
Abstract
This is a case of a pediatric male who presented with a postauricular mass and pain. Computed tomography and magnetic resonance imaging suggested a diagnosis of Langerhans cell histiocytosis. Characteristic imaging findings and initial workup for Langerhans cell histiocytosis are described.
Keywords
An 11-year-old male presented from an outside facility to the emergency department with complaints of left postauricular swelling and pain for 6 weeks. His father noted that this was coincident with an upper respiratory illness. The patient completed a course of antibiotics with improvement in the upper respiratory illness; however, the postauricular swelling persisted. Due to the persistent swelling, his pediatrician obtained a computed tomography (CT) scan, which showed a lytic lesion involving both the inner and outer tables of the left skull with local mass effect on the transverse and sigmoid sinus (Figure 1), and the patient was transferred to the emergency department for further evaluation.
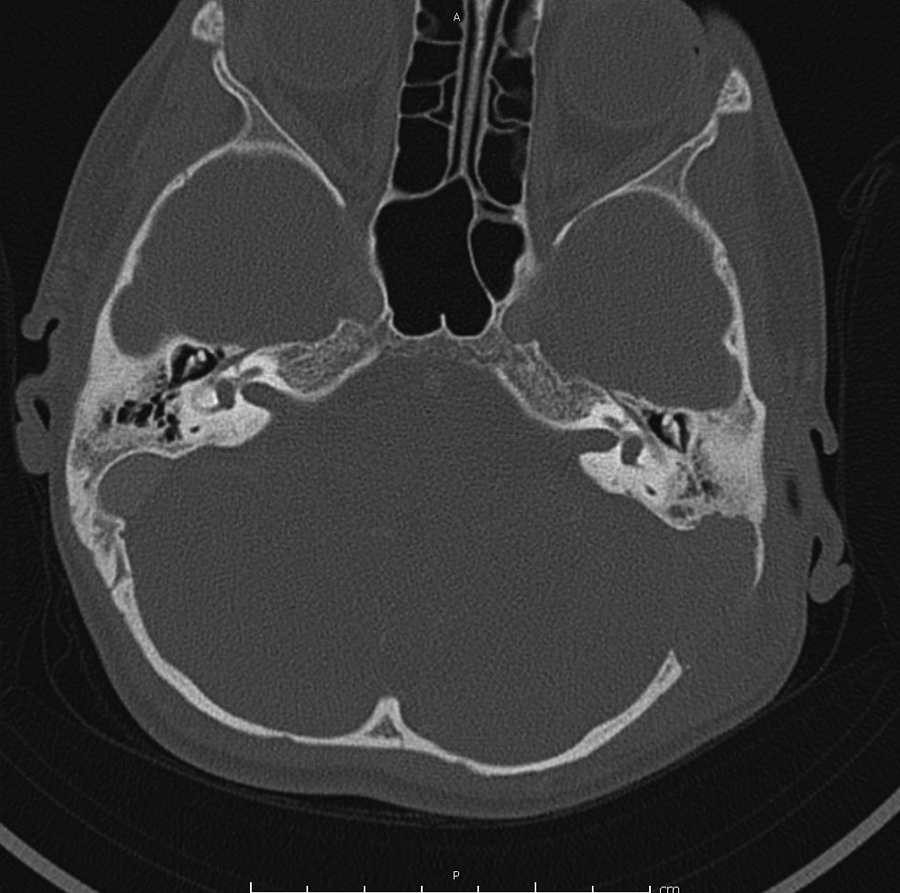
Axial computed tomography scan demonstrating a mass of the left temporal bone with loss of the inner and outer tables.
Upon presentation, the patient appeared well. The patient reported hearing loss and postauricular pain and denied otorrhea or tinnitus. He had a history of tympanostomy tubes placed 3 years prior and had no other history of other otologic surgeries. Physical examination revealed a palpable spongy mass in the left postauricular area, which was tender to palpation. The left tympanic membrane was intact and no middle ear effusion was identified. Differential diagnosis at the time included Langerhans cell histiocytosis (LCH), primary neoplasm (rhabdomyosarcoma), cholesteatoma, glomus jugulare, and otomastoiditis.
