
Abstract
Objectives:
To quantify differences in waste and cost of disposable equipment between different tonsillectomy techniques.
Methods:
Prospective study of waste attributable to disposable waste produced by tonsillectomy surgery. Disposable equipment required for tonsillectomy using cold, monopolar electrocautery (ME), and coblation techniques was measured; and differences in mass, volume, and cost of equipment between the 3 techniques were quantified.
Results:
Cold technique was found to produce the least waste and have the lowest cost attributable to disposable surgical equipment. Projected single-case savings in mass and volume of waste resulting from using cold technique compared to ME were 1.272 kg and 1.013 L, respectively, and 1.043 kg and 1.723 L compared to coblation. Projected single-case savings in cost of disposable equipment for cold technique compared to ME were US$9.35 and US$185.05 compared to coblation.
Discussion:
Using cold technique for adult tonsillectomy reduces waste and cost of disposable equipment compared to ME and coblation.
Introduction
Several millions of tons of waste are produced by US hospitals yearly. 1 The operating room (OR) is a major source of waste, as optimization of sterile technique is accomplished largely through disposable items rather than through laundering and sterilization procedures. 2 This reliance on disposable items produces a significant waste stream, much of which is disposed of as hazardous waste requiring specialized disposal procedures. 1,3
As the OR is responsible for a disproportionate amount of biohazardous and traditional solid waste, it represents an area of opportunity for waste reduction interventions. 4 Systems-based interventions to reduce OR waste have been described. 1,3,5 -7 However, decisions on which technique to use for a given procedure are largely left to the discretion of individual providers, and technique-specific data on waste and cost are lacking in the published literature. For this reason, we endeavored to critically evaluate the equipment opened for a case—the surgical “pick list”—of a sample surgery, in order to quantify the effect of surgical technique on waste and cost resulting from use of disposable equipment.
We selected tonsillectomy as a test procedure for several reasons. First, tonsillectomy is one of the most common major surgical procedures in adult and pediatric patients in the United States, with Centers for Disease Control and Prevention data indicating roughly 500 000 procedures are performed yearly. 8 Even relatively small reductions in waste for such a common procedure could have significant positive impact if widely adopted. Second, tonsillectomy is a relatively simple procedure that does not require specialized ancillary equipment for optimal outcomes, and previous studies have shown the potential for waste reduction with critical evaluation of equipment required for tonsillectomy. 7 Finally, as a clean-contaminated procedure, sterile draping and equipment may be reduced to a bare minimum. 9
Currently, there is no single tonsillectomy technique widely accepted as superior, with cold dissection, bipolar electrocautery, monopolar electrocautery (ME), and coblation, all demonstrating similar rates of major complications and surgical success. 10 We evaluated the surgical pick list at our institution for each technique on an item-by-item basis to identify differences in equipment required for each technique. Additionally, we tabulated equipment cost, as prior work has identified possible cost differences between different tonsillectomy techniques. 11 We hypothesized that, due to its emphasis on reusable, sterilizable equipment, cold technique would be superior to ME and coblation in minimizing waste and cost related to disposable equipment.
Materials and Methods
This research study was approved by the University of New Mexico Hospital (UNMH) institutional review board on January 18, 2018. All decisions regarding equipment required for the procedures were made by the attending surgeon (D.A.M.), in consultation with the Otolaryngology OR coordinator where necessary. The original pick list was first evaluated, and unnecessary items eliminated. Once the pick list was optimized in this fashion, all disposable equipment items specific to each of the 3 techniques were identified. Where multiple clinically equivalent options were available, equipment waste was measured; and the option resulting in the least overall waste produced was selected. The new pick list was then used in 20 consecutive cases, with review of the equipment after each case determining which items had been used and whether additional items not on the pick list were required to be opened. This information was used to finalize the pick list, which subsequently was used without need for adjustment in more than 60 cases of adult tonsillectomy.
All disposable items thus identified were weighed using a standard metric scale, with packaging included in measurements. Volume was determined by liquid displacement in a graduated cylinder of both the items and all of their disposable packaging. Volumes of packaged items were measured in an open, unwrapped state to avoid inclusion of intrapackage air in the measured volume, and disposable packaging was included in all measurements of mass and volume. Due to challenges in accessing and handling contaminated postoperative waste at our institution, mass and volume of waste leaving the OR after surgery were not measured directly. Item costs were obtained from the OR inventory list and tabulated; these represent the cost for purchase by the hospital for bulk or individual order, as applicable. Costs for disposal of waste were obtained from the third party waste management specialists who contract with UNMH for waste disposal.
