
Abstract
Introduction and Aims:
There is no consensus on the optimal tonsillectomy technique in adult patients. The study aims to identify all studies comparing the outcomes of coblation versus bipolar diathermy in adult patients undergoing tonsillectomy.
Methods:
A systematic review and meta-analysis were performed as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Primary outcomes were hemorrhage and postoperative pain. Secondary outcome measures included return to theatre, analgesia, intraoperative bleeding, diet, tonsillar healing, and operation time. Fixed-effects modeling was used for the analysis.
Results:
Six studies were identified enrolling a total of 1824 patients. There were no significant differences in terms of reactionary hemorrhage (OR = 1.81, P = .51), delayed hemorrhage (OR = 0.72, P = .20), or postoperative pain (mean difference = −0.15, P = .45); however, there is a general trend favuring coblation. For secondary outcomes, no significant differences noted in terms of intraoperative bleeding, diet, and cases returning to theatre. Analgesia administration was either insignificant or higher in the coblation group. The coblation group had longer operation time and greater healing effect on tonsillar tissue.
Conclusions:
There were no significant differences in outcomes for coblation and bipolar diathermy for adult tonsillectomy patients in this systematic review and meta-analysis.
Keywords
Introduction
Tonsillectomy is one of the commonly performed procedures globally by otolaryngologists and continues to be the most regularly performed surgeries in adults. 1 Adult tonsillectomy is indicated in chronic recurrent tonsillitis, suspicion of tonsillar malignancy, and in upper airway obstruction secondary to tonsillar hypertrophy. 2 Over the years, various techniques and instruments have evolved to aid tonsillectomy, such as bipolar diathermy dissection, harmonic ultrasonic, laser dissection, and, more recently, the coblation method. 3
Coblation involves passing radiofrequency energy through a conductive medium breaking down intracellular bonds and in effect segregates the tissue. 5 Regardless of the technique used, differences are present in complications including postoperative pain, hemorrhage, and postoperative infection. Hence, the debate about the optimal surgical technique continues in literature. 4
Diathermy involves the use of high radiofrequency current that is used to cut through or coagulate tissue. 5 Bipolar diathermy involves current that is being passed through 2 tips of the same forceps, hence the term “bipolar.” 6 Traditionally, diathermy was mainly used to seal the blood vessels after the surgical removal of the tonsils by a blade. 7 The use of bipolar diathermy has increased in popularity 8 as a standalone procedure, to perform both the dissection of the tonsils and the sealing of the blood vessels to stop the bleeding. In the context of ENT, bipolar diathermy is not only used in tonsillectomy, but it is also used to treat epistaxis. This is due to the sealing effect the heat has on the blood vessels to achieve haemostasis.9,10
There is a growing amount of research around coblation and bipolar diathermy techniques,11-16 including a previous meta-analysis comparing coblation to various tonsillectomy techniques. 17 However, to our knowledge, there were no meta-analyses published comparing bipolar and coblation tonsillectomy techniques. Therefore, our study aims to establish the differences in efficacy between coblation and bipolar diathermy techniques and tonsillectomy outcome among adults population.
Methods
A systematic review and meta-analysis were conducted as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 18
Eligibility Criteria
All randomized controlled trials (RCTs) and observational studies comparing coblation versus bipolar diathermy hemostasis techniques for tonsillectomy were included. Coblation was the intervention group of interest, and bipolar diathermy was the comparator. The study also included patients having bipolar scissors, bipolar forceps as well as cold steel and bipolar diathermy hemostasis as the comparator. All patients were included irrespective of gender or comorbidity status as long as they belonged to either a study or control group. All case reports or cohort studies without a comparison group, studies not written in English, as well as studies involving pediatric population were excluded. The study also excluded the following techniques: bipolar molecular resonance coagulation, tonsillotomy, unipolar or monopolar diathermy, adenotonsillectomy, children tonsillectomy, and conventional or traditional tonsillectomy without explicitly stating bipolar diathermy as the primary method for hemostasis.
Primary Outcomes
The primary outcomes are hemorrhage and postoperative pain. Hemorrhage is either reactionary (within 24 hours of the operation) or delayed (after 24 hours of the operation).
Secondary Outcomes
The secondary outcomes included a return to theatre, administration of analgesia, intraoperative bleeding and operation time (in minutes), return to normal diet (in days), and tonsillar fossae healing.
