
Abstract
Introduction:
Twenty percent of the total lithiasis that affect a major salivary gland will be found in the parotid gland. An exclusive sialoendoscopic approach has achieved success rates close to 80%. In a significant percentage of these remaining cases, combined transfacial approaches assisted by sialendoscopy are presented as an option to be taken into account.
Patients and Methods:
A prospective analysis of cases treated by combined transfacial approach assisted by sialendoscopy for lithiasis of the parotid gland and the impact of the facial nerve stimulator used during surgery.
Results:
Five patients were included; all of them operated satisfactorily. In 4 of them, the approach proposed by McGurk and modified by Capaccio was used, and in 1 of them, the approach proposed by Nahlieli was used. We suffered a complication in just case due to the appearance of postoperative sialocele.
Conclusion:
According to our results and those previously published, the transfacial approach assisted by sialendoscopy can be considered a useful technique. Proper planning ensures an optimal result in the treatment of parotid gland lithiasis. The use of facial nerve stimulator guarantees extra security when working near to a branch of the facial nerve is suspected.
Introduction
Obstruction in the parotid gland is usually manifested as edema and pain that could get worse with meals. Common causes described are lithiasis, ductal stenosis, and plugs secondary to mucus retention. 1 Although lithiasis represents more than 60% of all cases of salivary gland obstruction, 2 only 20% occur in the Stensen duct. 3
Sialendoscopy is a minimally invasive technique that has evolved significantly in the last 2 decades, reaching success rates above 80%. 4 These could be achieved only using the sialoendoscope when we find a completely visible and floating lithiasis, usually less than 4 mm. 3 However, when the stone is bigger, primary extraction is not possible, being necessary to use other techniques such as intraductal lithotripsy or combined techniques. 5
In 2002, Nahlieli et al described the first case series in which a combined approach was used. The authors proposed to locate the lithiasis by endoscopic visualization or ultrasonographic localization to make a transfacial incision for its extraction. 6 In 2006, McGurk et al would add the use of a preauricular cutaneous flap to expose the parotid and remove the lithiasis. 7 In 2007, Marchal would describe the use of the facial monitor during surgery, 8 and in 2014, Capaccio et al brought the use of the lifting incision to improve aesthetic results. 9