Results
Total mass, volume, and cost of disposable equipment for each technique are reported in Table 1. Savings in mass and volume of waste per case for cold technique compared to ME technique were 1.272 kg and 1.013 L, respectively. Savings in waste mass and volume compared to coblation technique were 1.043 kg and 1.723 L, respectively (Table 1).
Waste and Cost Comparison of Disposable Equipment by Tonsillectomy Technique.a
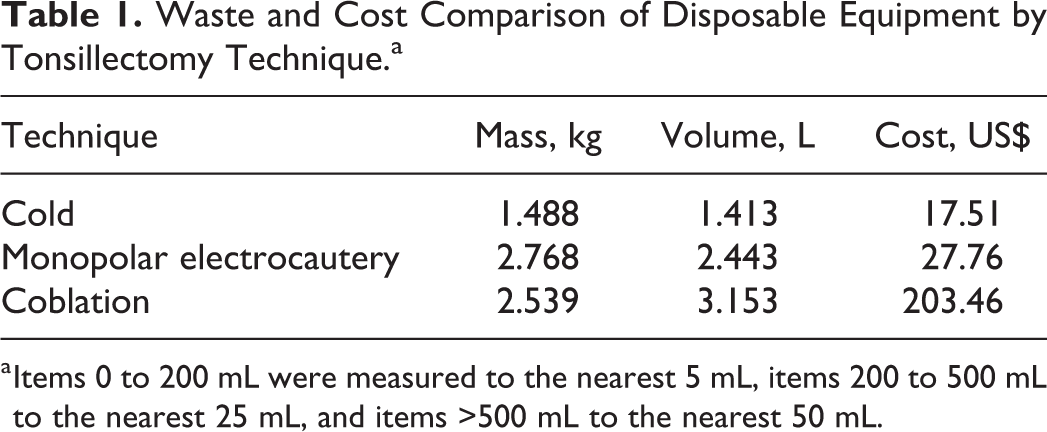
a Items 0 to 200 mL were measured to the nearest 5 mL, items 200 to 500 mL to the nearest 25 mL, and items >500 mL to the nearest 50 mL.
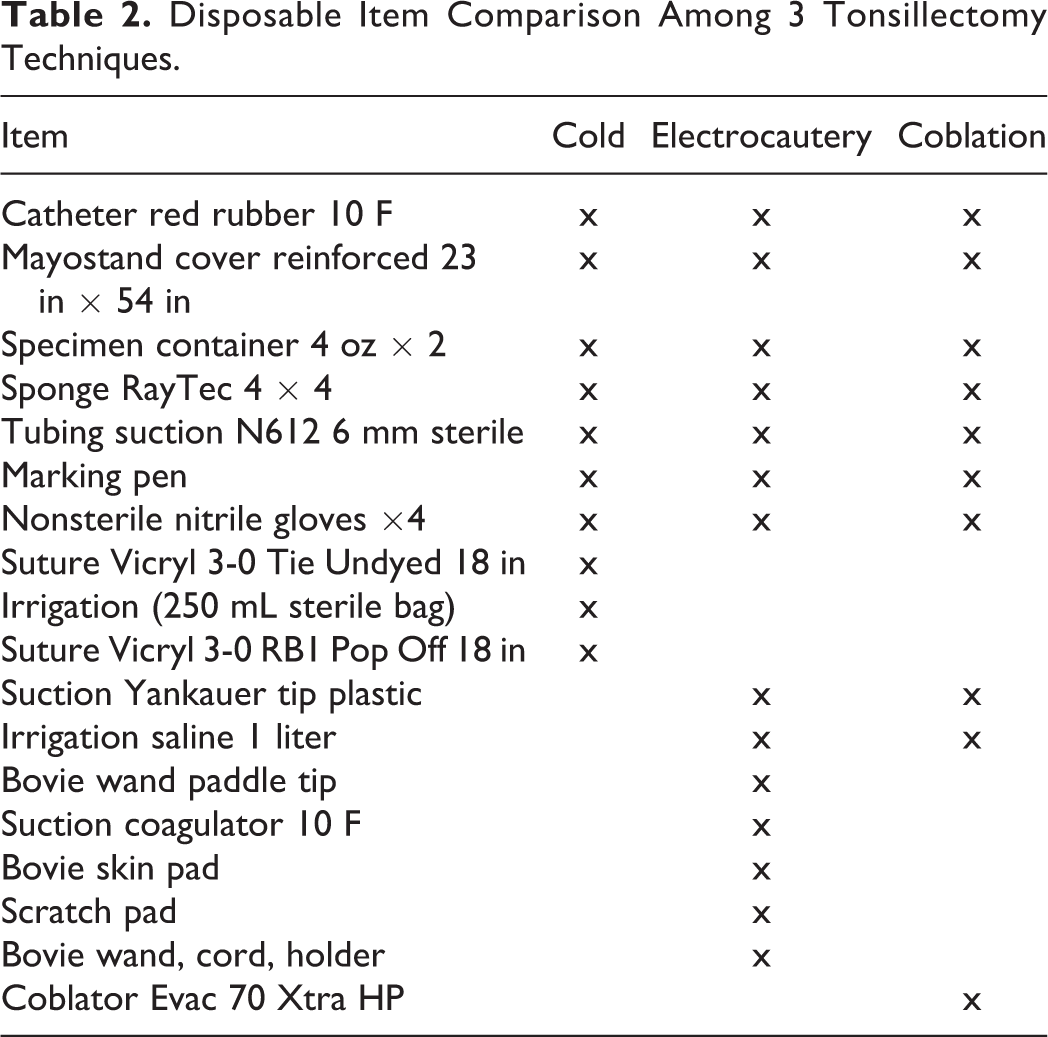
Disposable equipment cost savings for cold technique compared to ME were US$9.35 per case and compared to coblator were US$185.05 per case (Table 1). Cost of disposal of waste at our institution is US$0.33/pound or US$0.15/kg for nonbiohazardous waste and US$0.99/pound or US$0.45/kg for biohazardous waste. Accounting for this disposal cost with appropriate segregation of nonbiohazardous and biohazardous waste, total cost savings per case for cold technique compared to ME were US$9.92 and compared to coblation were US$185.52. The itemized list of disposable equipment across all 3 techniques is compared in Table 2, and a breakdown of the list of disposable equipment used in cold technique tonsillectomy is presented in Table 3. The new pick list has now been used in over 60 consecutive cases of adult tonsillectomy, with adequate instrumentation for all cases and no conversions to coblation or electrocautery required.
Disposable Item Comparison Among 3 Tonsillectomy Techniques.
Disposable Items in Pick List for Cold Technique Tonsillectomy.a
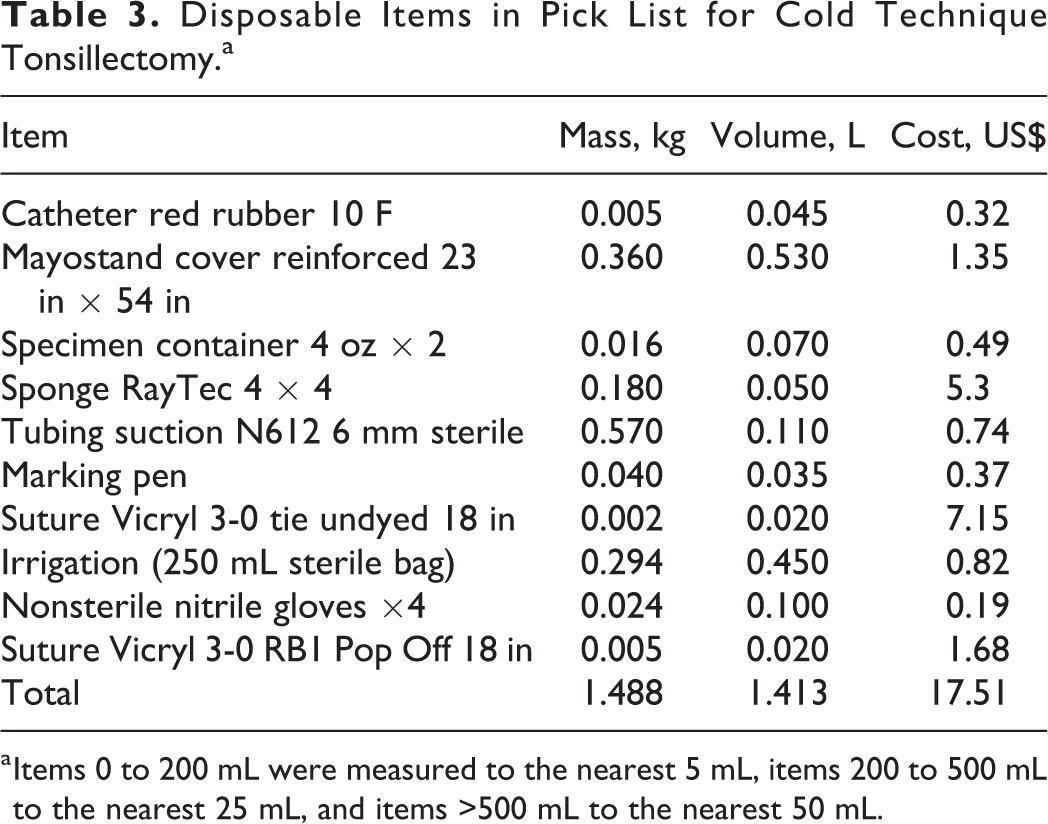
a Items 0 to 200 mL were measured to the nearest 5 mL, items 200 to 500 mL to the nearest 25 mL, and items >500 mL to the nearest 50 mL.
Discussion