Literature Search Strategy
Two authors (A.A. and M.K.) independently searched the following electronic databases: MEDLINE, EMBASE, EMCARE, CINAHL, and the Cochrane Central Register of Controlled Trials (CENTRAL). The last search was run on April 12, 2020. Thesaurus headings, search operators, and limits in each of the above databases were adapted accordingly. Beside this, World Health Organization International Clinical Trials Registry (http://apps.who.int/trialsearch/), ClinicalTrials.gov (http://clinical-trials.gov/), and ISRCTN Register (http://www.isrctn. com/) were searched for details of ongoing and unpublished studies. The search terminologies included “coblation,” “bipolar,” and “tonsillectomy.” The bibliographic lists of relevant articles were also reviewed.
Selection of Studies
The title and abstract of articles identified from the literature searches were assessed independently by 2 authors. The full texts of relevant reports were retrieved, and those articles that met the eligibility criteria of our review were selected. Any discrepancies in study selection were resolved by discussion between the authors.
Data Extraction and Management
An electronic data extraction spreadsheet was created in line with Cochrane data collection form for intervention reviews. The spreadsheet was pilot-tested in randomly selected articles and adjusted accordingly. Our data extraction spreadsheet included study-related data (first author, year of publication, country of origin of the corresponding author, journal in which the study was published, study design, study size, the clinical condition of the study participants, type of intervention, and comparison), baseline demographics of the included populations (age and gender), and primary and secondary outcome data. The data and results were cooperatively collected and recorded, and any disagreements were solved via discussion.
Data Synthesis
Data synthesis was conducted using the Review Manager 5.3 software. The extracted data were entered into review manager by 3 independent authors. The analysis involved used was based on fixed-effects modeling. The results were reported in forest plots with 95% CIs.
For dichotomous outcomes, the OR was calculated between the 2 groups. The OR is the odds of an event in the coblation group compared with the bipolar group. An OR of greater than 1 for the reactionary hemorrhage and delayed hemorrhage would favur the coblation group, an OR of less than 1 would favur the bipolar group, and an OR of 1 would favur neither groups.
For continuous outcomes, the mean difference (MD) was calculated between the 2 groups. A positive MD for the postoperative pain score by day 7 would favur the coblation group, a negative MD would favur the bipolar group, and an MD of 0 would favur neither groups.
Assessment of Heterogeneity
Heterogeneity among the studies was assessed using the Cochran Q test (χ2). Inconsistency was quantified by calculating I2 and interpreted using the following guide: 0% to 25% may represent low heterogeneity, 25% to 75% may represent moderate heterogeneity, and 75% to 100% may represent high heterogeneity.
Methodological Quality and Risk of Bias Assessment
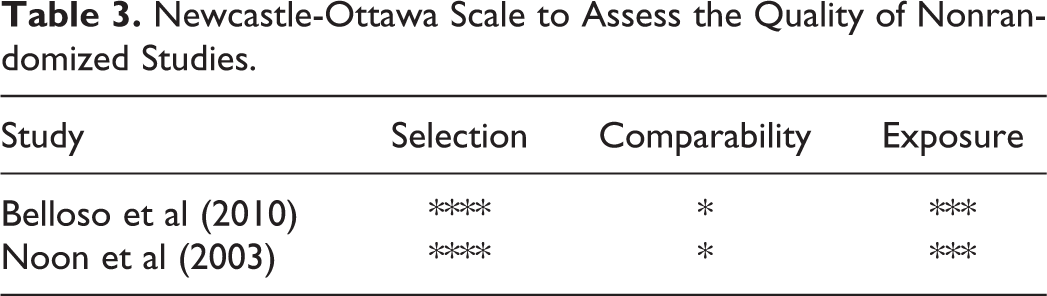
Two authors independently assessed the methodological quality as well as the risk of bias for articles matching the inclusion criteria. A third author was used as an adjudicator if a decision was disputed. For randomized trials, the Cochrane tool for evaluating the risk of bias was used. Domains assessed included selection bias, performance bias, detection bias, attrition bias, reporting bias, and other sources. The RCT studies are classified as low, unclear, and high risk of bias. For nonrandomized studies, the Newcastle-Ottawa Scale 7 was used. It uses a star grading system to assess studies in terms of 3 domains: selection, comparability, and exposure. The total maximum score for each study is 9 stars.
Results
Literature Search Results
The search strategy retrieved 546 studies, and after a thorough screening of the retrieved articles using the inclusion and exclusion criteria, the authors identified 6 studies in total which met the eligibility criteria (Figure 1).
