributed to obtained funding. Kai-Nan Lin, Hsiu-Yin Lin, and Jeng-Wen Chen contributed to administrative, technical, or material support. Kai-Nan Lin and Jeng-Wen Chen contributed to study supervision. Pei-Hsin Chen, Kai-Nan Lin, and Hsiu-Yin Lin have equal contributions to this study. All authors contributed to critical revision of the manuscript for important intellectual content.
Acknowledgment
The authors are grateful for administrative assistance on this project provided by Chiu-Ping Wang, Shu-Hwei Fan, Wei-Chun Chen, and Uan-Shr Jan. The authors also thank the staff of the Audiology Department of Cardinal Tien Hospital, for their technical support. They received no additional compensation for their contributions. This manuscript was edited by Wallace Academic Editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Science and Technology of the Republic of China (Taiwan) under grant MOST 109-2511-H-567-001-MY2 and MOST 110-2511-H-567-001-MY2 and, in part, funded by Cardinal Tien Hospital under grant CTH-106A-2A29.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.