
Abstract
Introduction
The B vitamins, namely, B1, B2, B3, B5, B6, B7, B9, and B12, also known as thiamine, riboflavin, niacin, pantothenic acid, pyridoxine, biotin, folate, and cobalamin respectively, are group of essential nutrients with diverse chemical properties that fulfill various functions in the human body. 1 Most of these vitamins are produced by plants, except for vitamin B12. The neurotropic vitamins B1, B6, and B12 each plays unique roles in the nervous system. Vitamin B12 (cobalamin) is a micronutrient that serves an important function in maintaining metabolic function of the body. It also has a role in DNA synthesis and maintaining blood level. 2 Myelination, which refers to synthesis of myelin sheath, is another important function of vitamin B12(2). Due to its involvement in numerous critical pathways, a deficiency in vitamin B12 poses a significant health issue.3,4
Insufficient intake or impaired absorption of vitamin B12 leads to vitamin B12 deficiency. 5 A vitamin B12 deficiency is commonly diagnosed based on the measurement of vitamin B12 in serum or plasma. A vitamin B12 deficiency is considered as having a concentration below 148 pmol/L (200 pg/mL) and marginal status defined as a concentration of 148 to 221 pmol/L. 6
The source of vitamin B12 is mainly from animal-based food products 7 and very few plant based foods, such as shiitake mushrooms, dried purple laver (nori), and tempe. 8 One of the studies shows that consuming meat, milk, and fish is associated with higher vitamin B12 levels, particularly in Western countries. 9 Different types of animal meats such as beef, veal, mutton, and lamb, which come from ruminant animals such as cattle and sheep, are rich sources of B12. Additionally, pork and poultry, which come from omnivorous animals such as pigs and chickens, also serve as good sources of vitamin B12.7,10 Vegans, who exclude all animal-derived foods from their diet, need to fulfil their vitamin B12 needs through fortified foods or supplement 3 diet, thus having a significant impact on the vitamin B12 levels
The process of making vitamin B12 from food usable by our cells is complicated and has several steps. First, vitamin B12 binds to different proteins as it moves through the intestine and blood. These proteins include haptocorrin, intrinsic factor, and transcobalamin II. 11 Finally, the vitamin B12, now part of the holotranscobalamin complex, is absorbed by the target cell after it binds to the transcobalamin receptor. 12
Apart from vitamin B12 deficiency, other nutritional deficiencies such as iron, folic acid, and vitamin D are also known to affect the auditory system.9,13,14 Vitamin D is crucial for maintaining calcium balance and is essential for transmitting electrical impulses between nerve fibers and hair cells. Few studies have reported that low levels of vitamin D can lead to sensorineural hearing loss (SNHL) and may also increase the risk of age-related hearing loss (ARHL).15,16 Iron deficiency can reduce oxygen supply to cells, potentially damaging them and impairing the brain's ability to process sound signals. This can lead to hearing loss and reduced auditory perception. 17 The formation of free radicals in the inner ear is a key factor in hearing loss, and vitamins A, C, and E, in synergy with magnesium, reduce changes in hearing thresholds more reliably than any single agent.18,19
Deficiency of vitamin B12 has been linked to impaired myelination of neurons in cochlear nerve, impaired cellular metabolism affecting nervous system and vascular system affecting hearing loss.20,21 Adequate vitamin B12 levels are essential for optimal functioning of the nervous and vascular systems. The deficiency in these levels and its impact on the auditory system has been explored in isolated studies, and a systematic review is warranted to consolidate these findings. The present systematic review explores the connection between vitamin B12 deficiency and hearing loss.
Method
The review was carried out based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 22 The review aimed to answer the research question “What is the relationship between vitamin B12 deficiency and hearing loss as evidenced in literature?” Thus, a systematic search was conducted to find the relevant articles examining the link.
The inclusion criteria for including studies in the review were as follows: studies exploring link between vitamin B12 deficiency and hearing loss and studies published in English language up to Match 2024. Animal and in vitro studies and studies on other micronutrients that did not discuss vitamin B12 deficiency and published in languages other than English were excluded. Case reports or case series and letter to editor were excluded.
