
Abstract
Introduction:
The objectives of this investigation are to characterize the epidemiology of base of tongue adenocarcinoma utilizing a population-based database and to identify prognostic factors that may affect survival.
Methods:
A retrospective cohort study was conducted using the Surveillance, Epidemiology, and End Results database. Univariate Kaplan-Meier analysis and multivariate Cox-regression analysis were performed to evaluate the association of suspected prognostic factors with survival. Overall survival (OS) and disease-specific survival (DSS) were the primary outcome measures.
Results:
A total of 176 cases were eligible based on inclusion criteria. The 5-year OS and DSS were 49% and 66%, respectively. On multivariate analysis, surgical management was associated with improved OS and DSS (OS hazard ratio [HR]: 0.34, 95% confidence interval [CI]: 0.20-0.58, P < .001; DSS HR: 0.20, 95% CI: 0.09-0.48, P < .001), while higher tumor grade was associated with worse OS and DSS (OS HR: 1.58, 95% CI: 1.14-2.19, P = .006; DSS HR: 1.68, 95% CI: 1.01-2.79, P = .045). Administration of chemotherapy or radiation did not have a significant association with OS or DSS.
Conclusion:
This investigation is the largest to date to analyze the base of tongue adenocarcinoma as its own entity. Surgery remains the mainstay of treatment, and lower tumor grade is associated with improved survival in these patients. Administration of radiation or chemotherapy was not associated with improved survival.
Introduction
Oropharyngeal cancers represent approximately 3% of all new cancer cases in the United States. 1 Anatomic locations in this group include soft palate, base of tongue (BOT), lingual tonsil, and palatine tonsil. Incidence of squamous cell carcinoma (SCC) of the oropharynx has dramatically increased in the United States in the past 40 years and is associated with human papillomavirus (HPV) related disease. 2 However, other histologic types of oropharyngeal cancers are not associated with HPV infection and require further study for prognostic and treatment guidelines. Minor salivary gland carcinomas are found predominantly in the BOT, soft palate, or tonsil but are not typically associated with HPV infection and subsequent p16 upregulation. 3,4 Among the minor salivary gland carcinoma histologic subtypes, adenocarcinoma has been identified but little prognostic or treatment guideline information is available for these cancers occurring in the oropharynx, specifically the BOT.
Options for the resection of oropharyngeal tumors have evolved and, depending on the tumor, patients can be considered for transoral or transcervical approaches. Historically, mandibulotomy or transcervical transhyoid procedures with pedicled or free flap reconstruction have been used. These approaches have increased morbidity due to the route of tissue mobilized to allow for proper exposure of the pharynx. Recently, transoral robotic surgery (TORS) has become an effective surgical tool for the treatment of lesions of the pharynx and tongue base. Patients in which TORS is utilized as part of a treatment paradigm for oropharyngeal cancer have been found to have an improved quality of life and function as compared with nonsurgical treatment of oropharyngeal cancer and those treated with traditional surgical approaches. 5 -7 In addition, TORS allows for oncologic resections, with proper patient selection, and less morbidity compared with traditional surgical approaches. 8 The National Comprehensive Cancer Network 2018 guidelines for p16 negative, typically HPV-negative cancers, describe definitive radiation therapy (RT), transoral or open tumor resection, or induction chemotherapy with RT for treatment of this group of tumors. 9 However, further study is needed to provide evidence-based guidelines within this group of neoplasms, especially for non-SCC pathologic types. 9 As surgery continues to advance, there is opportunity to treat BOT cancers with advanced techniques, but evidence for particular types of cancers is required for appropriate recommendations.
This study aims to utilize population-level analysis to characterize BOT adenocarcinomas. This study aims to further characterize epidemiology and prognostic factors for BOT adenocarcinoma.
Patients and Methods
A population-based cohort analysis was performed utilizing the Surveillance, Epidemiology, and End Results (SEER) 18 database, including cancer cases from 15 states across the United States from 1973 to 2014. This database is maintained by the National Cancer Institute and contains publicly available, deidentified case information. Because of these qualities, no Rush Institutional Review Board review was necessary.