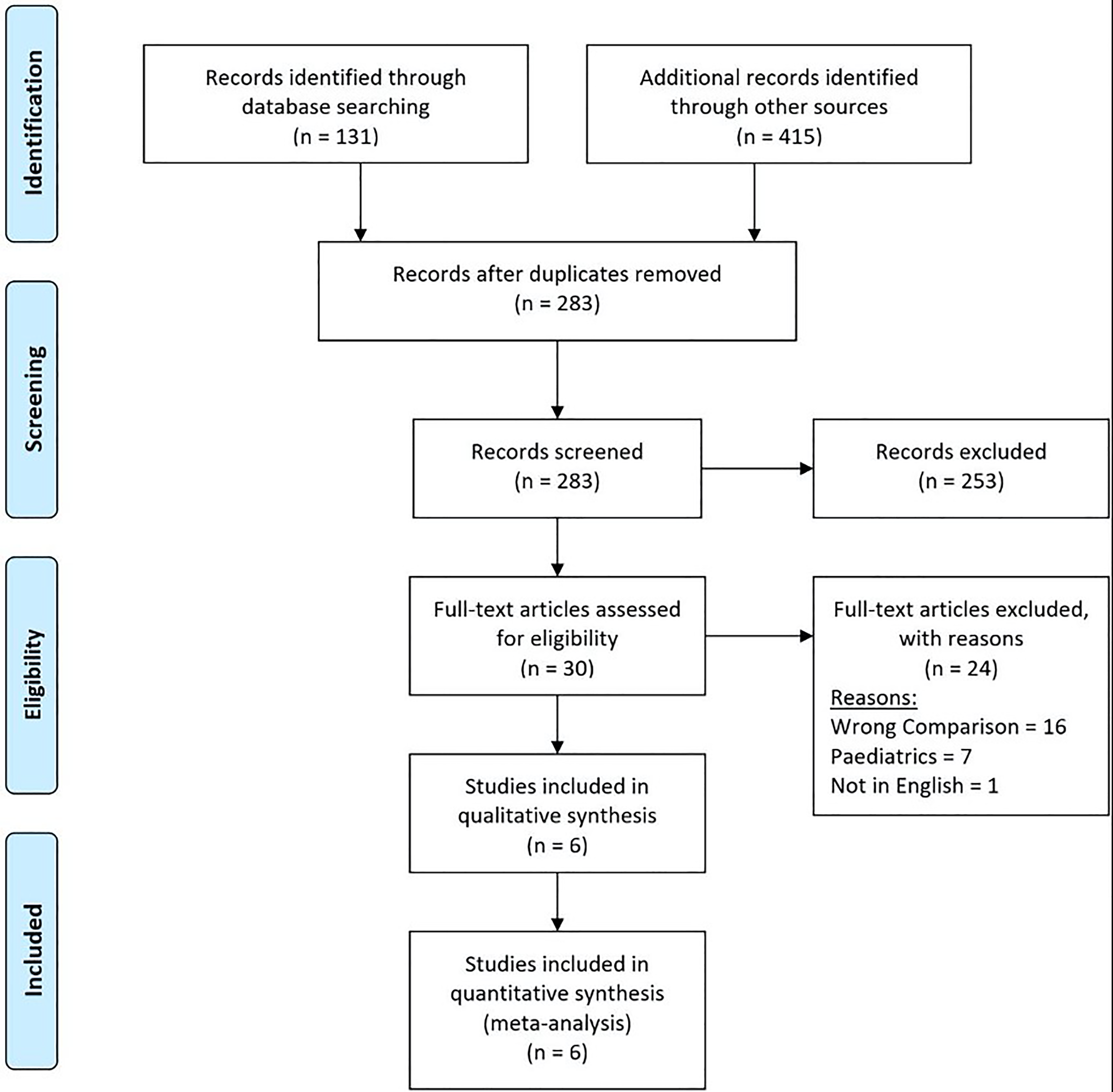
PRISMA flow diagram illustrating the search and selection processes applied during the overview. PRISMA indicates Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Description of Studies
The baseline characteristics of the included studies are summarized in Table 1.
Baseline Characteristics of the Included Studies.