The PubMed, Scopus, and Cochrane databases were searched using search terms and suitable Boolean operators “AND” and “OR.” A broad search was carried out using search terms “hearing loss” OR “hearing impairment” AND “Vitamin B12.” The search results were compiled using the Mendeley desktop reference manager, and duplicate studies were eliminated. Title and abstract screening were carried out independently by the first and second authors. The articles that met the inclusion criteria were included at this stage. Any discrepancies in inclusion were resolved through discussion among all the authors. The full-text articles corresponding to the shortlisted abstracts were retrieved. A predefined data-extraction template was used for this study. The data extracted from the final articles included details such as author details, year of publication, study design, population, inclusion and exclusion criteria, serum vitamin levels, audiological findings, and intervention used and outcomes. The quality of the included studies were assessed using the Mixed Methods Appraisal Tool (MMAT) version 2018. 23
Results
The Figure 1 illustrates the process followed based on the PRISMA statement.
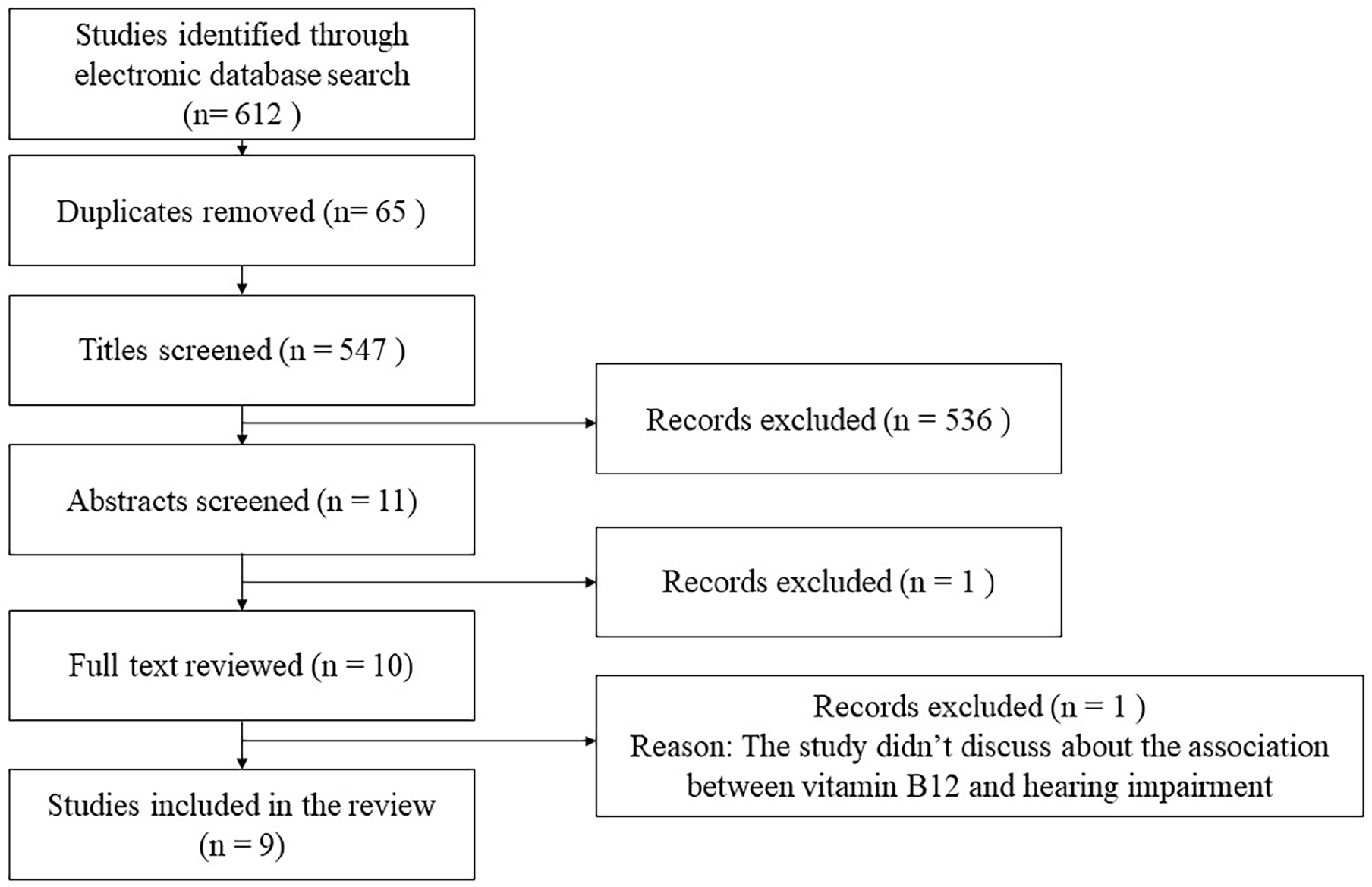
Prisma flowchart.