Cases were queried by primary site, C01.9 (BOT) and histologic type. Histology codes from the International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3) included 8140 (adenocarcinoma NOS), 8141 (scirrhous adenocarcinoma), 8147 (basal cell adenocarcinoma), 8211 (tubular adenocarcinoma), 8260 (papillary adenocarcinoma NOS), 8290 (oxyphilic adenocarcinoma), 8310 (clear cell carcinoma, not otherwise specified [NOS]), 8450 (papillary cystadenocarcinoma), 8480 (mucinous adenocarcinoma), 8481 (mucin-producing adenocarcinoma), 8525 (polymorphous low grade adenocarcinoma), 8550 (acinar adenocarcinoma), 8560 (adenosquamous carcinoma), and 8574 (adenocarcinoma with neuroendocrine differentiation).
Variables extracted for each case included race, gender, age at diagnosis, tumor grade, tumor histology, tumor size (American Joint Committee on Cancer [AJCC] T stage), nodal involvement (AJCC N stage), presence of distant metastases (AJCC M stage), radiation administration, chemotherapy administration, and surgical resection. The outcome measure of this study was survival, which was calculated from the date of diagnosis of malignancy to whichever of the following occurred first: date of death, date of the last follow-up, or end of the study period (December 31, 2014). Both overall survival (OS) and disease-specific survival (DSS) were assessed for each patient; OS was defined as the time from diagnosis to death from any cause, while DSS was defined as the time from diagnosis to death directly attributable to the primary malignant tumor. Any patients lost to follow-up were coded as censored observations.
