
Abstract
Objective:
Vitamin B12 deficiency-induced hyperhomocysteinemia has been associated with impaired microarterial flow, demyelization, and neuronal damage, resulting in cochlear damage and auditory dysfunction. Therefore, we aimed to evaluate the possible vestibular-evoked myogenic potential (VEMP) abnormalities in patients with vitamin B12 deficiency.
Material and Method:
In this prospective study, 37 patients diagnosed with vitamin B12 deficiency (<220 pg/mL) were compared with 31 audiologically healthy participants with normal B12 levels. Burst-evoked cervical VEMP (cVEMP) measurements were performed on all participants. Additionally, cVEMP responses were analyzed for P1-N1 latency, interpeak amplitude, and amplitude asymmetry ratio. The results of audiometric examination and VEMP records as well as absent responses were evaluated and compared between groups.
Results:
The rate of absent VEMP responses was twice as high in the patient group than in the healthy control group (12 vs 6 cases, respectively). Moreover, the mean values of interpeak amplitude in both right and left ears were statistically shorter in the patient group than the control group (P values = .024 and .007, respectively). Similarly, the mean amplitude asymmetry ratio was statistically higher in the patient group than the control group (P = .050). There were no statistically significant differences in latency responses between groups. Furthermore, positive, statistically significant correlation was detected between values of the left P1-N1 interpeak amplitude and vitamin B12 levels (r = 0.287, P = .037).
Conclusions:
Increased rates of absent VEMPs and decreased amplitudes with normal latencies are attributed to peripheral vestibular hypofunction in patients with vitamin B12 deficiency.
Introduction
Micronutrient insufficiencies have been significantly associated with auditory problems and hearing loss in recent years. 1 Vitamin B12 is the cofactor of the methylation reaction, resulting in myelin synthesis. 2 Accumulation of homocysteine levels via vitamin B12 deficiency may cause vascular inflammation, reduced microvessel flow, and permeability. Thus, the reduced cochlear blood flow might result in atrophy of the stria vascularis. 1,3 Demyelinisation-associated axonal degeneration and apoptotic neuronal death caused by impaired methionine synthesis, which directly affects cochlear neurons, is well-known today. 3 In addition to neuronal damage, effects such as cellular oxidative stress, direct neurotoxicity, and vascular toxicity caused by auto-oxidation of elevated homocysteine have been demonstrated. Recently, vitamin B12 deficiency-triggered hyperhomocysteinemia has been shown to be significantly associated with cognitive impairments, neurodegenerative diseases, neuropsychiatric symptoms, and auditory dysfunction. 4
Vestibular-evoked myogenic potential (VEMP) is a noninvasive, rapid, easy, and cost-effective sound-evoked muscle reflex test that has become widespread for the electrophysiological assessment of vestibular functions in recent years. 5 Both cervical VEMP (cVEMP) and ocular VEMP (oVEMP) recording requires high intensity auditory stimuli such as clicks, bursts, or tapping. Cervical VEMPs are short-latency inhibitory reflexes of stimuli recorded from the electrodes placed over the contracted sternocleidomastoid (SCM) muscle. 6 Cervical VEMP typically evaluates the integrity of saccular and inferior-vestibular nerve functions. 7 Today, the diagnostic value of VEMP has expanded and been utilized in the diagnosis of various diseases and even in the assessment of central otolithic pathways. 8 Furthermore, VEMP abnormalities in patients with multiple sclerosis (MS), vestibular migraine, and some neurodegenerative disorders have been documented. 9 Therefore, we aimed to evaluate the VEMP responses in patients with vitamin B12 deficiency.
Materials and Methods
Sample
In this prospective study, 37 patients between 21 and 80 years diagnosed with vitamin B12 deficiency (<220 pg/mL) and had normal vestibular tests were compared with 31 audiologically healthy participants (control group) with normal B12 levels.
