
Abstract
Background:
Recurrent aphthous stomatitis is one of the most prevalent oral mucosa diseases and the etiology is unclear. As a potent anti-inflammatory and immunomodulating agent, vitamin D can significantly affect oral cavity homeostasis. However, to the best of our knowledge, no study has been conducted in pediatric population on the potential role of vitamin D in recurrent aphthous stomatitis to date. The aim of the present study is to determine the vitamin D status in recurrent aphthous stomatitis in children.
Methods:
This study is conducted retrospectively. Seventy-two patients with minor recurrent aphthous stomatitis and 70 age-matched healthy controls included in the study. 25-Hydroxyvitamin D levels were measured in all patients using enzyme immunoassay.
Results:
Serum vitamin D levels were 16.4 (8.6) ng/mL in patient group and 23.1 (11.5) ng/mL in healthy controls. There was a statistically significant difference between the groups in terms of serum vitamin D levels (P = .002). There was no significant correlation between serum vitamin D levels and the severity of the recurrent aphthous stomatitis (r = 0.54, P = .76).
Conclusions:
Our study showed a significant difference in vitamin D levels between patients with recurrent aphthous stomatitis and the healthy control group. We also found no correlation between vitamin D status and the severity of the disease.
Introduction
Recurrent aphthous stomatitis is one of the most prevalent oral mucosa diseases. It affects 5% to 25% of the population, mostly women and in higher socioeconomic groups. 1 These idiopathic lesions are characterized by recurrent painful attacks. 2 The condition is chronic and usually self-limiting in immunocompetent patients. Etiology remains unclear, but local trauma, emotional stress, allergy, toxin exposure, poor oral hygiene, vitamin deficiency, and alterations in the oral flora are defined as risk factors. 3 The lesions are painful and their sizes range from 1 mm to a few centimeters in diameter. The lesion size is one of the diagnostic criteria used in classification, which is divided into 3 categories: major, minor, and herpetiform. 4 Minor aphthous stomatitis constitutes about 80% to 85% of the cases and is characterized by 1 to 5 erosions smaller than 1 cm in diameter, healing spontaneously within 5 to 10 days without scarring, while major aphthous stomatitis occurs as long-lasting lesions bigger than 1 cm in diameter and leaving a scar. 5
Vitamin D is a steroid hormone and plays an important role in calcium metabolism, but more recently, emerging evidence suggests that vitamin D plays an important role in immunity regulation. 6,7 Vitamin D receptor has been found in most of the immune cell types, including antigen-presenting cells, such as macrophages and dendritic cells, and T cells. The immunomodulatory effect of this vitamin has raised an interest in its possible role in etiology immune-dependent entities. Also, vitamin D deficiency has been associated with some autoimmune diseases. 8 As a regulator of mineral balance and bony tissue metabolism and a potent anti-inflammatory and immunomodulating agent, vitamin D can significantly affect oral cavity homeostasis. The role of vitamin D as a modifier of autoimmunologic conditions of the oral cavity is of considerable importance. 5
There are only a few studies conducted in adult population to investigate the possible relationship of vitamin D and recurrent aphthous stomatitis. 2,5,9 However, to the best of our knowledge, no study has been conducted in pediatric population on the potential role of vitamin D in recurrent aphthous stomatitis to date. The aim of the present study is to determine the vitamin D status in recurrent aphthous stomatitis in children.
Materials and Methods
This study is done retrospectively from January 2014 to January 2019. We performed power analysis to calculate minimum number of patient for the study. After accepting significance level (type 1 error) as 0.05 and power (type 2 error) as 0.8, we decided to include at least 30 patients and 30 control groups as minimum numbers to the study. Hence, a cohort of 76 children of both sexes (41 girls and 35 boys) aged between 3 and 12 years with recurrent minor aphthous stomatitis were included as patient group and 70 age-matched healthy children (34 girls and 36 boys) were included as control group. After all patients records were evaluated, patients were called for a face-to-face interview to the outpatient clinic of our hospital. Four patients who did not except for the interview were excluded from the study. So study was conducted with 72 patients. All patients were evaluated by investigators with a face-to-face interview. Patients aged between 3 and 12 years with a validated history of at least 3 episodes of minor idiopathic recurrent aphthous stomatitis within the previous 12 months were included. Only minor aphthous lesions <1 cm in diameter were included in the study. Control group consisted of healthy children who had no complaints or systemic diseases and admitted to our well-child follow-up outpatient clinic. Severity classification was proposed by Bagan et al; type 1 disease is characterized by the intervals between the flare-ups of over 3 months, whereas in the type 2 disease, the flare-ups occur at 1 to 3 months intervals. In type 3, aphthous lesions are present almost continuously. 10
Exclusion criteria were as follows: (1) age <3 years or >12 years, (2) any systemic or chronic disease, (3) use of vitamin D supplementation within last 6 months, and (4) major or herpetiform aphthous stomatitis.