In this article, we reviewed 5 cases treated at our department using this technique, emphasizing the advantage of the multiple variants described previously by other authors and proposing a new variation through the use of facial nerve stimulator during the gland dissection to avoid the damage of any facial nerve branch.
Materials and Methods
After approval of the ethics committee of our center, a pilot study to assess the safety and the feasibility of sialendoscopy-assisted transfacial approach in parotid gland sialolithiasis were conducted. We included 5 cases of parotid gland lithiasis that required a combined approach, through a sialoendoscopic location of the lithiasis combined with a transfacial approach for the stone removal between July 2017 and July 2018. Written informed consent from the patients was obtained before surgery. The inclusion criteria were palpable lithiasis at the level of Stensen duct; size equal or bigger than 7 mm, located by a radiological test (computed tomography scan or ultrasound); and clinical examination in the proximal portion of the main duct, in 1 of the secondary ducts or within the parenchyma of the parotid gland (Figure 1).
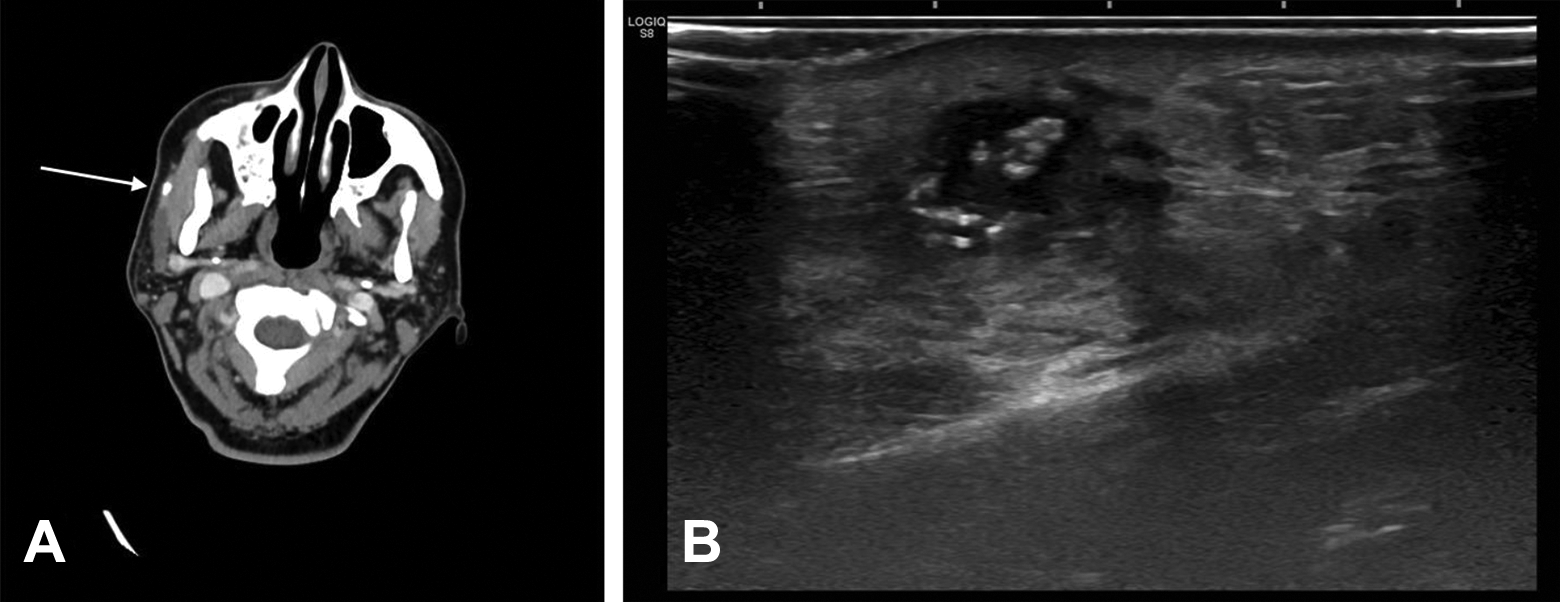
A, A CT scan where lithiasis can be seen over the masseter muscle. B, Ultrasound image of lithiasis within the parenchyma of the parotid gland complicated with parotid abscess. CT indicates computed tomography.
A descriptive analysis of each case was made, age, sex, lithiasis size, surgical time, postoperative stay, complications, and functional outcome were included.
The first step was to identify the Stensen duct based on the work of Toure et al. 10 To do this, we drew 2 lines that go from the tragal cartilage to the nasal ala and another to the labial commissure. Subsequently, we plotted the possible curved path of the Stensen duct, described by the authors in 3 segments; the first will run from the parotid gland to the masseter muscle, the second lateral to the masseter muscle, and the third lateral to the buccinator muscle. Based on this, we will define our work area, which we will contrast with the clinical examination, by palpation of the lithiasis and sialoendoscopic exploration by transillumination (Figure 2).
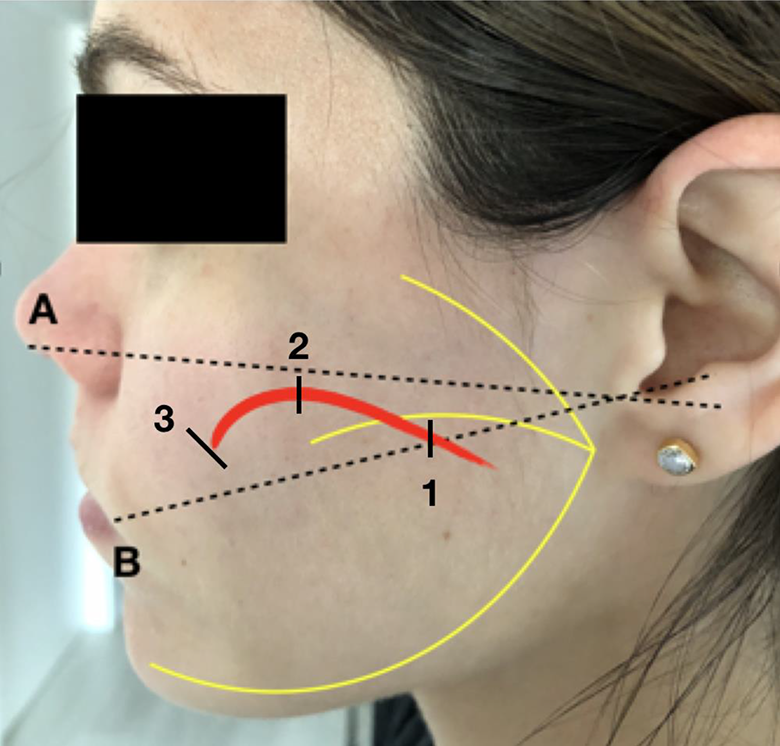
Topographic location of the Stensen duct. Line A, To the intertragal incisure to the base of the nostril. Line B, From the intertragal incisura to the labial commissure. The Stensen duct trajectory was divided into 3 segments: 1, the first segment lies between the parotid gland and the masseter; 2, the second lateral to the masseter; and 3, lateral to the buccinator.