The patient was admitted to the hospital and received magnetic resonance imaging (MRI) for further characterization of the mass, which confirmed the presence of an expansile mass centered just posterior to the left mastoid with effacement of the sigmoid sinus (Figures 2 and 3) suggestive of LCH. A bone scan showed no additional significant osseous lesions. Biopsy specimens were obtained, which demonstrated infiltrates of atypical histiocytes, and immunohistochemical analysis showed coexpression of CD1a and S100 antigens confirming the diagnosis of unifocal LCH. The patient underwent placement of an implanted port and was referred to the local cancer center for treatment.
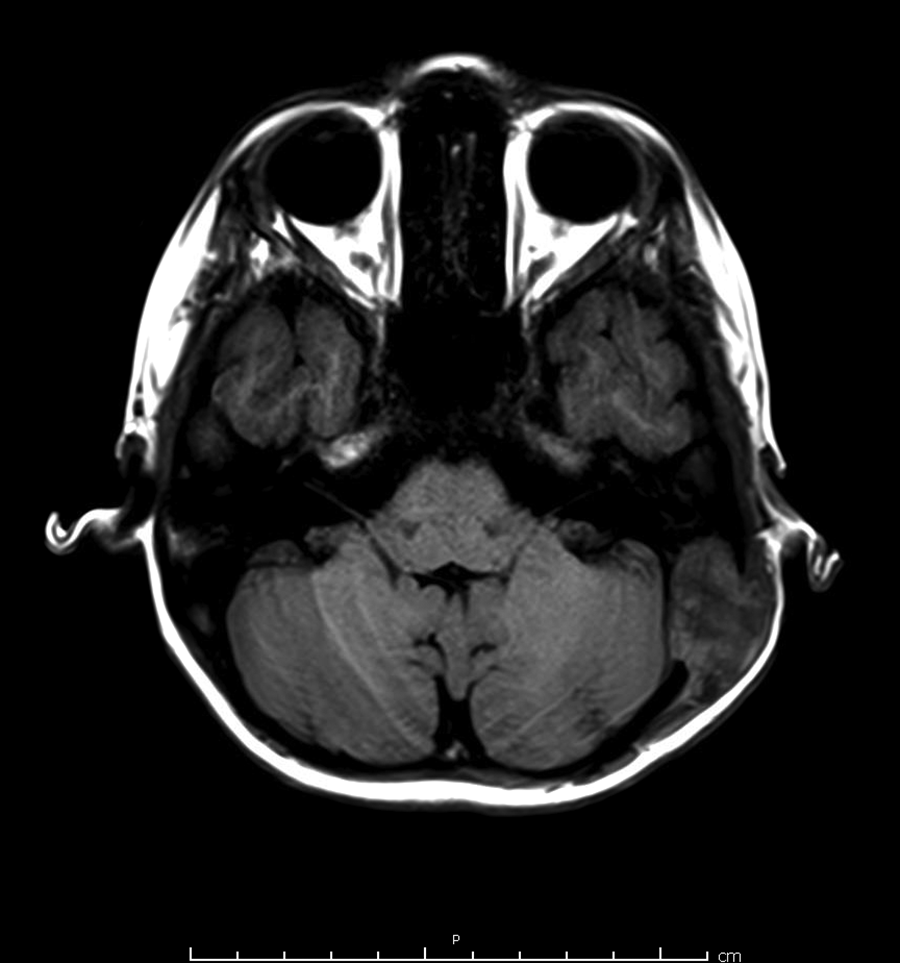
T1-weighted magnetic resonance imaging demonstrating a heterogenous hypointense mass of the left temporal bone.