Age, gender, and place of residence were recorded. Diagnosis of recurrent aphthous stomatitis was based on the physical examinations by an experienced pediatrist and patient history.
25-Hydroxyvitamin D [25(OH)D] levels were measured in all patients twice yearly (in the winter and summer seasons due to seasonal variability) using enzyme immunoassay (EIA). Average level of serum 25(OH)D was considered for the study; 25(OH)D values is defined as sufficient if at least 30 ng/mL, insufficient between 20 and 30 ng/mL, and deficient if <20 ng/mL.
This study complied with the tenets of the Declaration of Helsinki and was approved by our local ethics committee. Written informed consent was obtained from the legal guardians of all the patients before the study.
Statistical Analysis
Data were analyzed using SPSS 21 (IBM SPSS, Chicago, Illinois). Continuous variables were expressed as the mean (standard deviation), ordinal variables as median (minimum-maximum), and as frequency with percent for categorical variables. To evaluate the level of data normality for continuous variables, the Kolmogorov-Smirnov test was used; χ2 test was used to test differences in categorical variables between the 2 groups. Independent sample t test was used for comparing the means of continuous variables. For more than 2 independent groups, the Kruskal-Wallis test was used for non-normally distributed variables. A Spearman ρ correlation was used to analyze the association between non-normally distributed variables. Correlations between normally distributed variables were analyzed by Pearson correlation coefficient. A significant level of P < .05 was accepted significant.
Results
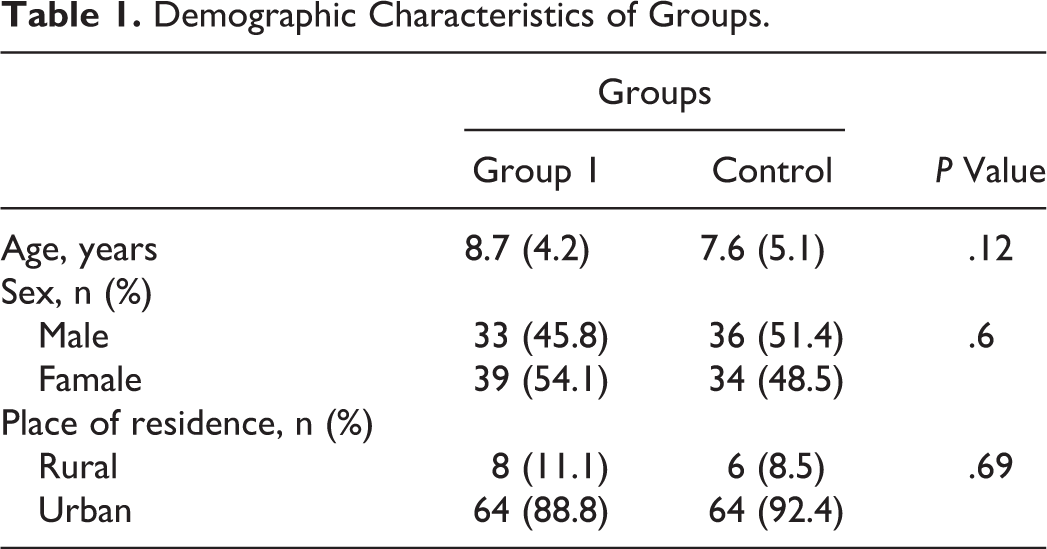
A total of 72 patients (39 females, 33 males) were included as case group (group 1) and 70 healthy children (34 females, 36 males) in case group (group 2). The mean age of the group 1 was 8.7 (4.2) years and that of the group 2 was 7.6 (5.1) years. There was no statistically significant difference between the 2 groups in terms of age (P = .12) and gender (P = .6). Also, place of residence was not significantly different between the groups (Table 1).