Patients with a history of external and middle ear diseases; with dizziness or vertigo symptoms, otologic surgery, or intratympanic interventions; conductive hearing loss; type B or type C tympanograms; extended myorelaxant treatment; neck surgery; neuropsychiatric, metabolic, or systemic disease, and patients with hearing aids or vitamin B12 levels > 220 pg/mL were excluded from the present study. Participants were enrolled in the study after written informed consent was obtained. Complete otorhinolaryngologic, pure-tone audiometry and immitancemetric examinations were performed on all participants.
Measures
Cervical VEMP test
Vestibular-evoked myogenic potentials were recorded while patients were in a seated position and rotated to face the contralateral side to provide sufficient tension of the SCM muscle. The short-tone bursts (500 Hz, 95 dB normal hearing level, and 5.1/s duration of repetition) with rarefied polarity were presented via ICS Medical Insert Earphones (ER 3A/5A Insert Earphone 300 ohms; ICS Medical, Illinois). Electromyographic activity was recorded ipsilaterally from surface electrodes placed over the upper third of the SCM muscle. During the test, the electrode impedance was less than 5 ohms.
The first early positive (p13) and following negative (n23) peaks (waves) of the VEMP responses and amplitudes between the waves (p13-n23, interpeak amplitude, millisecond) were analyzed. Additionally, the VEMP asymmetry ratio was calculated with the following formula:

where Ar is the amplitude on the right and Al is the amplitude on the left.
Laboratory measurements
The serum vitamin B12 analysis was performed via an immunodiagnostic system (Siemens, Advia Centaur XP, Germany) at a normality level of 220 pg/mL.
Statistical Analysis