A total of 612 articles were identified across different databases of which 69 were duplicates. After duplicates removal, 547 studies were screened for the title. Eleven articles underwent abstracts screening. A total of 10 studies were included for full-length review of which 9 article were finally included in review for data-extraction.
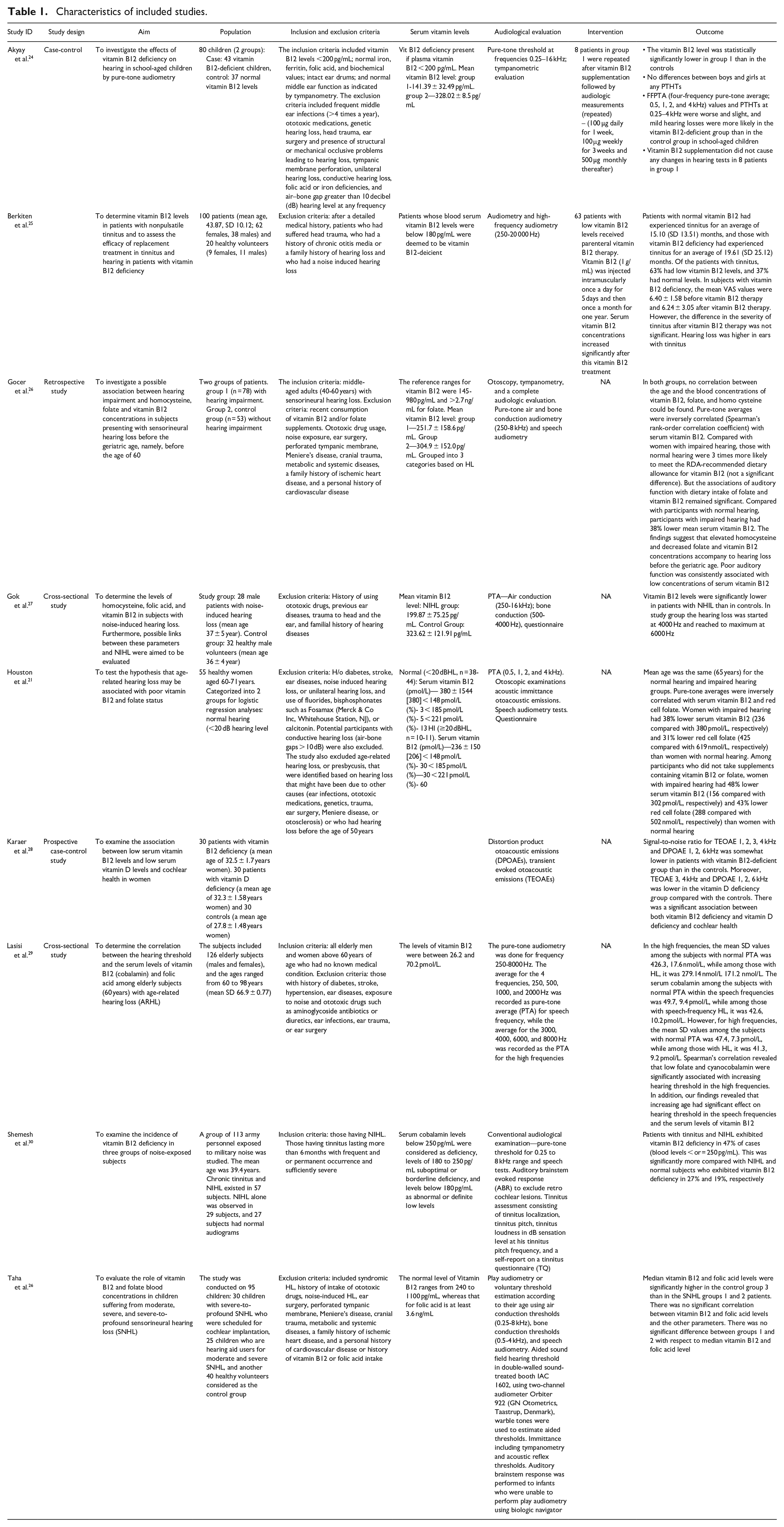
The characteristics of the included studies are discussed in Table 1.