All procedures were carried out under general anesthesia, using a facial nerve monitor (NIM-Response 3.0, Medtronic, Dublin, Ireland). After progressive dilatation of the Stensen caruncle (Marchal Dilator Set, Karl Storz Co, GmbH), we performed a sialoendoscopic evaluation of the entire ductal system using a 1.3 mm optic (Marchal sialendoscope, Karl Storz Co, GmbH). Once the lithiasis was located, the light from the tip of the optics was used as a guide to locate the lithiasis, and the skin was marked. Before start with the external approach, a Seldinger guidewire was left inside the duct to work as a guide to locate the lithiasis and visualize before opening the duct.
In 4 cases, the approach was performed according to the technique described by McGurk et al and modified by Capaccio et al. 7,9 The first step consists of making a preauricular incision, gently raising the skin flap and the parotid fascia to expose the superficial portion of the gland. Once exposed, the sialendoscopic evaluation is repeated to evaluate the Stensen duct, locate the lithiasis, and determine its position by transillumination. We verified the location of any branch of the facial nerve near to our working area using a facial nerve stimulator (Vari-Stim III, Medtronic). After dissecting the duct and defining the location of the lithiasis, we incised the Stensen duct with a disposable ophthalmological scalpel to extract the lithiasis. The duct was closed using 6-0 nylon. In those cases when an extensive ductotomy was required, a silastic stent was placed to avoid duct stenosis or sialocele formation. Finally, the duct was thoroughly checked by endoscopy to rule out the presence of residual stones (Figures 3 and 4). In 1 case, we used the approach described by Nahlieli et al. To do this, we located the lithiasis with the endoscope, and just above it, an incision and elevation of the skin were made followed by a delicate dissection of the parotid tissue until the duct was found. During the dissection, we verified the absence of facial nerve branches with the nerve stimulator. In this case, we did not suture the duct, just closing the glandular parenchyma directly. The use of aspiration drainage was not required in any case.

A, Lithiasis localization by sialendoscopic visualization. B, Preauricular incision and elevation of the skin flap. C, Closure.
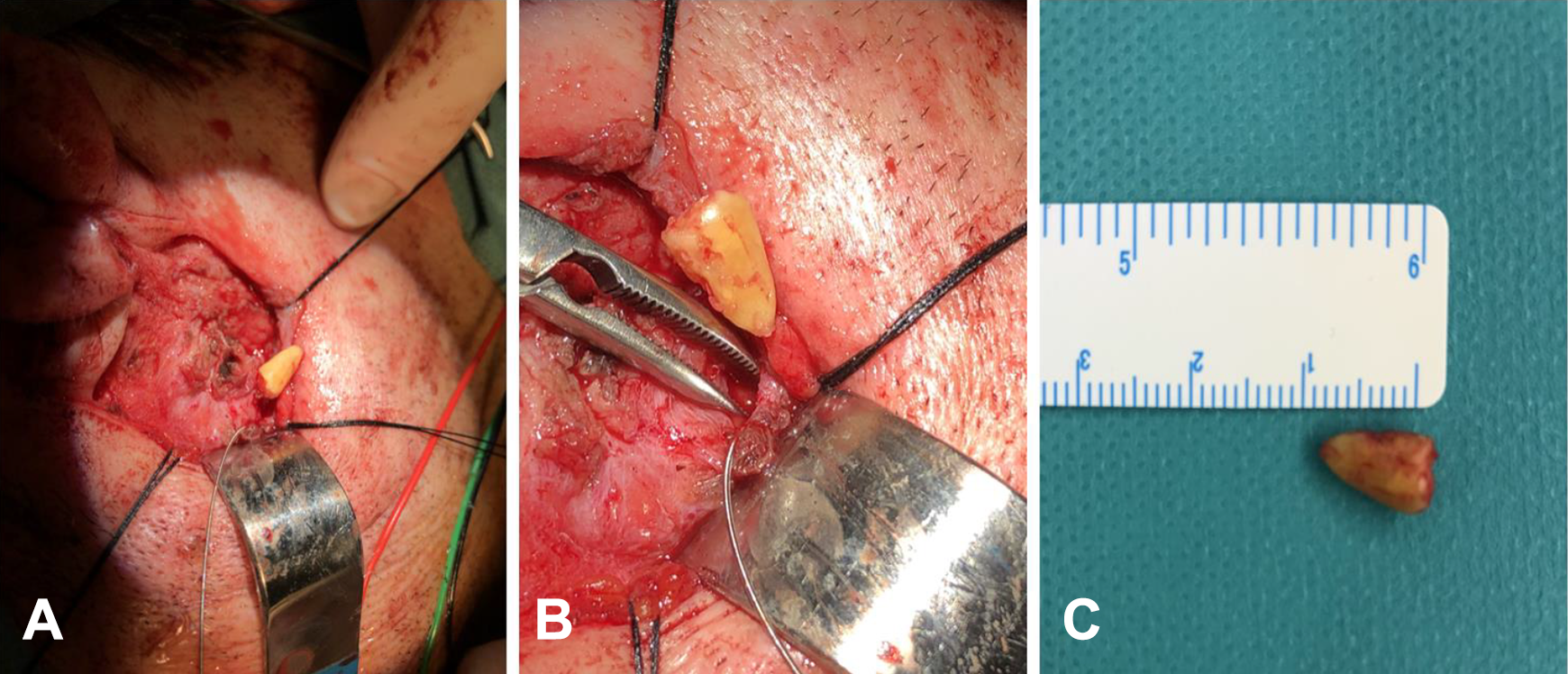
A, Surgical exposure for lithiasis extraction. B, Stensen duct opening, Seldinger guide visualization, and the extracted lithiasis. C, Lithiasis of 1 cm.
