
Abstract
Osteomas are rare benign bony tumors located in the tongue area. In most cases, patients presenting with a lingual osteoma are asymptomatic but may complain of the sensation of having a foreign body. Fewer than 100 cases of lingual osteoma have been reported worldwide. Here, we present 2 cases of tongue base osteoma that were treated with excision under a laryngoscope.
Introduction
Osteomas are benign bony tumors that consist of normal mature osseous tissue. They are often found in the flat bones of the skull and face, without specific clinical symptoms, and are rarely found in the intraoral region. Moreover, fewer than 100 cases of lingual osteoma have been reported since Monserrat first used the term “lingual osteoma.” 1 Because of its rarity, here we present 2 cases of tongue base osteoma that occurred in a 27-year-old man and a 23-year-old man. The epidemiology, clinical presentation, and underlying pathogenesis of this condition are also discussed.
Case 1
A 27-year-old man, without any underlying disease, presented with an intermittent sensation of a lump in the throat for 3 months. There were no complaints of odynophagia, dysphagia, blood-tinged sputum, or body weight loss. Fiberscopy revealed a well-defined, smooth-surface mass over the midline junction of the tongue and tongue base (Figure 1A). The head and neck regions were normal. No cervical masses or lymphadenopathy were found. Under the impression of a benign tongue base tumor, the mass was excised by laryngomicrosurgery under general anesthesia. The mass measured 0.8 cm × 0.5 cm × 0.5 cm and was hard to palpate. Tumor section was composed of mature bone trabeculae covered by fibrous stroma and overlying squamous epithelium (Figure 1B and C). A diagnosis of osteoma was confirmed.
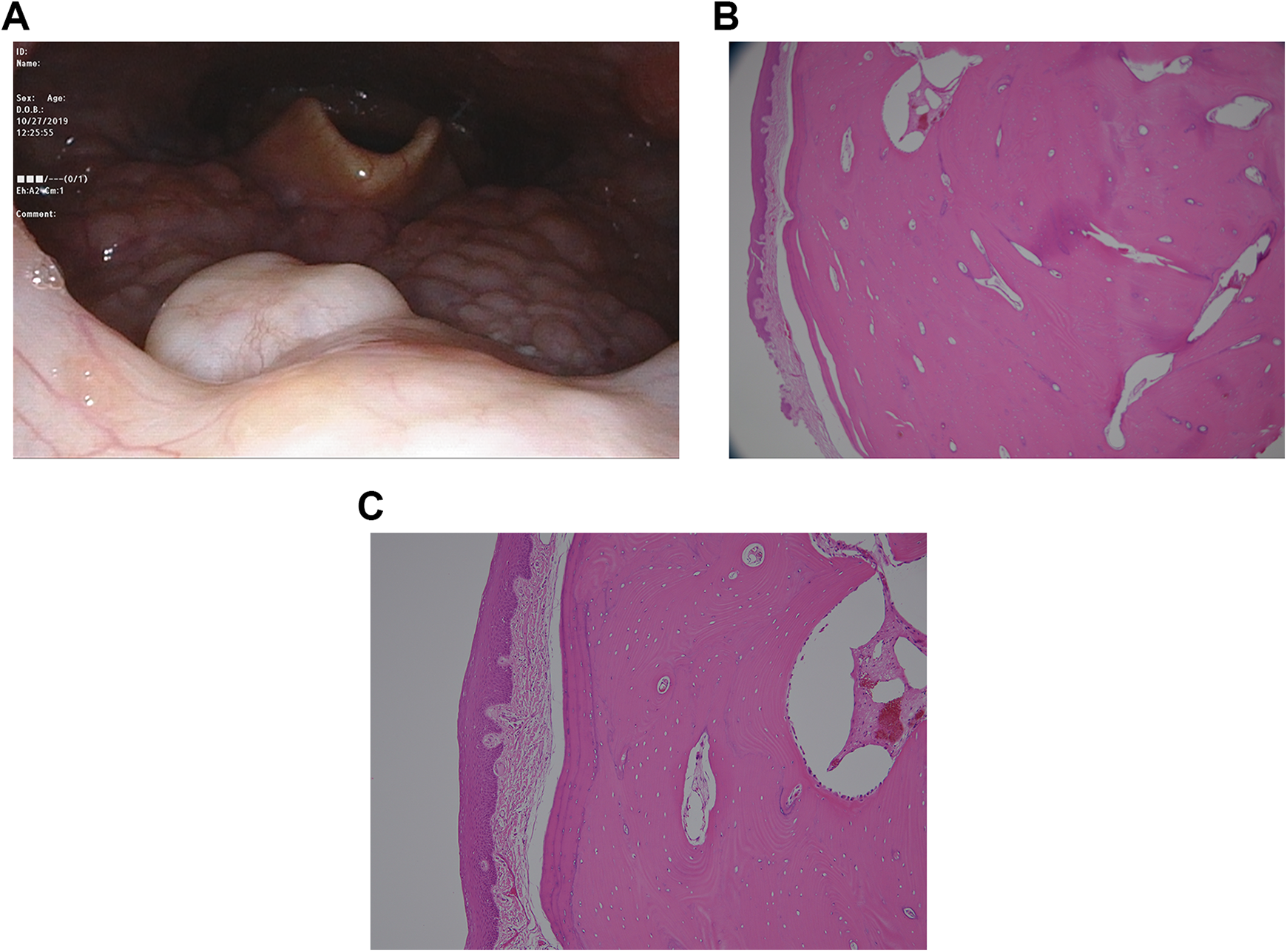
A, Case 1: Mass was found on the right side of the tongue base. B and C, Mature bone surrounded by fibrous stroma and lined with stratified squamous epithelium under ×40 (B) and ×100 (C) microscopic magnification, with H-E stain.