Characteristics of included studies.
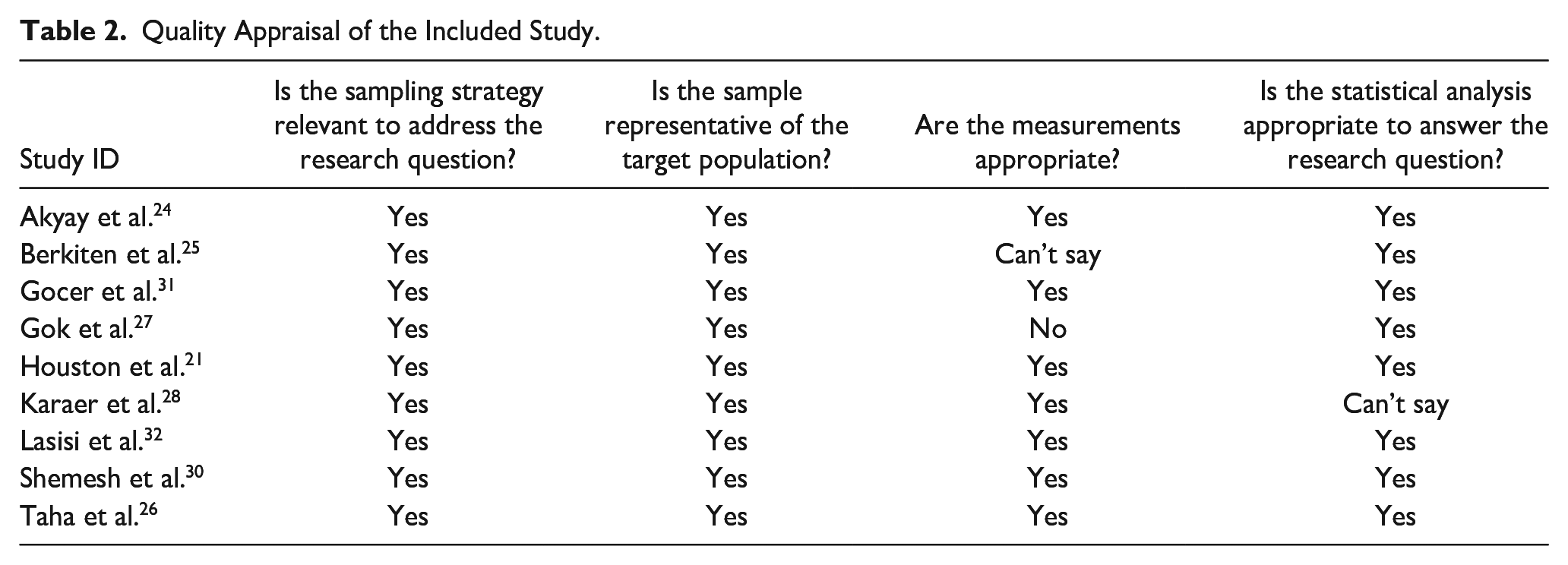
MMAT was used to appraise the quality of the included study, and the results are tabulated in Table 2.
Quality Appraisal of the Included Study.