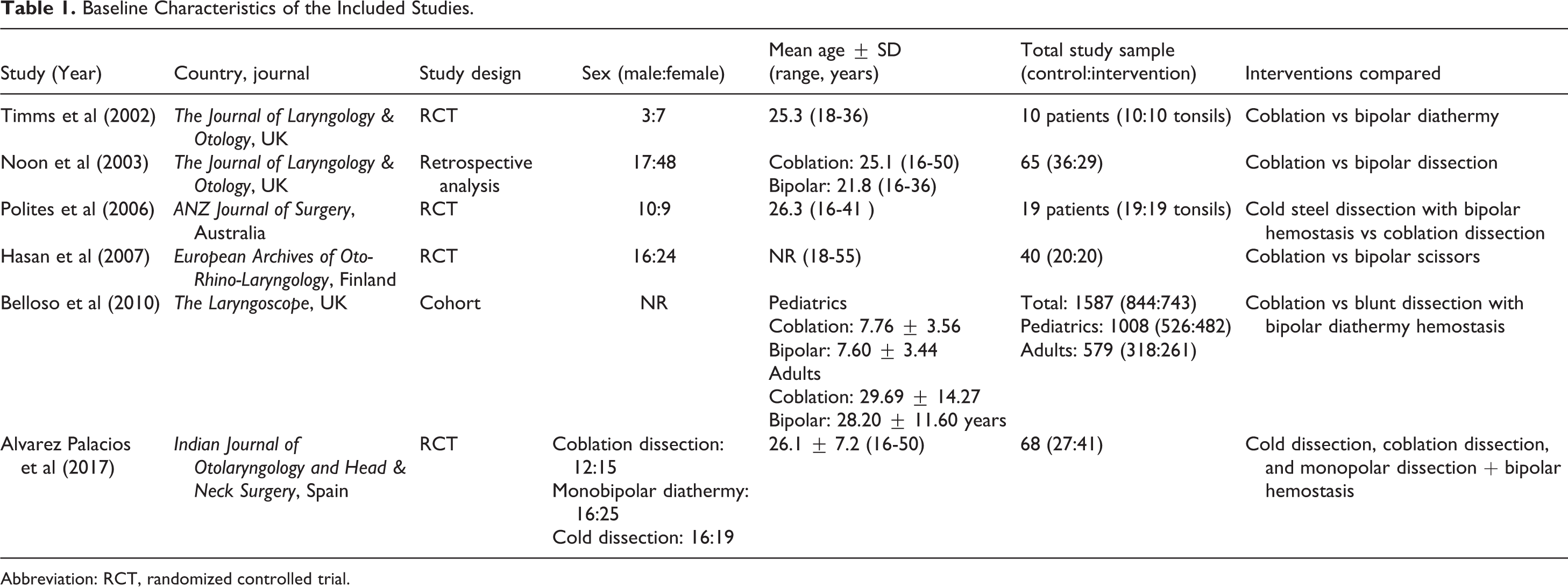
Abbreviation: RCT, randomized controlled trial.
Timms et al 2002
Timms et al performed single-center double-blinded RCT that included 10 adult patients with recurrent tonsillitis undergoing routine tonsillectomy. The randomization of patients was done through storing numbers in opaque envelopes, to have one tonsil removed completely by tissue coblation and the other by bipolar dissection. The surgical techniques on each side were not mentioned to the patients. Bipolar dissection was done using the standard technique (set at 4/10- and 50-Watts power). All tonsillectomies were extracapsular. They have excluded patients with history quinsy, medical disease, and bleeding disorders. 11
Noon et al 2003
Noon et al conducted a single-center retrospective study that included 65 adult patients undergoing tonsillectomy. The study included patients undergoing coblation tonsillectomy or bipolar diathermy. At the end of this period, one researcher has analyzed the patients’ notes. Bipolar dissection was done using the standard technique (set at 4/10- and 50-Watts power). All tonsillectomies were extracapsular. In addition, the study excluded obese patients. 12
Polites et al 2006
Polites et al performed a single-center double-blinded prospective RCT that included 20 adult patients listed for tonsillectomy due to symptoms of tonsillitis. Randomly, each patient had one tonsil selected for removal by cold steel dissection with bipolar hemostasis and the other tonsil by coblation. Bipolar dissection was done using the standard technique (set at 4/10- and 50-Watts power). All tonsillectomies were extracapsular. They have excluded patients with history of peritonsillar abscess and bleeding disorders. 13
Hasan et al 2007
Hasan et al conducted a single-center RCT that included 40 adult patients listed for tonsillectomy due to symptoms of tonsillitis. Patients were randomly allocated into 2 groups: 20 patients underwent coblation and the other 20 were operated with bipolar scissors. The randomization was generated by using sequence number on the day of the operation. All tonsillectomies were extracapsular. They have excluded patients with history of peritonsillar abscess, major health problems, and bleeding disorders. 14
Belloso et al 2010
Belloso et al conducted a single-center prospective observational cohort study that included 318 coblation tonsillectomies with a control group of 261 tonsillectomies performed by blunt dissection from July 2001 to January 2003. The groups reported in the study were extracted from a tonsillectomy audit. All tonsillectomies were extracapsular. 15
Alvarez Palacios et al 2017
Alvarez Palacios et al performed single-center RCT that included 103 adult patients who were scheduled for elective tonsillectomy. Patients were randomized to tonsillectomy with cold dissection, monopolar–bipolar dissection, and coblation dissection. All tonsillectomies were extracapsular. 16
Primary Outcomes
Hemorrhage
Hemorrhage was divided into reactionary hemorrhage (within 24 hours postoperatively) and delayed hemorrhage (after 24 hours postoperatively).