Recent reports have highlighted the harmful effects of environmental pollution on population health. 12,13 Ironically, the US health-care sector is a major contributor to this pollution. 14 To reduce this environmental footprint, change will be required at multiple levels of government and within the health-care sector itself; however, individual providers have the power to make choices to reduce waste significantly within their own practice. The information required to make these choices is severely lacking in the published literature. Here, we report a sample study of such data: a quantitative comparison of waste and cost of disposable equipment between cold technique, ME, and coblation for adult tonsillectomy. Prior studies have discussed the effect of critical review of the pick list for a given surgical case 7 and the intersurgeon differences in costs for tonsillectomy, 11 but to our knowledge, ours is the first to report the differences in disposable equipment waste and cost between specific tonsillectomy techniques.
Annual cost and waste savings may be projected from these single-case data. For a single surgeon operating at our hospital performing an average of 40 adult tonsillectomies a year, converting from ME to cold technique is expected to result in waste savings of 51 kg and 41 L, and from coblation to cold technique, savings of 42 kg and 69 L. Cost savings, including disposal costs, over the same time frame would be US$396.80 for changing from ME and US$7420.80 for changing from coblation. On a larger scale, nationwide data on surgeon choice of tonsillectomy technique in America are not available, but for every 10 000 tonsillectomies, using our hospital’s costs for waste disposal, change in technique alone could result in reduction of approximately 12 720 kg and 10 130 L in waste with reduction in cost of US$99 200 if converting from ME, or 10 430 kg and 17 230 L in waste with reduction in cost of US$1 855 200 if converting from coblation.