Statistical analysis was performed with SPSS software (version 22; IBM Corporation, Armonk, New York). Univariate Kaplan-Meier analysis was performed to evaluate the association of prognostic variables with survival; each association was analyzed using the log-rank test and was deemed statistically significant at the P < .05 level. Multivariate Cox proportional hazards regression analysis was subsequently performed to test significant predictors. The number of variables that could be included in the multivariate analysis was computed based on a ratio of 10 events per variable.
Results
Patient Characteristics
A total of 176 patients with BOT adenocarcinoma were included in the study cohort (Table 1). The mean age of patients was 61.9; males comprised 58.0% of the sample, and the cohort was predominantly white (84.1%). The most commonly specified histology was adenosquamous carcinoma (16.5%), and tumors were most commonly moderately differentiated (31.3%). With regard to treatment, most patients received surgery (54.0%) and radiation (55.1%) but not chemotherapy (22.7%).
Patient Demographics, Tumor Characteristics, and Univariate Analysis of Overall Survival and Disease-Specific Survival.
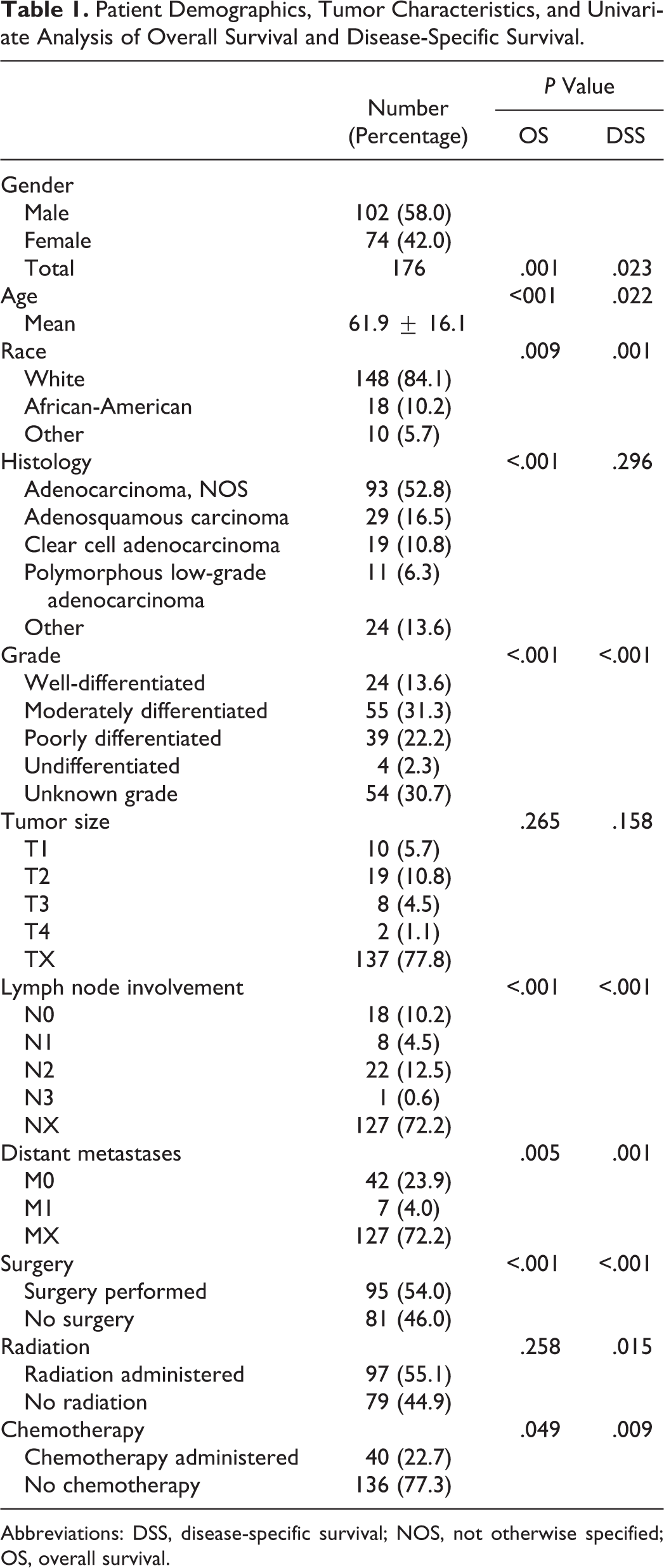
Abbreviations: DSS, disease-specific survival; NOS, not otherwise specified; OS, overall survival.
Univariate Analysis