Discussion
The systematic review examined the association between vitamin B12 levels and hearing loss across multiple studies. The review examined the relationship between vitamin B12 levels and hearing loss across diverse populations, considering factors such as noise-induced hearing loss (NIHL), age-related hearing decline, and elderly participants. Based on our findings several studies reported that individuals with lower vitamin B12 levels had a higher prevalence of hearing impairment than those with normal or elevated levels.24-26,29,31,32
Homocysteine, Folate, and B12 Deficiency: Links to Sensorineural Hearing Loss
Vitamin B12 and folic acid play a crucial role in homocysteine metabolism, and a deficiency in either of these vitamins leads to elevated homocysteine levels. 32 Gocer et al. 31 and Gok et al. 27 aimed to investigate the association between hearing impairment and the levels of homocysteine, folate, and vitamin B12 in individuals with SNHL under the age of 60, and to determine these levels in subjects with NIHL and evaluate their potential links to NIHL respectively. Gok et al. 27 aimed to assess the levels of homocysteine, folic acid, and vitamin B12 in individuals with NIHL and explore potential connections between these factors and NIHL. Results indicated that folate and vitamin B12 levels were notably reduced in patients with NIHL. Additionally, the hearing loss in the study group predominantly began at 4000 Hz and peaked at 6000 Hz. Gocer et al. 31 conducted a retrospective study investigating the potential association between SNHL before the age of 60 and levels of homocysteine, folate, and vitamin B12. They analyzed 2 groups: group 1, comprising 78 participants with hearing impairment, and group 2, a control group of 53 individuals without hearing impairment. The study included middle-aged adults (40-60 years) with SNHL and excluded those with recent vitamin B12 or folate supplement intake, ototoxic drug usage, noise exposure, ear surgery, and various medical conditions. The study found significant associations between auditory function and dietary intake of folate and vitamin B12, with participants with impaired hearing having lower mean serum vitamin B12 levels, suggesting a potential link between elevated homocysteine and decreased folate and vitamin B12 concentrations and hearing loss before old age. The findings underscored a consistent association between poor auditory function and low serum vitamin B12 concentrations.
Vitamin B12 Deficiency in Children and Hearing Loss
Hearing loss due to vitamin B12 deficiency manifests differently across the lifespan. In children, it can disrupt the development of the auditory system, leading to notable developmental issues if untreated, while in adults, particularly the elderly, it accelerates age-related hearing decline due to neurodegenerative effects.24,26 Akyay et al. 24 provided critical insights into the effect of vitamin B12 supplementation on hearing outcomes. This study reported that among 8 patients with severe B12 deficiency (levels less than 100 pg/mL) supplementation did not result in significant changes in their hearing test results. Additionally, they observed that mild hearing loss was more common among school-aged children with vitamin B12 deficiency than those in the control group. Another study by Taha et al. 26 assessed the impact of blood concentrations of vitamin B12 and folate in children experiencing varying degrees of SNHL, ranging from moderate to severe and severe to profound. The control group had significantly higher median levels of vitamin B12 than the groups with SNHL. However, there was no significant difference between the 2 groups with SNHL moderate to severe and severe to profound with respect to median vitamin B12 level.
Influence of Vitamin B12 Deficiency on Elderly Population and Hearing Loss
Seven studies address the connection between vitamin B12 deficiency and hearing loss in adults and older people. Two studies21,29 investigated the possible relationship between vitamin B12 levels and ARHL in older adults. Based on pure-tone air conduction threshold, Houston et al. 21 performed a comprehensive audiometric evaluation on 55 healthy women aged 60 to 71 years, classifying their hearing function into the normal and impaired groups. They discovered that compared to women with normal hearing those with hearing impairments had far lower serum vitamin B12 levels. Serum vitamin B12 levels were found to be 38% lower in women with hearing impairments and 48% lower in those who did not take vitamin B12 supplements. It is interesting to note that there was a dose-response pattern in the link between serum vitamin B12 levels and auditory function at various hearing levels. This investigation was expanded to a more extensive and diversified group of 126 senior citizens, aged 60 to 98, who were both male and female. They evaluated hearing thresholds at different frequencies and compared the results to serum levels of folate and vitamin B12. They reported that there was a substantial correlation between growing older and declining vitamin B12 levels and that higher hearing thresholds in the high frequencies were significantly correlated with lower vitamin B12 levels. The results of these investigations emphasize the significance of keeping elderly people’s vitamin B12 levels at optimal levels as a potentially modifiable risk factor for ARHL. Since vitamin B12 deficiency can have a substantial negative influence on quality of life, early detection of and treatment for the deficiency could be a preventive intervention. 21 Lasisi et al. 29 conducted a cross-sectional study aiming to determine the relationship between hearing thresholds and serum levels of vitamin B12 and folic acid among elderly individuals (aged 60 years and above) with ARHL. The study included 126 elderly subjects, both males and females, with an age range of 60 to 98 years. The study found that lower serum levels of folate and vitamin B12 were significantly associated with increased hearing thresholds in high frequencies. Additionally, advancing age was found to have a significant impact on hearing thresholds in speech frequencies and serum levels of vitamin B12. However, the correlation between vitamin B12 and ARHL does not appear to be significant after adjusting for age.