Previous authors have noted the challenges in exact quantification of hospital costs and charges, particularly where disposable instrumentation is concerned. 15 Due to this complexity, we report only the actual cost of the individual items and disposal to the hospital itself; precise measurement of charges to the patient, as well as fiscal impact on the hospital or the US medical system, are beyond the scope of this study.
We note several limitations to this study. Our data represent a proxy of the waste reduced, as the actual waste being removed from the OR at the end of a case or a series of cases was not measured due to the difficulty of obtaining these data within the OR setting at our institution. Reusable equipment costs were not measured; however, reusable equipment is similar across all 3 pick lists, and prior research suggests that disposable equipment exerts a disproportionately large effect on surgical waste compared to reusable equipment. 4
Implications for Practice
Cold technique for tonsillectomy, compared to ME and coblation techniques, produces less waste and cost due to reduction in disposable equipment. Critical evaluation of disposable equipment required for different surgical techniques is recommended to optimize waste reduction. When multiple clinically equivalent techniques are available for a given procedure, we recommend that surgeons consider the technique that produces the least waste, in order to maximize benefit to the environment and minimize costs. Future work in this area should include the cost and energy demand from sterile processing, as well as production, transport and disposal of disposable and reusable instrumentation, to incorporate this information in a comprehensive environmental and fiscal evaluation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.