In Figure 2, reactionary hemorrhage was reported in 4 studies enrolling in 193 patients. There was no statistically significant difference seen in the OR analyses showing a lower rate of reactionary hemorrhage for the coblation group (OR = 1.81, CI, 0.31-10.40, P = .51). A moderate level of heterogeneity was found among the studies (I2 = 42%, P = .19).
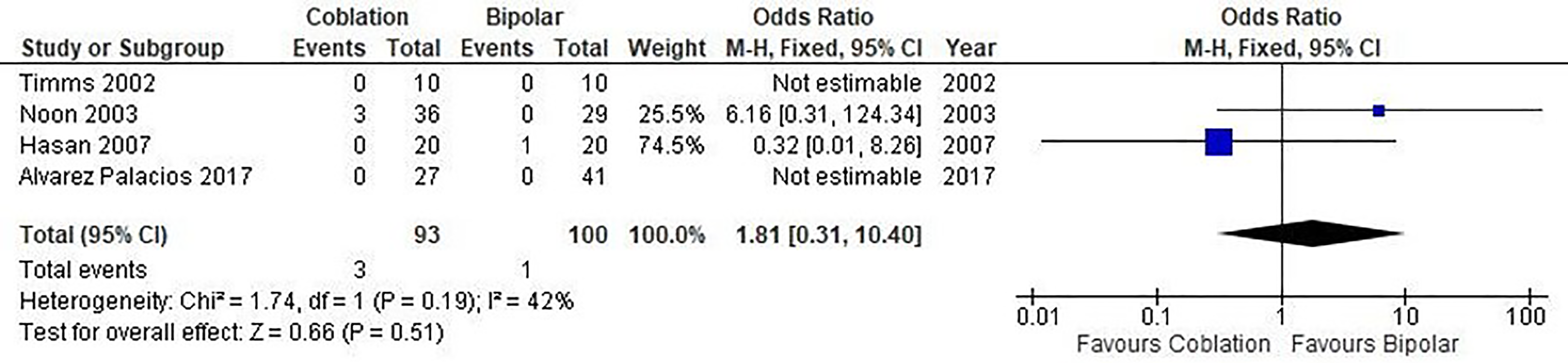
Forest plot of coblation versus bipolar tonsillectomy—reactionary hemorrhage. Quantitative analysis showing the OR in the reactionary hemorrhage reported by Timms et al (2002), Noon et al (2003), Hasan et al (2007), and Alvarez Palacios et al (2017).
In Figure 3, delayed hemorrhage was reported in 6 studies enrolling 810 patients. There was no statistically significant difference seen in the OR analysis illustrating a lower rate of delayed hemorrhage for the coblation group (OR = 0.72, CI, 0.43-1.19, P = .20). A moderate level of heterogeneity was found among the studies (I2 = 59%, P = .01).
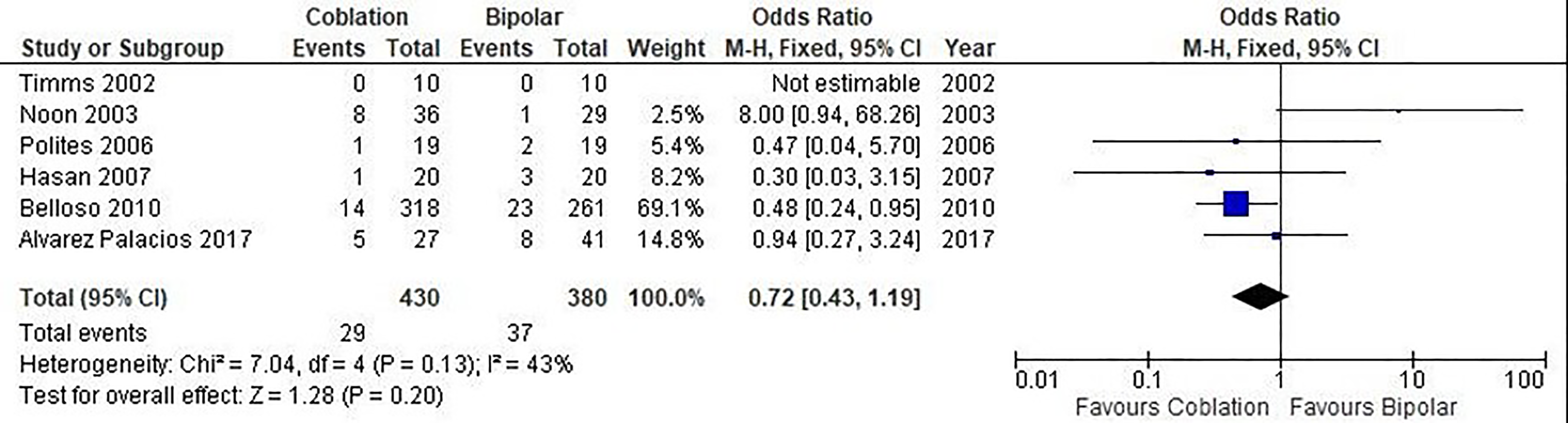
Forest plot of coblation versus bipolar tonsillectomy—delayed hemorrhage. Quantitative analysis showing the OR in the delayed hemorrhage reported by Timms et al (2002), Noon et al (2003), Polites et al (2006), Hasan et al (2007), Belloso et al (2010), and Alvarez Palacios et al (2017).