All data were analyzed with SPSS (Statistical Package for the Social Sciences) software for Windows (version 21.0; IBM, Armonk, New York). Individual and aggregate data were summarized using descriptive statistics including mean, standard deviations, medians (min-max), frequency distributions, and percentages. Patients with absent VEMP responses were also included into all analyses. Normality of data distribution was verified by the Kolmogorov-Smirnov test. Comparison of the variables with normal distribution was made with a Student t test. For the variables that were not normally distributed, the Mann-Whitney and Kruskal-Wallis tests were conducted to compare the groups. Evaluation of categorical variables was performed by χ2 test. The presence of correlation was analyzed with Spearman ρ or Pearson tests. Values of P < .05 were considered to be statistically significant.
Results
Of the 68 patients included in this study, 21 (30.9%) were male, 47 (69.1%) female, and the mean age of total participants was 46.75 ± 14.88 (range: 20-79) years. Of the patient group (n = 37) with vitamin B12 deficiency, 9 (24.3%) were male and 28 (75.7%) female (female to male ratio was 3:1), with a total mean age of 49.00 ± 15.23 years. In addition, the mean age was significantly higher in male patients (57.78 ± 12.37) compared to female patients (46.18 ± 15.17; P = .030; Table 1).
Comparison of the Groups According to the Age and Gender.
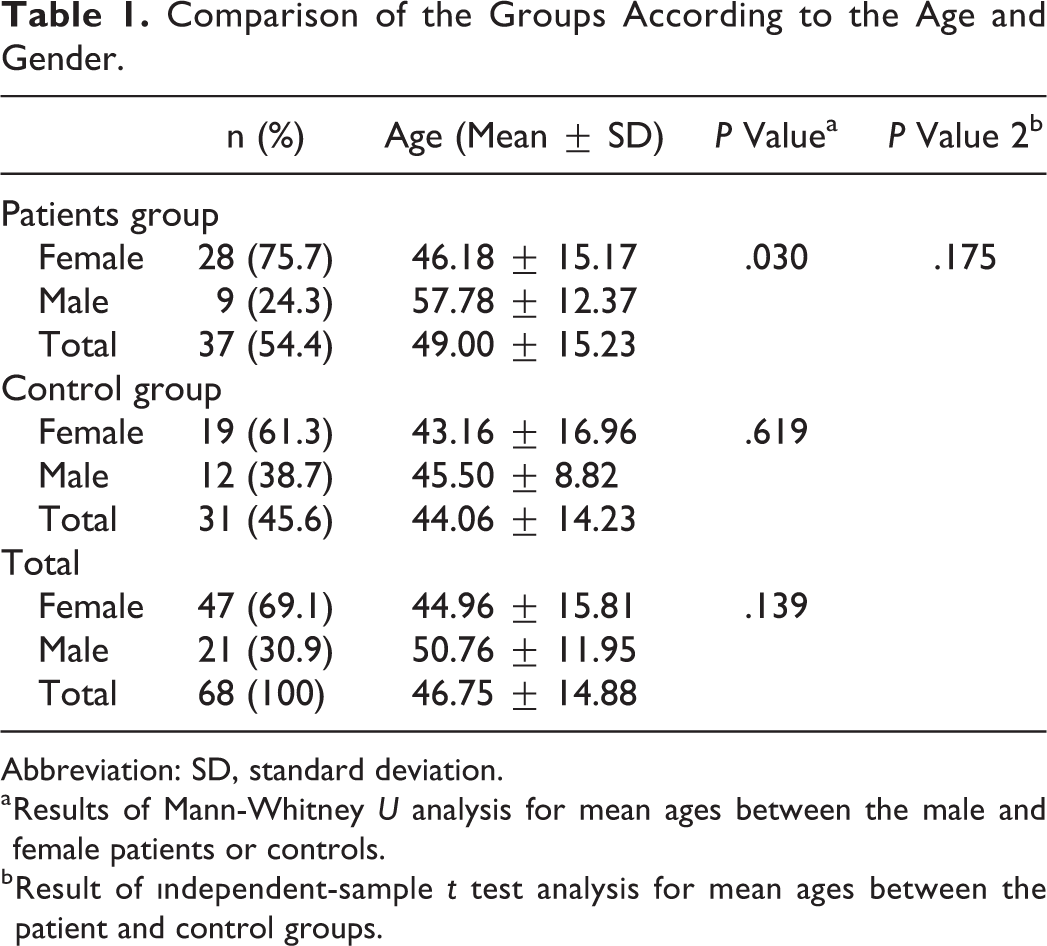
Abbreviation: SD, standard deviation.
a Results of Mann-Whitney U analysis for mean ages between the male and female patients or controls.
b Result of ındependent-sample t test analysis for mean ages between the patient and control groups.
In our study, VEMP recordings revealed 12 patients (7 bilaterally and 5 unilaterally) and 6 healthy individuals (2 bilaterally and 4 unilaterally) with absent VEMP responses. Thus, the rate of absent VEMP responses in the patient group was numerically higher than the control group (P = .064; Table 2). Additionally, there were no statistically significant differences detected according to the pure-tone audiometric results between patients and healthy controls.
VEMP Responses.
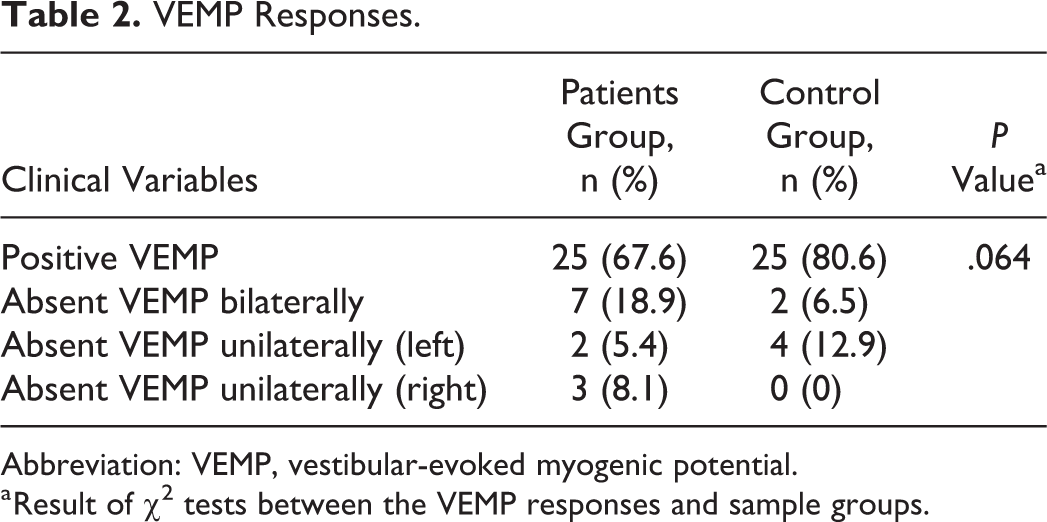
Abbreviation: VEMP, vestibular-evoked myogenic potential.
a Result of χ2 tests between the VEMP responses and sample groups.