In the postoperative period, all patients were evaluated at 3 weeks and were followed up for at least 8 months. In the follow-up, the presence of residual symptoms and the outflow of salivary flow through the Stensen canal were evaluated.
Results
Five patients were operated during this period (Table 1). Three of them were women, and 2 were men. The mean size of the stones was 10.6 mm (minimum [min]: 7 mm/maximum [max]: 19 mm). In all cases, the size of the stones made not possible their primary extraction. According to lithiasis location: in 1 patient was in the proximal Stensen duct; in another patient, it was above the masseter muscle, other immediately after the masseter muscle; and in 2 patients, the stone was located in the gland parenchyma. In 1 case, the patient came to the clinic for the first time with a parotid gland abscess secondary to intraparenchymal lithiasis (Figure 1B).
Clinical Data of Patients Operated by Combined Approach.
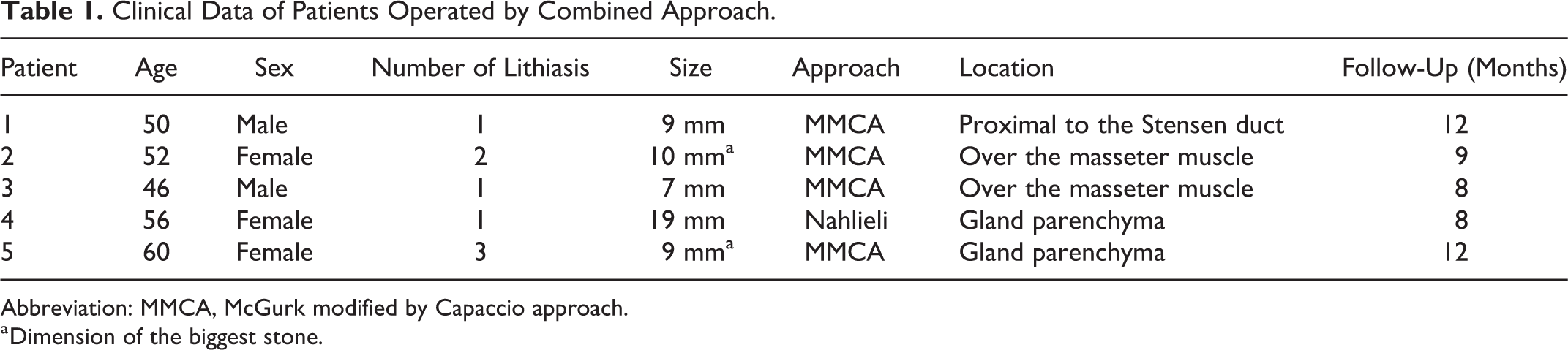
Abbreviation: MMCA, McGurk modified by Capaccio approach.
a Dimension of the biggest stone.
All the procedures were successful and proceeded without incident. The mean operative time was 131 minutes, with a range of 120 to 165 minutes. Mean hospital stay was 1.8 days (min: 1/max: 5), 4 patients were discharged 1 day after surgery, and 1 patient needs to stay in the hospital for 5 days to manage a sialocele complication. No facial nerve or greater auricular nerve (GAN) lesion was observed. All the patients presented glandular edema, which disappeared progressively. During the follow-up, all patients presented a healthy functioning of the gland after the compressive massage. Regarding complications, 1 patient presented a sialocele, which was solved after 10 days with compression and drainage. No infection of the surgical wound or postoperative bleeding was observed. Regarding aesthetic results, patients were satisfied, and none of them had wound dehiscence or developed a hypertrophic scar.