Postoperative pain by day 7
In Figure 4, postoperative pain by day 7 was reported using different pain scores in 2 studies enrolling 106 patients. There was no statistically significant difference seen in the standardized MD analysis showing less postoperative pain associated with the coblation group (standardized MD = −0.15, CI, −0.54 to 0.24, P = .45). A low level of heterogeneity was found among the studies (I2 = 0%, P = .64).

Forest plot of coblation versus bipolar tonsillectomy—postoperative pain by day 7. Quantitative analysis showing the standardized mean difference in postoperative pain by day 7 reported by Polites et al (2006) and Alvarez Palacios et al (2017).
Timms (2002) and Hasan (2007) also reported postoperative pain scores on day 7; however, this was given as a median (and range), therefore not allowing quantitative analysis. Timms showed a significant median score favuring the coblation group (P = .001), while Hasan showed an insignificant difference between the 2 groups (P = .962).
Secondary Outcomes
Return to theatre
Noon et al reported no significant difference in the number of cases that returned to the theatre between coblation and bipolar groups (4 and 0 cases, respectively).
Administration of analgesia
Hasan et al and Alvarez Palacios et al looked into the administration of analgesia following both coblation and bipolar diathermy. Hassan et al used a self-administered device containing opioids and showed a higher median number of analgesic doses required by the coblation group during the hospital stay compared to the bipolar group (9 vs 4). Alvarez Palacios et al used a combination of paracetamol, codeine, dexketoprofen, and metamizole ampoles reporting no significant difference in the average consumption of analgesics during the first postoperative day.
Intraoperative bleeding
Hasan et al reported no significant difference between the coblation and bipolar groups in terms of intraoperative bleeding.
Diet
The time taken to return to a normal diet was reported by Hasan et al. The study found no significant difference in the patients’ opinion of their ability to return to a normal diet while comparing the 2 distinctive groups.
Effect on tonsils: Degree of healing in tonsillar fossae
Timms et al reported a significant difference in the healing of the tonsillar fossae between postcoblation and postbipolar dissection groups. The results found that the postcoblation group had more rapid healing of the tonsillar fossae. In the coblation group, 7 tonsils were fully healed, 1 tonsil had 50% slough, and 2 tonsils had only 25% slough. In the bipolar group, 9 tonsils were covered with 100% slough and 1 tonsil had 50% slough.
Operation time (minutes)
The operative time (minutes) between coblation and bipolar dissection groups was only reported by Hasan et al who found a significant difference between the 2 groups. In the coblation group, the mean time taken to operate was 20.5 minutes while the bipolar diathermy group had a mean operating time of 12 minutes with a P value of <.001.
Methodological Quality and Risk of Bias Assessment
The Cochrane Collaboration tool was used to assess the quality of the RCTs included in the study (Table 2). The Newcastle-Ottawa Scale was used to assess the quality of the nonrandomized studies (Table 3), which offers a star system for analysis. 19 The quality of the 2 nonrandomized studies (Belloso et al and Noon et al) was deemed to be high in selection and exposure but low incomparability. Overall, both studies were of good quality based on the AHRQ standards. 19
Bias Analysis of the Randomized Trials Using the Cochrane Collaboration Tool.