In our study, the comparison of VEMP test findings between the patient group with a mean serum B12 level of 224.47 ± 20.48 pg/mL and the control group with a mean serum B12 level of 525.42 ± 110.92 pg/mL is presented in Table 3. The mean interpeak amplitude value in both the right (49.17 ± 45.95 µv) and left (53.05 ± 38.71 µv) ears measured in the patient group was statistically lower than the mean interpeak amplitude values measured in the right (68.46 ± 40.77 µv) and left (79.69 ± 43.52 µv) ears of the control group (P values = .024 and .007, respectively). Moreover, the mean amplitude asymmetry ratio was statistically higher in the patient group (29.00 ± 21.30) than the control group (18.58 ± 14.70; P = .050). There were no statistically significant differences detected according to the p13 or n23 latency responses measured in both the right and left ears between groups (P > .05). Furthermore, a positive, statistically significant correlation was detected between values of left P1–N1 interpeak amplitude and vitamin B12 levels (r = 0.287, P = .037; Table 4).
VEMP Findings Between Groups.
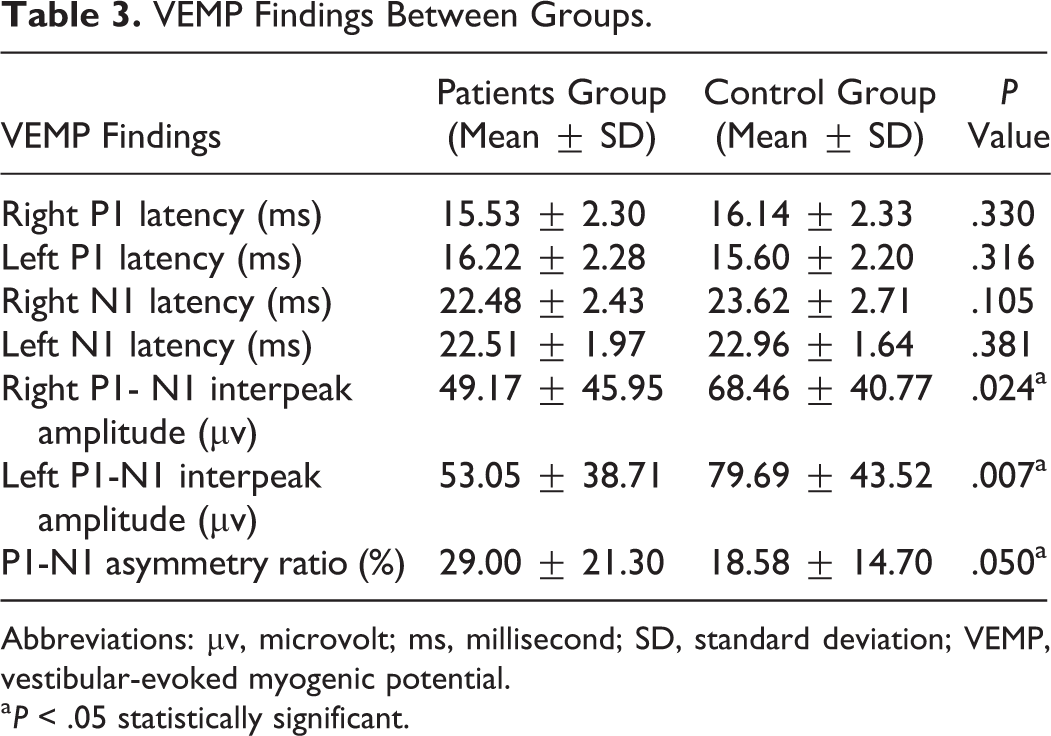
Abbreviations: µv, microvolt; ms, millisecond; SD, standard deviation; VEMP, vestibular-evoked myogenic potential.
a P < .05 statistically significant.