The 5-year OS and DSS were 49% and 66%, respectively (Figures 1 and 2). The results of the univariate Kaplan-Meier analysis are depicted in Table 1. Log-rank tests suggested that OS was predicted by gender (P = .001), age (P < .001), race (P = .009), histology (P < .001), grade (P < .001), lymph node involvement (P < .001), distant metastases (P = .005), surgery (P < .001), and chemotherapy (P = .049). Disease-specific survival was predicted by gender (P = .023), age (P = .022), race (P = .001), grade (P < .001), lymph node involvement (P < .001), distant metastases (P = .001), surgery (P < .001), radiation administration (P = .015), and chemotherapy (P = .009).
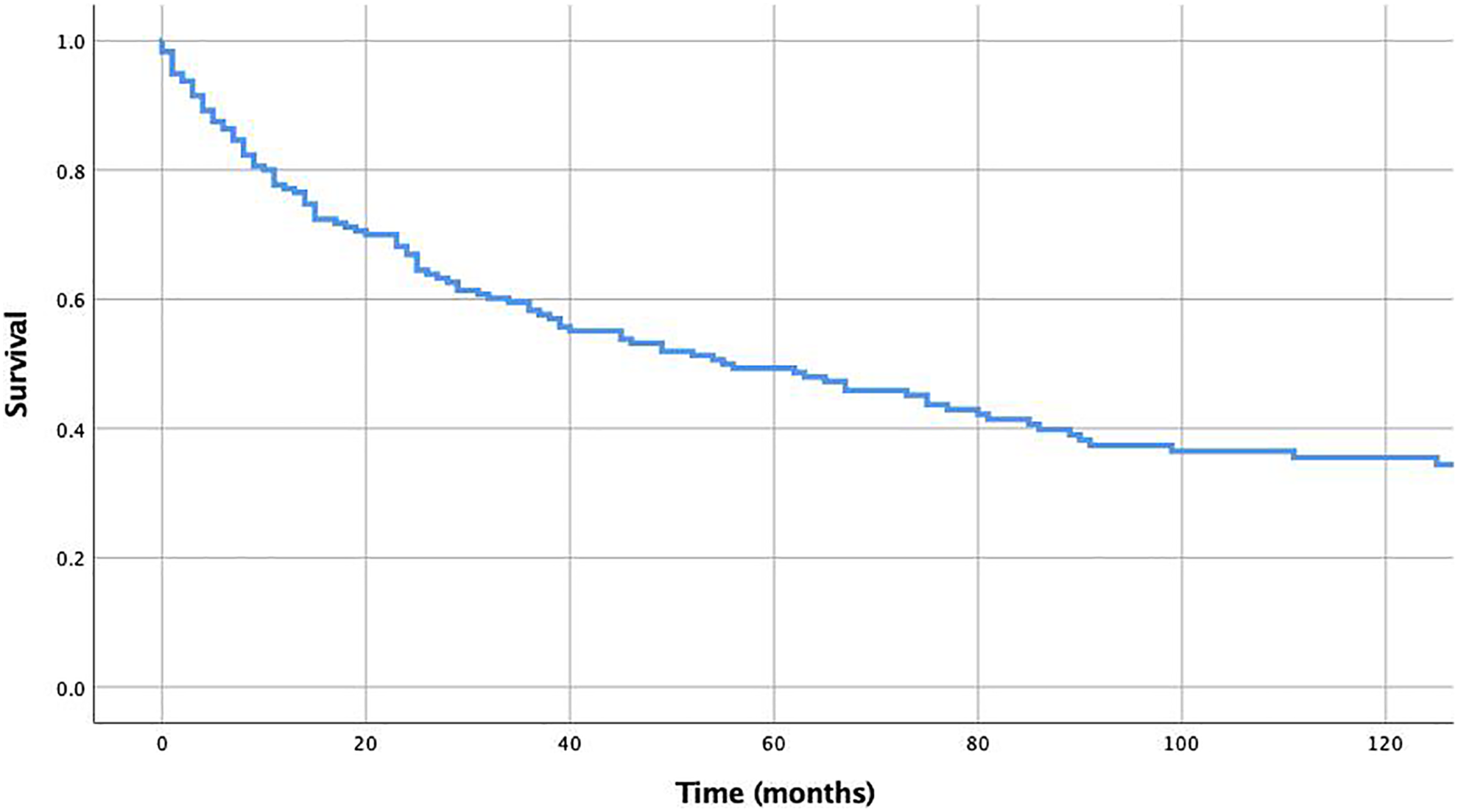
Kaplan-Meier analysis of overall survival.
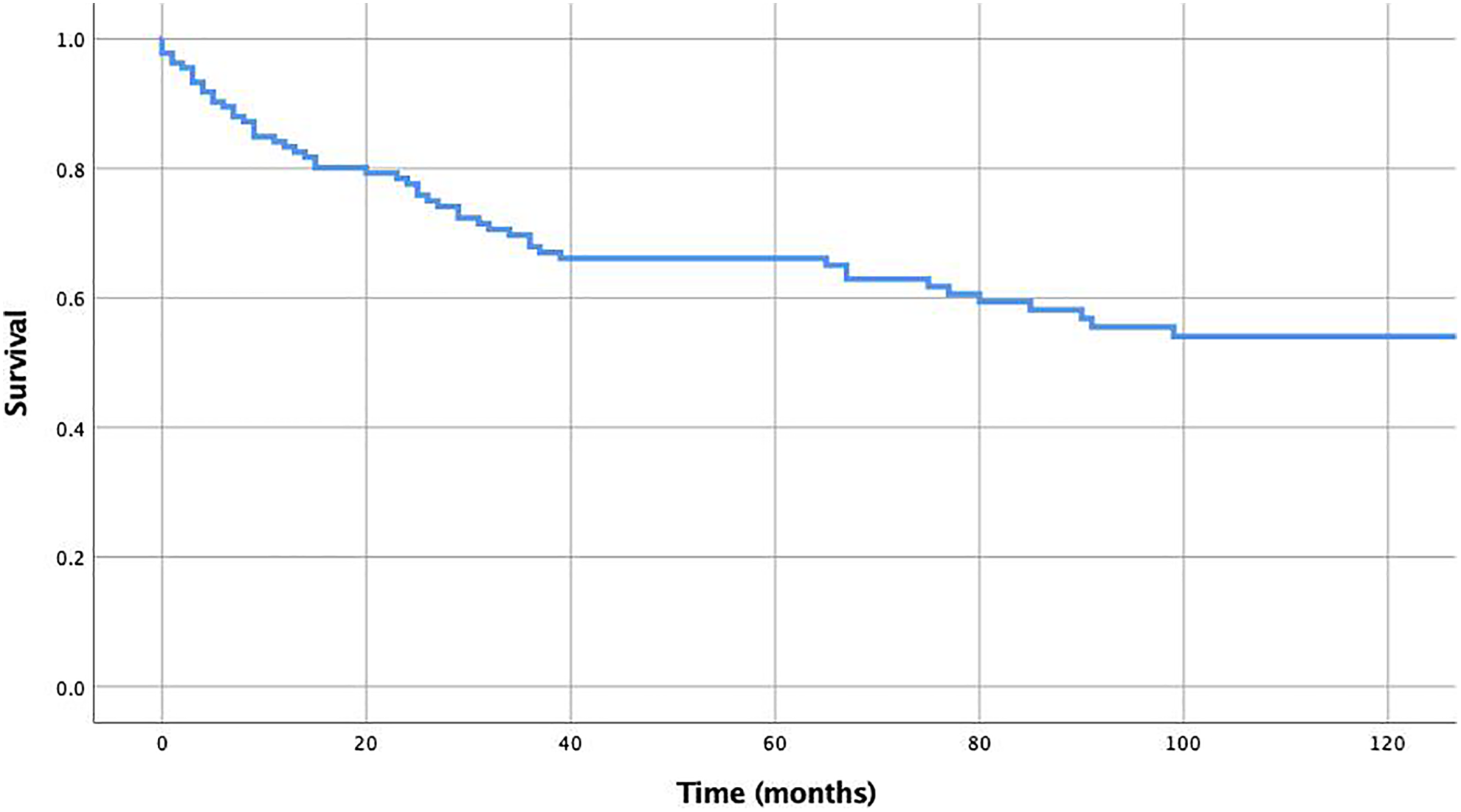
Kaplan-Meier analysis of disease-specific survival.
Multivariate Analysis
The results of multivariate Cox-regression analysis are depicted in Table 2. Based on the number of events in the data set, it was determined that a maximum of 4 variables could be included in the analysis to maintain 10 events per variable ratio and ensure accuracy of the statistical model. Given the investigation’s focus on treatment variables, we sought to include surgery, radiation administration, and chemotherapy administration in the multivariate model; additionally, staging variables were excluded despite their significance on univariate analysis because the majority of cases did not have staging data available. On multivariate analysis, surgical management was associated with improved OS and DSS (OS hazard ratio [HR]: 0.34, 95% confidence interval [CI]: 0.20-0.58, P < .001; DSS HR: 0.20, 95% CI: 0.09-0.48, P < .001) while higher tumor grade was associated with worse OS and DSS (OS HR: 1.58, 95% CI: 1.14-2.19, P = .006; DSS HR: 1.68, 95% CI: 1.01-2.79, P = .045). Administration of chemotherapy or radiation did not have a significant association with OS or DSS.
Multivariate Cox-Regression Analysis of Selected Predictors of Overall Survival and Disease-Specific Survival.

a Values are presented as hazard ratios (95% confidence interval).
Discussion
Tongue base adenocarcinoma is a rare pathology of the head and neck and treatment recommendations are unclear. Limited evidence is available and the various approaches that are offered are usually institution dependent. This investigation is the largest to date to analyze BOT adenocarcinoma as its own entity. Our univariate analysis of data demonstrated surgery and chemotherapy as significant variables associated with increases in DSS months. However, many case entries in the database did not specify the specific type of surgery performed, so further case-specific information would be useful to draw broader conclusions on surgical approaches. With the improving technology in transoral laser and robot-assisted surgery, more BOT surgeries that spare surrounding structures are possible. The data from this study support a survival benefit with surgical treatment, which may be able to be applied to more patients given the advances in surgical technology. Understanding the utility of these various modalities is important for oncologic planning to determine an effective treatment approach for patients with this rare tumor.