Case 2
A 23-year-old man, without any underlying disease, found a firm lesion over the left side of the dorsal tongue by himself while brushing his teeth. Other symptoms included a mild sensation of having a lump in the throat and minimal oral bleeding. There were no complaints of odynophagia or dysphagia. He visited our outpatient department, and an intraoral examination and fiberscopy were performed. It revealed a solid mass (0.8 cm × 0.7 cm) over the left side of the tongue base (Figure 2A). No other abnormalities were found over the head and neck regions. Under the impression of a benign tongue base tumor, the mass was excised by laryngomicrosurgery under general anesthesia. The mass measured 0.8 cm × 0.7 cm × 0.5 cm (Figure 2B). Tumor section was composed of woven bone formation surrounded by inflamed fibrous tissue. There was no evidence of malignancy. A diagnosis of osteoma/osseous choristoma was confirmed.
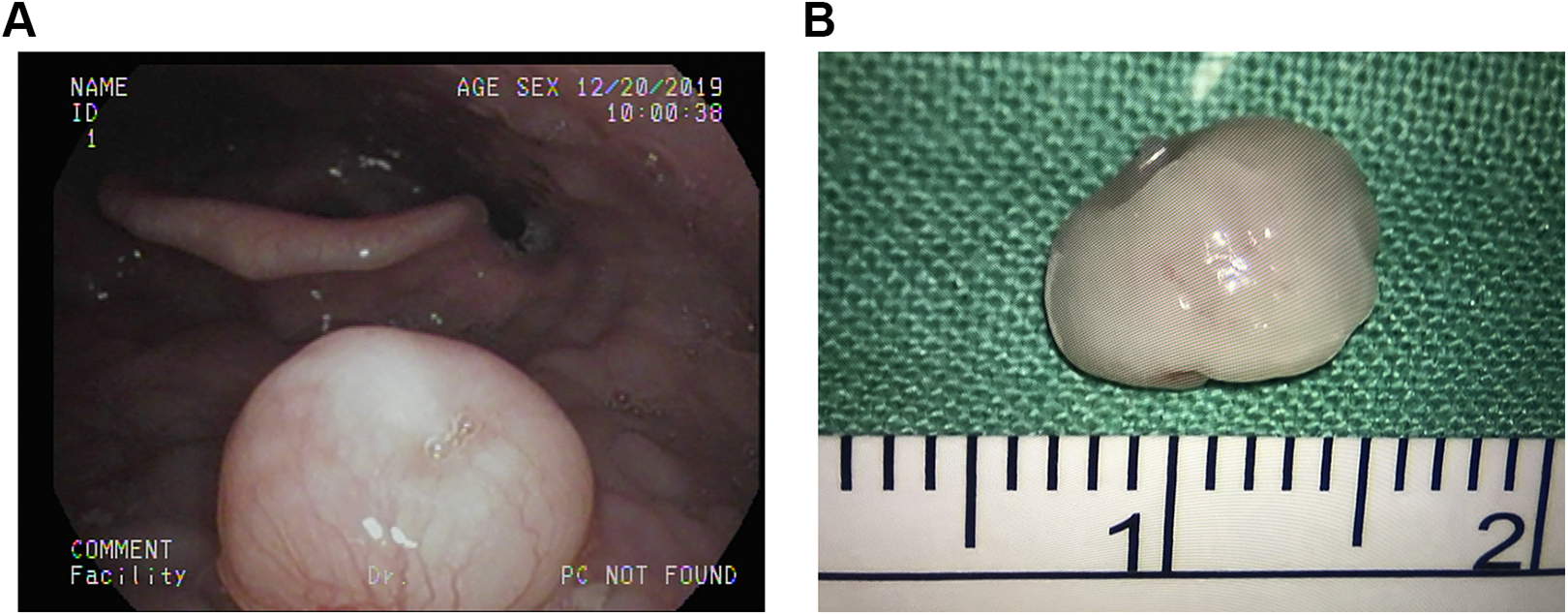
A and B, Case 2 mass was found on the left side of the tongue base.