Correlation Analysis Between Vitamin B-12 Levels and VEMP Findings in Participants.
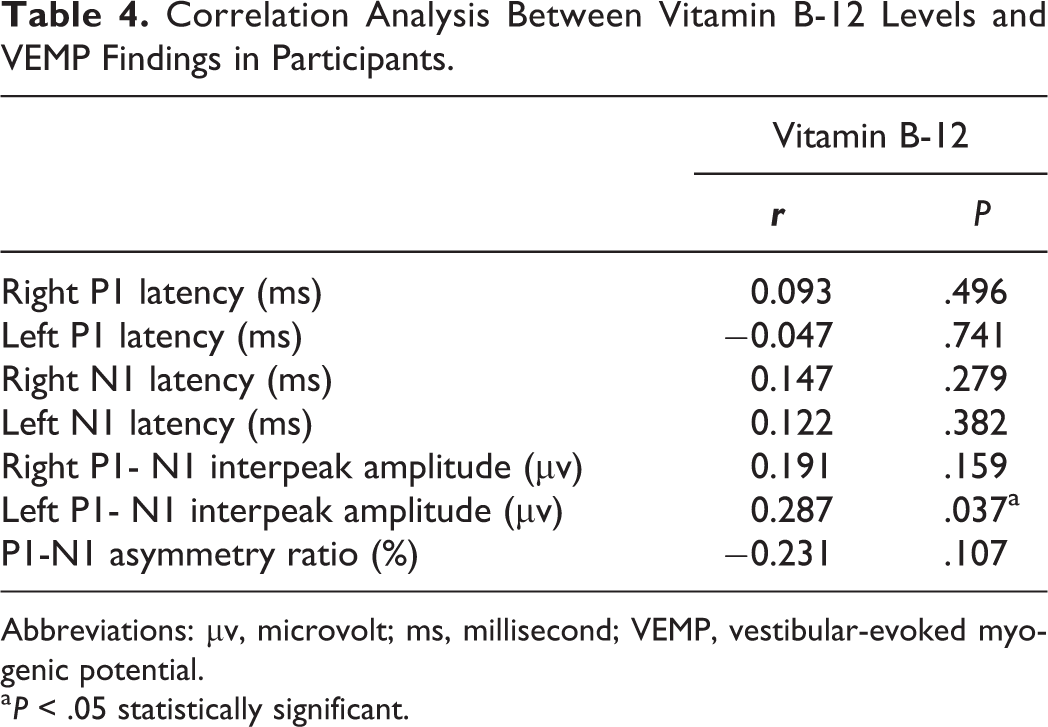
Abbreviations: µv, microvolt; ms, millisecond; VEMP, vestibular-evoked myogenic potential.
a P < .05 statistically significant.
Discussion
In recent years, nutritional status has become an increasingly popular research topic in the etiology of hearing impairment. 10 According to the National Health and Nutrition Examination Survey data, the prevalence of B12 deficiency is reported as 2.9%, 10.6%, or 25.7% based on B12 cutoff values of < 148, < 200, and < 256 pmol/L, respectively. In addition, advanced age (> 60 years) and female gender are frequently associated with increased prevalence. 2,11 Karabulut et al 12 documented a high B12 vitamin deficiency in 21.6% of 466 adult premarital women. In accordance with these data, the prevalence of B12 deficiency was 3.1 times higher in female patients, and male patients were significantly older in our study. In addition, there were no statistically significant differences found between the mean ages of patients and healthy controls.
Hyperhomocysteinemia due to low levels of vitamin B12 and folate have been linked to hearing impairment in numerous published studies. 3,13 In order to prevent possible bias caused by impaired B12 absorption in advanced age, Gocer et al 14 designed a sample group with middle-aged (40-60 years) patients. Researchers reported lower B12/folate status with higher homocysteine levels in patients (n = 78) with hearing impairment than in the healthy control group (n = 53). There are limited published studies evaluating micronutriological risk factors with the VEMP method. Only a few studies documented VEMP recordings in vitamin D deficiency with debated results. 15,16 Moreover, to our knowledge, there is no published study available that evaluated the vestibular or auditory functions via VEMP method in patients with B12 deficiency.