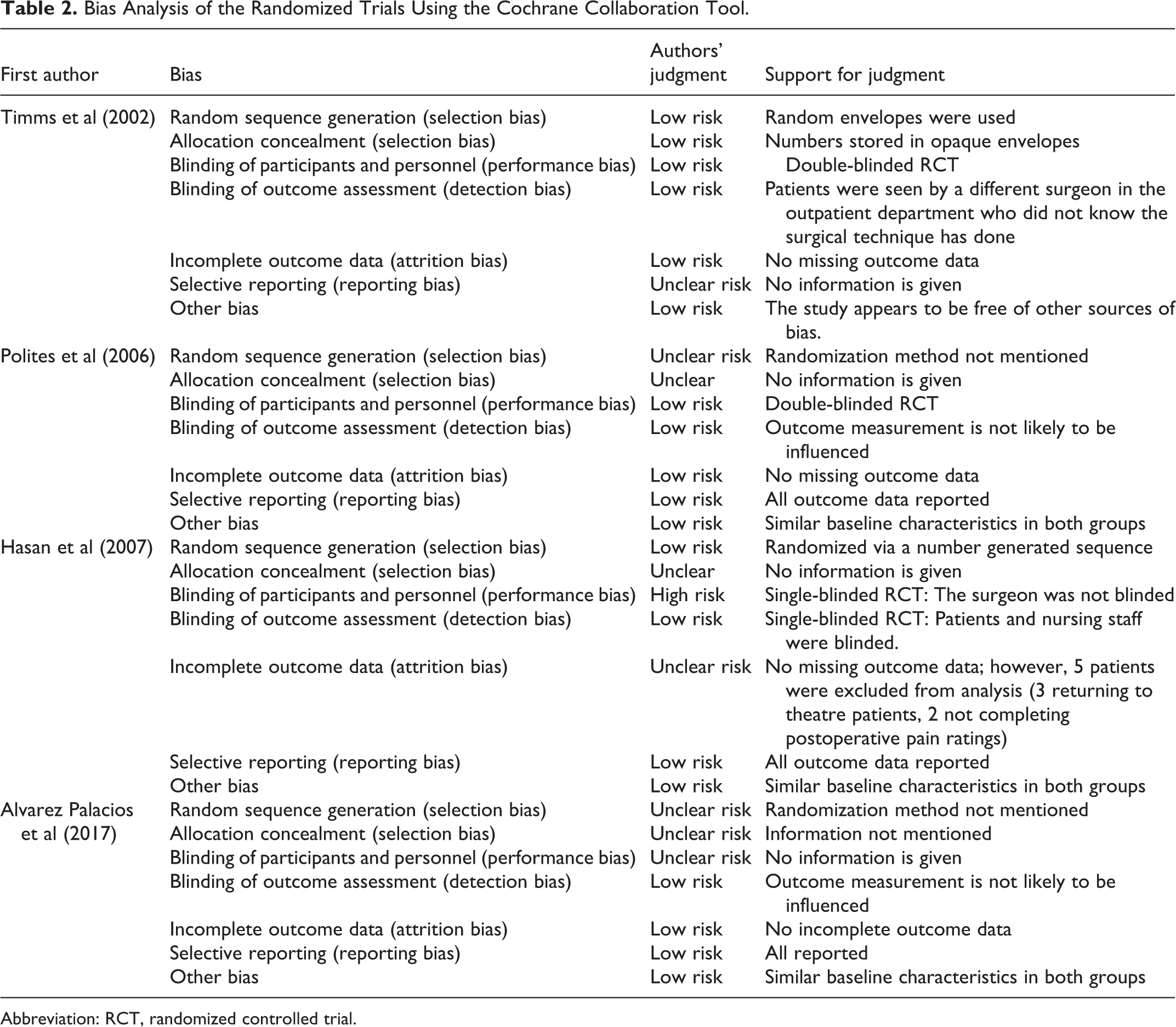
Abbreviation: RCT, randomized controlled trial.
Newcastle-Ottawa Scale to Assess the Quality of Nonrandomized Studies.
Discussion
Coblation showed a similar effect when compared with bipolar diathermy, with all primary outcomes as shown by the results of the analyses. Reactionary hemorrhage showed no significant (P = .51) improvements in the coblation group when compared with the bipolar group (Figure 2). Also, there were a similar number of delayed hemorrhage cases within both groups (P = .20; Figure 3). Furthermore, postoperative pain scores also had no significant difference (P = .45) in both techniques (Figure 4). The between-study heterogeneity was deemed moderate for reactionary and delayed hemorrhages (I2 = 42% and 43%, respectively); however, the heterogeneity for postoperative pain score was judged to have a low level (I2 = 0%), based on the assessment as mentioned in section “Methods.”
In addition to the outcomes mentioned above, the findings of this study reported many secondary outcomes that proved coblation has very similar efficacy to bipolar diathermy for adult patients undergoing tonsillectomy. Intraoperative blood loss and diet both showed similar results between both techniques. Similarly, there were no significant differences noted in terms of the number of cases that returned to the theatre. In addition, operative time was found to be longer in the coblation group. Furthermore, the rate of healing of the tonsillar fossae was seen to be greater in coblation compared with the bipolar technique. Regarding the administration of analgesia, Hasan et al found that the coblation group had a significantly higher number of analgesic doses during the hospital stay, while Alvarez Palacios et al found no significant difference between the 2 groups.