Radiation therapy was not a significant variable in increased overall or DSS months for BOT adenocarcinoma. In multivariate analysis, surgery and tumor grade were found to be significant variables for both OS and DSS. This is useful information to discuss treatment plans for patients with these rare cancers, although the limitations of a retrospective cohort study must be kept in mind. Although RT for minor salivary gland carcinomas has been studied in retrospective cohorts among many histologic subtypes and anatomic sites, it is challenging to draw specific conclusions about tongue base adenocarcinoma. In a study of 52 patients, RT plus surgery was found to have improved local control rates compared to primary RT in advanced stage minor salivary gland carcinomas. 10 However, in early stage cancers, there was no significant difference between the treatment groups. This may indicate a difference in survival benefit from RT based on tumor stage. This was supported by a single-institution retrospective analysis of patients with minor salivary gland carcinoma in which tumor stage was a strong predictor of locoregional and distant control. 11 Another single-institution retrospective analysis found significantly improved locoregional control in minor salivary gland carcinoma with adjuvant RT, except within the adenocarcinoma subtypes, demonstrating the difference in characteristics among tongue base neoplasms. 12 A significantly higher rate of failure with radiation treatment was found between patients treated before 1990, as compared with those treated after. 11 As the SEER database includes data from 1973 but does not indicate in which year the patient received RT, the difference in RT technologies over time may have affected the results of this study. The optimal treatment for oropharyngeal adenocarcinoma is not clear and radiation is likely to benefit certain patients, but the indications for this treatment are not clear.
The current study has limitations that are intrinsic to a study utilizing the SEER database. More detailed information about treatment modalities, including the timing of treatment following diagnosis, surgical margin status, the dosage of radiotherapy, and details of chemotherapy administration, is unavailable in the SEER database and, therefore, could not be analyzed as part of this study. In addition, this article, like most SEER studies, relies on the accuracy of records compiled in the database. In this regard, institutional-based chart review and prospective studies may be stronger compared with retrospective cohort studies. Finally, despite utilizing a large database to study BOT adenocarcinoma, this study includes relatively few cases compared to other major cancer subtypes, making this study underpowered inherent to the incidence of this disease.
Further information about extent and regimen specifications for RT and surgical approaches, such as intensity-modulated radiation therapy (IMRT), and neck dissection, would be useful to further characterize the utility of these treatments. The inability to stratify DSS based on the presence of neck dissection in the surgery performed adds another limitation to this study. The N status was determined but given the structure of the database, it remains unclear if this is clinical, as determined by the radiographic presence of nodes, or pathologic, as determined by the classification of nodal status after neck dissection. This would be useful to clearly compare these results with other studies as the nodal component of staging can change drastically after surgery.
Future directions in studying BOT adenocarcinoma include investigating the presence of predilection for regional metastasis to understand the role of neck dissection in these cases. The BOT has bilateral cervical lymph node drainage and involves the upper two-thirds of the jugular lymphatic chains. 13 Due to this bilateral lymph drainage, BOT squamous cell carcinoma typically necessitates bilateral neck dissection and/or RT to bilateral neck lymph node basins. Understanding the potential for regional metastasis in BOT adenocarcinoma would be instrumental to guide specific surgery and radiation planning. As more cases become available in population-based databases, further investigation of treatment modalities including information on combinations of surgery and other treatment options would provide clearer data to further identify risk factors and guide BOT adenocarcinoma treatment.
Conclusion
Base of tongue adenocarcinoma is a rare subtype of oropharyngeal cancer that was studied utilizing population-level analysis. Multivariate analysis demonstrated significant associations of surgical treatment and lower tumor grade with increased survival, whereas the association with RT was not significant. The results prompt further study to understand appropriate treatment guidelines, including the utility of RT and determination of surgical approach for BOT adenocarcinoma. Multidisciplinary teams are necessary for devising treatment plans for patients with BOT adenocarcinoma due to the rare nature of this disease and variety of available treatment modalities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.