Interaction of Noise Induced Hearing Loss and Vitamin B12 Deficiency
Two investigations found a link between vitamin B12 deficiency and noise exposure. In one study, Gok et al. 27 examined vitamin B12 levels in those who had NIHL. The research group’s hearing loss peaked at 6000 Hz, having begun at 4000 Hz. Patients with NHIL have considerably reduced mean levels of vitamin B12. The control group in this study consisted exclusively of men, influencing the generalizability of the findings across genders. Shemesh et al. 30 investigated the relationship between vitamin B12 deficiency and chronic tinnitus, which is often associated with hearing loss. They examined the prevalence of vitamin B12 deficiency in 3 groups of noise-exposed people: individuals with NIHL only, individuals with chronic tinnitus and NHIL, and subjects with normal hearing. One hundred thirteen military members who were subjected to noise were among the subjects. Ninety percent of the participants in the audiological testing and questionnaire used to estimate tinnitus stated having tinnitus pitch in the 4 to 8 kHz range. Supplements of vitamin B12 were given to each subject and kept up until levels were steady. While there was some improvement, the 3 symptoms of tinnitus, loudness, disruption in noisy surroundings, and general feeling showed significant improvement. The findings showed that vitamin B12 deficiency was much more common (47%) in patients with tinnitus and NIHL.
Vitamin B12 Deficiency and Tinnitus
Two of the studies also addressed tinnitus in those who are vitamin B12 deficient. In addition to reporting the vitamin B12 levels in individuals with nonpulsatile tinnitus, Berkiten et al. 25 also investigated the outcomes of vitamin B12 therapy. The study group and the control group had tinnitus for slightly different lengths of time. Thirty-seven percent of the tinnitus patients had normal vitamin B12 levels, while 63% had low level pure-tone audiometry revealed that ears experiencing tinnitus exhibited higher levels of hearing loss than those without tinnitus. An observational study by Shemesh et al. 30 found that supplementation with vitamin B12 led to an improvement in tinnitus symptoms for some of the patients, suggesting a potential therapeutic role for B12 in managing tinnitus associated with deficiency.
Limitations and Future Recommendations
Only studies in peer-reviewed English language articles were included, and grey literature and articles published in other languages were not considered. Differing reference ranges for vitamin B12 levels across studies and inconsistent categorization of participants based on hearing loss severity make the comparison of findings difficult. Additionally, understanding the relationship between auditory pathways and vitamin B12 deficiency is complex, considering factors such as the duration of deficiency and its impact on hearing sensitivity.
The present review included studies conducted in humans only, further studies and reviews can explore the relation between vitamin B12 deficiency based on laboratory-based or animal studies. There is also a lack of longitudinal data among individuals with vitamin B12 deficiency and the benefits on the auditory system (if any) associated with food and medical supplements to overcome the deficiency.
Conclusion
The current study contributes to the growing body of evidence suggesting a potential role for vitamin B12 in maintaining auditory health. Findings demonstrate that vitamin B12 deficiencies cause hearing impairment, particularly in cases of ARHL, NIHL, and SNHL. DPOAE responses in vitamin B12-deficient individuals were decreased, suggesting cochlear dysfunction. While some studies found that taking B12 supplements led to minor improvements in the severity of tinnitus and hearing thresholds, these results were often not statistically significant, suggesting that the therapeutic value of B12 is still unknown and needs more research. These results emphasize the need for additional study to completely comprehend the connection between vitamin B12 levels and hearing health, as well as the possible advantages of focused therapies for controlling and preventing hearing loss.
Footnotes
Contributors
KK, DRG, and RR proposed the search strategy, and SA and JR independently searched the database and extracted relevant data from the included literature. DRG arbitrate questions or disagreements arising from data retrieval and analysis. The final version of the manuscript has been reviewed by all authors and approved for publication.
CRediT Authorship Contribution Statement
Joyline Rodrigues and Shubhangi Anand: Conceptualization, investigation, methodology, project administration, and writing—original draft. Dhanshree R. Gunjawate: Supervision, validation, writing, and review and editing. Kaushlendra Kumar: Supervision, validation, and review and editing. Rohit Ravi: Conceptualization, methodology, data curation, and review and editing, and supervision.
Consent for Publication
All authors consent to the publication of this work.
Data Availability
The present study is a secondary data analysis, and all the information is embedded in the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.