Demographic Characteristics of Groups.
The mean duration of recurrent aphthous stomatitis was 32 (18-58) months. The mean number of the lesions per patient was 2 (1-5). The mean frequency of recurrence was 24 (14-90) days. The mean healing time was 5.3 (3.5) days. There was no significant correlation between serum vitamin D levels and the numbers of lesions (r = 0.081, P = .76), the mean frequency of recurrence (r = 0.78, P = .65), and the mean healing time (r = 0.026, P = .966). Severity classification was performed with the suggestions of Bagan et al. 10 There was no significant correlation between serum vitamin D levels and the severity of the recurrent aphthous stomatitis (r = 0.54, P = .76; Table 2).
Vitamin D Status According to the Severity of Recurrent Aphthous Stomatitis.a
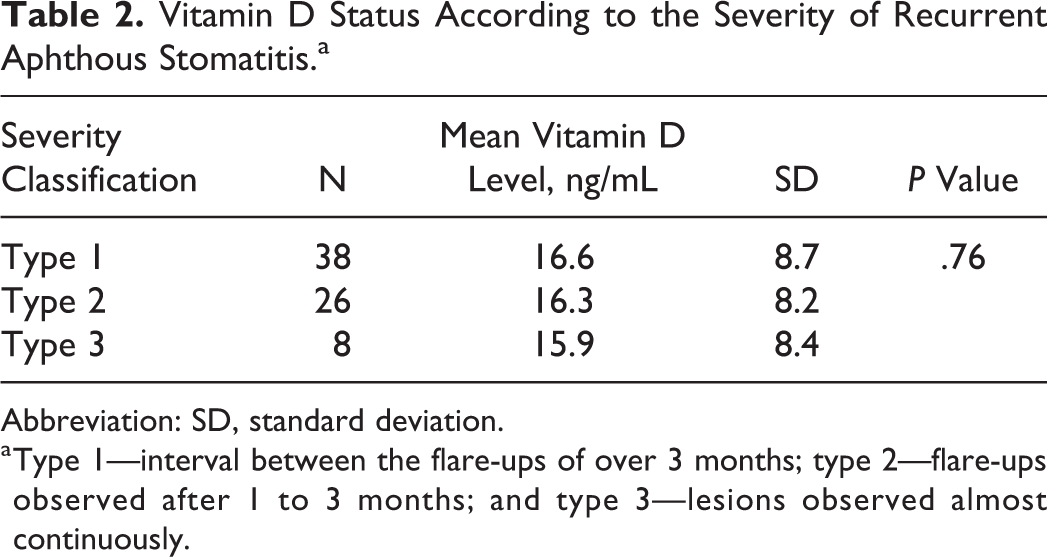
Abbreviation: SD, standard deviation.
a Type 1—interval between the flare-ups of over 3 months; type 2—flare-ups observed after 1 to 3 months; and type 3—lesions observed almost continuously.
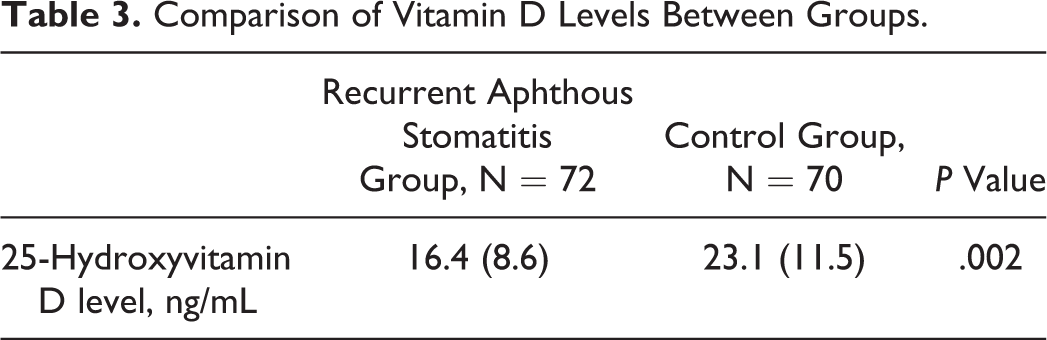
Serum vitamin D levels were 16.4 (8.6) ng/mL in group 1 and 23.1 (11.5) ng/mL in group 2. There was a statistically significant difference between the groups in terms of serum vitamin D levels (P = .002; Table 3).