Nola et al 17 observed normalized cVEMP responses without any improvement of the caloric test in 20 patients diagnosed with acute vertigo caused by vestibular neuritis (VN). Thus, the researchers concluded that the cVEMP recording is an appropriate method for screening vestibular disorders as it easily monitors the improvement of otolithic functions and contributes to the diagnosis of VN-associated vestibulopathy. Similarly, Ochi and Ohashi 18 reported absent VEMP responses in a patient with acute-phase VN, and researchers also observed complete recovery of the VEMP responses after 15 months. Additionally, absent click-VEMP responses were documented between 12% and 39% of patients with VN. 19 Moreover, Egami et al 20 reported a sensitivity and specificity of 50% and 48.9%, respectively, with the VEMP procedure, and Waele et al 21 reported absent VEMPs in 54% of patients with Meniere’s disease. Furthermore, absent cVEMP responses were considered to be associated with saccular dysfunction, particularly in the advanced stages of Meniere’s disease; thus, researchers recommended cVEMP as a useful test to measure saccular function in Meniere’s disease. 22 However, absent VEMP responses are documented in bilateral vestibulopathy and vestibular schwannoma (up to 80%); the reliability of the VEMP method in the presence of a tumor is an uncertain and debated topic today. 19 Similarly, in our study, VEMP recordings revealed 12 patients (7 bilaterally and 5 unilaterally) and 6 healthy individuals (2 bilaterally and 4 unilaterally) with absent VEMP responses. Thus, absent VEMP responses occurred twice as often in the patient group than in the healthy control group. It was initially confirmed that there were no technical or physical causes leading to absent VEMPs during the testing procedure. Although the published data demonstrated that absent VEMPs involve a wide range of pathologies, in the present study, absent responses of VEMP were attributed to peripheral vestibular pathologies rather than to central pathologies. Additionally, in the control group, absent VEMPs in 5 participants aged > 45 years were interpreted as an advanced age effect; absent VEMPs in another control participant (aged 23 years) were attributed to possible asymptomatic saccular pathologies.
Eleftheriadou et al 23 compared 46 MS patients with vestibular symptoms to 40 healthy controls and noted p13-n13 abnormalities in 50% (n = 23) of patients via cVEMP recordings. Researchers concluded that demyelination of primary afferent or vestibulospinal tract axons caused absence or delay of p13-n23 latency in VEMP recordings. Moreover, lower amplitude recordings have been documented by VEMP in patients with vestibular migraine compared to the healthy controls. 24,25 Baier et al 26 compared cVEMP responses in 63 patients with vestibular migraine to 63 gender- and age-matched healthy controls and detected reduced VEMP amplitudes in 68% of patients without any pathology in latency responses. Researchers indicated possible abnormalities in saccular pathways. In our study, significantly reduced mean value of interpeak amplitude in both right and left ears without any abnormalities in latencies was demonstrated in the patient group. Moreover, the mean amplitude asymmetry ratio was statistically higher in the patient group than the control group. Furthermore, a positive, statistically significant correlation was detected between values of left p1-n1 interpeak amplitude and vitamin B12 levels. The asymmetry ratio is a more sensitive parameter, particularly in unilateral hypofunction evaluation. Therefore, our findings can be attributed to impaired function or ischemia of peripheral vestibular structures.
We conducted a prospective evaluation with a limited sample sized. In this respect, further research should be performed with larger study groups to contribute to the diagnosis and treatment of impaired vestibular functions with nutritional etiology.
In conclusion, to our knowledge, for the first time in the literature, an increased rate of absent VEMPs and decreased amplitudes with normal latencies was demonstrated in patients with vitamin B12 deficiency. These findings are interpreted as evidence of peripheral vestibular hypofunction.
Footnotes
Authors’ Note
Institutional Review Board protocol approval number: 2018/304. Institutional Review Board protocol approval number date: 05/07/2018.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.