Even though tonsillectomy is one of the most commonly performed procedures in otorhinolaryngology and worldwide, none of the popularly used techniques for tonsillectomy is superior to date. 7 The current study findings show that coblation is not a superior or an inferior option to bipolar diathermy for adult patients undergoing tonsillectomy. The finding of an insignificant difference in the rates of hemorrhage is supported by the work done by Leinbach et al 7 who looked into tonsillectomy techniques and found no significant difference in both groups. However, other studies found that coblation had a higher rate of postoperative hemorrhage. 17 This controversy in the findings was addressed by Ragab et al 20 who mentioned that there are not enough large studies to detect the small difference in the rates of hemorrhage. Additionally, the work by Philpott et al 21 found that coblation had no symptomatic advantages over conventional dissection tonsillectomy, which supports the findings of this study regarding postoperative pain. In contrast, Cardozo et al 22 found a significant association between bipolar diathermy and postoperative pain in adult tonsillectomy. With regard to the healing of the tonsillar fossae, Temple et al 23 found all fossae to be healed in patients who underwent coblation tonsillectomy, which also supports the current study’s findings, but their study only included pediatric patients.
A study conducted in the United Kingdom highlighted that coblation is a cost-effective intervention for tonsillectomy when compared with cold steel procedures for both adult and pediatric patients, with a probability of at least .7 at being cost-effective. 24 In another study conducted in the United States, coblation was reported to have significantly lower costs compared to electrocautery surgery; however, the total cost of coblation was slightly higher when central supply was taken into account. 25
Based upon the results from the best available evidence comparing coblation tonsillectomy to bipolar diathermy in adult patients, there is no significant difference in the outcomes between the 2 techniques apart from more rapid healing of the tonsillar fossae in the coblation technique. The current evidence, therefore, suggests coblation tonsillectomy does not necessarily need to replace bipolar diathermy in adult patients undergoing tonsillectomy. However, complete certainty is difficult due to the controversial findings of the studies previously mentioned, highlighting the importance of additional well-designed, large, RCTs in order to draw a more definitive conclusion.
A systematic approach was applied to provide a strong conclusion based on reliable evidence. The study included 4 standardized RCTs and 2 nonrandomized studies with a total sample size of 1824 patients of a wide range of ages. The large sample size and age ranges allow the study to be more representative of the general population, providing a better perspective and understanding. However, the current study also had some limitations. The search strategy only yielded 6 studies, which also lacked the statistical power to reach appropriate conclusions regarding the effectiveness of coblation compared to traditional tonsillectomy. Due to the nature of the treatment being studied, double-blind randomization was not possible. In addition, included studies contained heterogeneous populations in terms of ages, surgical indications, and types of procedures. Furthermore, uncontrollable variables, such as the “skill level” of surgeons performing such operations, may have influenced the outcomes.
Conclusions
Although the evidence is limited with only 6 studies comparing coblation and bipolar diathermy, the results of this meta-analysis suggest that coblation does not improve or worsen the outcomes in adult patients undergoing tonsillectomy as it has similar hemorrhage cases and comparable postoperative pain scores, while also lengthening the operative time. The authors suggest further clinical studies to be performed to determine whether coblation has any superior clinical benefits.
Supplemental Material
Supplemental Material, sj-doc-1-ear-10.1177_0145561321994995 - Tonsillectomy Outcomes for Coblation Versus Bipolar Diathermy Techniques in Adult Patients: A Systematic Review and Meta-Analysis
Supplemental Material, sj-doc-1-ear-10.1177_0145561321994995 for Tonsillectomy Outcomes for Coblation Versus Bipolar Diathermy Techniques in Adult Patients: A Systematic Review and Meta-Analysis by Abdulmalik Alsaif, Mohammad Alazemi, Narvair Kahlar, Mohammad Karam, Ahmad Abul, Abdulrahman Al-Naseem, Abdulredha Al Muhanna and Turki Aldrees in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
Abdulmalik Alsaif, Abdulrahman Al-Naseem, Abdulredha Al Muhanna, Ahmad Abul, and Mohammad Karam did data acquisition. Abdulmalik Alsaif, Ahmad Abul, and Mohammad Karam contributed to data analysis and interpretation. Mohammad Al Azemi, Narvair Kahlar, and all the other authors contributed to drafting the manuscript. Ahmad Abul and Mohammad Karam did study concept and design. Turki Aldrees did study supervision and logistic support. All authors read and approved the final manuscript. Abdulmalik Alsaif and Mohammad Alazemi contributed as co-first authors. The data sets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.