Comparison of Vitamin D Levels Between Groups.
Discussion
Recurrent aphthous stomatitis is an oral condition characterized by the presence of erosions and ulcers appearing regularly on the oral mucosa. Although the etiopathogenesis of this condition is not fully understood, several studies have suggested that the main cause is related to genetically mediated immunologic disturbances modified by environmental factors, which may include stress, smoking, and iron, zinc, or vitamin B12 deficiencies. 4,9,11,12 Since the exact etiology of recurrent aphthous stomatitis is unknown, there is no effective therapy. Treatment options (topical analgesics, antiseptics, corticosteroids, etc) used for this disease are nonspecific and have limited efficacy. 2 The role of multivitamin supplementation in the treatment of recurrent aphthous stomatitis is controversial. 13,14
The enhanced expression of the Th1 gene cluster in comparison to the Th2 cluster in patients with recurrent aphthous stomatitis has been demonstrated. 15 The increased activity of Th1-type immune response accompanied by the decreased anti-inflammatory Th2-type cytokines and tumor growth factor-β levels are typical features of autoimmune diseases. 5 The profile of secreted cytokines is altered by vitamin D; hence, the production of Th1-type cytokine is decreased and the production of Th2 type is increased. Vitamin D deficiency may be a risk factor for autoimmunization. 5,6
Our study showed a significant difference in vitamin D levels between patients with recurrent aphthous stomatitis and the healthy control group. We also found no correlation between vitamin D status and the severity of the disease. To the best of our knowledge, there are only a few studies conducted in adult population on the relationship between recurrent aphthous stomatitis and vitamin D. 2,5,16 But the results are controversial. Krawiecka et al 5 conducted a study in Poland and found no significant difference between patients with recurrent aphthous stomatitis and healthy individuals in terms of vitamin D levels. Also, they found no correlation between vitamin D status and the severity of recurrent aphthous stomatitis. Khabbazi et al 16 reported that vitamin D levels were significantly lower in study group than control group. Similarly, Oztekin and Oztekin 2 found decreased levels in the serum of patients with recurrent aphthous stomatitis compared to healthy control patients. Also, Bahramian et al 17 reported that the serum levels of vitamin D in patients with recurrent aphthous stomatitis were significantly less than that in healthy individuals.
Although there are only a few studies published on the vitamin D status in recurrent aphthous stomatitis, other studies have been reported on syndromes associated with aphthous stomatitis, such as Behçet disease and periodic fever, aphthous stomatitis, pharyngitis, and cervical adenitis (PFAPA) syndrome. Several studies reported significantly lower vitamin D levels in Behçet disease in comparison to healthy control groups. 18 -20 Similarly, several studies found the vitamin D levels to be significantly lower in patients with PFAPA than that in the controls. 6,21,22
The possible action of vitamin D as a modifying factor in recurrent aphthous stomatitis seemed to be worth considering, because despite multicentered studies, relatively little is known about the etiopathogenesis of the disease. The biologic effects of vitamin D including its modification of both the innate and acquired immune system and its influence on the cytokine profile suggest the potential role of this hormone in the development of disease. 5,23 Therefore, given the regulatory effect of vitamin D on the immune system and based on the results of the present study, it can be concluded that the lower serum levels of vitamin D might be considered as possible factor for inducing recurrent aphthous stomatitis, especially genetically susceptible patients. However, it is not clear whether vitamin D deficiency is the cause or rather a consequence of the disease. So, even vitamin D replacement therapy will not cause significant adverse effects, recommending vitamin D as a supportive treatment option is controversial.
To the best of our knowledge, this is the first study conducted in pediatric population with recurrent aphthous stomatitis. We found significantly lower levels of vitamin D in patient group compared to healthy control group. The main limitation of this study is the retrospective design. However, further prospective randomized clinical trials with larger sample size are necessary to reveal the potential role of vitamin D in recurrent aphthous stomatitis.
Footnotes
Authors’ Note
Dr Burçin Nalbantoğlu is contributed to concept and design. Dr Burçin Nalbantoğu and Dr Ayşin Nalbantoğlu collected data, analyzed, did literature search, and wrote the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.