Discussion
In 1913, Monserrent was the first to describe a bony tumor forming in the tongue of an individual. Since then, fewer than 100 cases have been reported to our knowledge. Osteomas of the tongue occur more frequently in women (male:female ratio, 16:44). 2 One literature review showed that the patient age range was from 5 to 73 years (mean, 28.7 years), and the majority of cases occurred in the second or third decades of life. 2 The lesions are most commonly located in the posterior third of the dorsal tongue, foramen cecum, and circumvallate papillae (90%), and 10% are on the middle third of tongue. The remaining cases are located on the lateral side of the tongue. 1 In most cases, the patients are asymptomatic but may complain of having a foreign body sensation in the throat (25.8%), dysphagia (6.9%), gagging (5.1%), nausea (3.4%), and irritation (3.4%). 1 Although the pathogenesis of lingual osteoma is still unknown, several theories have been published, as discussed below.
Branchial Arch Persistence Theory 3
This theory considers the lingual osteomas to be ossified branchial arch remnants. During embryological development, the anterior two-thirds of the tongue originates from the first branchial arch, whereas the posterior third of the tongue originates from the third branchial arch. The 2 parts of the tongue fuse at the region of the foramen cecum and the sulcus terminalis. 4 Certain normal osseous structures originate from these branchial arches through endochondral ossification (first branchial arch: incus and malleus; second branchial arch: stapes, styloid process, and lesser horn of the hyoid bone; and third branchial arch: the remainder of the hyoid bone). This theory may explain the location of osteomas, but it fails to explain the predilection for women.
Lingual Thyroid Remnant Ossification Theory5,6
The thyroid gland arises at the foramen cecum and descends into its normal position in the neck. If there is an undescended thyroid remnant, regardless of differentiation, the tissue may ossify to form a lingual osteoma during puberty. The incidence rate of lingual thyroid tissue remnants and embryologically displaced intralaryngeal thyroid tissue are predominant in women, as along with lingual osteomas. This may support this theory, but so far, no thyroid tissue has been found in current specimens.
Posttraumatic Reaction Theory 1
This theory considers that the posterior third of the tongue is susceptible to frequent irritation (swallowing, articulation, or trauma). This may cause local inflammation with deposits of calcium, which later leads to calcification. This theory is similar to “myositis ossificans,” a condition whereby heterotopic ossification occurred inside muscle or other soft tissue after mechanical injury. However, posttraumatic ossification, such as myositis ossificans, usually lacks the Haversian system; whereas, lingual osteomas contain fully developed bone with the Haversian system.
The term “osteoma” is also controversial. Osteoma is usually defined as a benign progressively enlarging neoplasm of bone, originating from osteogenic tissue, and is closely associated with the skeleton. When these criteria are applied to lingual osseous lesions, no close relationship between the lesion and the skeleton or a proven osteogenic origin can be found. In addition, not all lingual lesions display a growth tendency. For these reasons, the term lingual osteoma does not strictly fit the criteria of osteoma. Krolls et al 7 suggested the term “osseous choristoma of the tongue.” By definition, a choristoma is a developmental tumor-like growth of microscopically normal tissue in an abnormal location. Osseous choristoma refers to heterotopic mature bone within soft tissues, either the skin (previously known as osteoma cutis) or the mucosa of the oral cavity (known as osteoma mucosae or soft tissue osteoma).
Treatment
Lingual osteomas are usually treated with surgical excision. Although recurrent cases of intraoral osteoma have been reported,8,9 no recurrence has been reported in the tongue. No cases of malignant transformation have been reported.
Conclusion
A lingual osteoma is a rare benign tumor. It is most commonly found in the posterior third of the dorsal tongue, close to the foramen cecum. The pathogenesis of lingual osteoma remains unclear. Surgical excision is the main treatment choice and shows good prognosis and low recurrence rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.