Discussion
The development of minimally invasive surgical techniques for the management of parotid gland lithiasis allows surgeons to perform conservatives and gland sparing approaches rather than major surgery. Before the onset of sialendoscopy, the management of parotid gland lithiasis was limited to attempt its extraction using a transfacial or intraoral approach (according to the palpation or radiological image), a suprafacial parotidectomy (SP) or through conservative management waiting for the atrophy of the gland. 4
Today, those floating lithiases, smaller than 4 mm, can be handled mostly by sialendoscopy with excellent results. However, larger lithiasis (>7 mm) is usually fixed in sections of the ductal tree where the diameter is smaller than the stone, duct bifurcations, stenosis, or in the glandular parenchyma itself. In these cases, a simple endoscopic approach is not always feasible, and sometimes, we found more than 1 stone in the same gland. 9
Intraductal lithotripsy techniques, such as the holmium laser or the stone breaker, will allow the fracture of fixed lithiasis. In fragments, extraction can be easy, 11,12 being a good option in intermediate size stones (4-6 mm). However, in larger sizes, the lithotripsy time can become excessive, and the thermal or mechanical damage in the duct can lead to the stenosis formation.
In those cases where sialendoscopy or intraductal lithotripsy is not feasible, the combined approach represents a good option, guaranteeing the preservation of the gland and its function, with minimal aesthetic repercussion and with a low rate of complications.
The approach will depend on the lithiasis location. When the stones are located in the anterior edge of the masseter muscle, the combined approach will be more accessible through the jugal mucosa, using the so-called transoral combined sialolitectomy technique. Cases of lithiasis located more proximal to the gland, posterior to the anterior border of the masseter, will be treated by combined transfacial approaches.
Nowadays, we are facing a paradigm shift in the way we approach this pathology supported by multiple publications. Roland et al 4 recently published the first systematic review and meta-analysis concerning this technique. It has taken into account a total of 10 articles in which 184 patients were included. The authors report a success rate greater than 97% in lithiasis extraction, preservation of the gland, and disappearance of symptoms, reporting a complication rate of 6%, including children and adults. Regarding the type of complications, these corresponded to the appearance of sialocele, salivary fistula, hematoma, perforation of the duct, and infection of the surgical area.
Looking for a surgical alternative, we have the SP, a technique widely used in the management of tumors of the parotid gland and associated with well-known complications such as facial asymmetry, surgical scar, risk of paresis, or paralysis of the facial nerve and resection of a potentially functional gland. When dealing with the obstructive pathology of a functional disorder, it seems aggressive to perform a treatment like this in patients who might be candidates for a less aggressive technique as described in this article. After reviewing the indexed literature, we found 2 studies regarding SP in the treatment of lithiasis of the parotid gland, published by Bates et al 13 and another by Patel et al 14 ; in both studies, complication rates were 26.5% and 33%, respectively, regarding facial paresis and 1% of definitive paralysis.
The transfacial approach combined with the use of the endoscope represents an alternative, following the principle of minimally invasive surgery, in those cases in which the obstruction cannot be solved using the endoscope. In our series, we obtained a satisfactory result, being able to conserve the functionality of the gland during the follow-up time and evidencing only 1 major complication, due to the appearance of sialocele. To avoid the damage of any branch of the facial nerve, it is essential to consider the use of the facial nerve monitoring as other authors have previously described. 7 Moreover, the use of facial nerve stimulator guarantees extra security when suspect we are facing any of the facial nerve branches, systematically to avoid any risk over them. In our series, none of the patients presented any facial nerve damage. To avoid an inadvertent injury of the GAN, a careful dissection of the posterior and inferior region of the earlobe in its entrance area is mandatory. With this precaution, in none of the 4 cases in which we have used the McGurk approach, modified by Capaccio, GAN lesions have occurred.
Finally, we need to address some limitations of our study as the limited number of patients and the short follow-up period. However, after this positive initial experience, we continue to perform this procedure at our department and including all the data (functional outcomes, complications, etc) in our salivary gland database in order to create a larger study in the future to further evaluate this technique.
Conclusion
According to our results and those previously published, the transfacial approach assisted by sialendoscopy can be considered a useful technique. Proper planning ensures an optimal result in the treatment of parotid gland lithiasis. Also, the use of the facial nerve stimulator guarantees extra security when suspect we are working near a branch of the facial nerve.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.