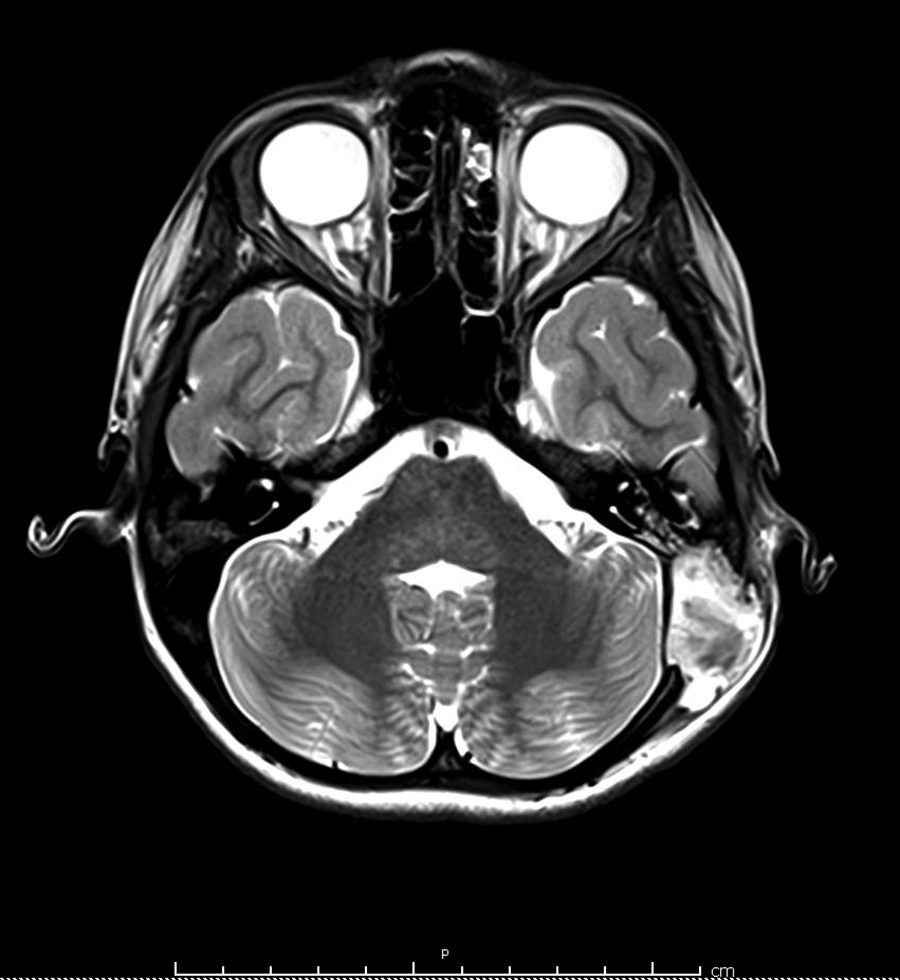
T2-weighted magnetic resonance imaging of the left temporal bone mass demonstrating a hyperintense mass of the temporal bone.
Langerhans cell histiocytosis is a rare disorder, with an estimated incidence of 8.9 cases per million children younger than 15 years. 1 The term Langerhans cell histiocytosis encompasses 3 classic syndromes: eosinophilic granuloma, Hand-Schuller-Christian disease, and Letterer-Siwe disease. Eosinophilic granuloma is the most common form of LCH and manifests predominantly in the pediatric age-group, typically between 5 and 15 years. 2 It occurs most commonly as a unifocal bone lesion, resulting from the proliferation and accumulation of histiocytes and eosinophils. 2 This abnormal collection of Langerhans cells usually causes localized pain and adjacent soft tissue swelling or mass.
Osseous involvement is the most common presentation of LCH, typically presenting in the skull, pelvis, spine, mandible, ribs, and tubular bones. 3 The skull is the most commonly involved site. These lesions typically develop in the diploic space and appear as single or multiple punched-out lytic lesions with well-defined borders on radiographic imaging. The destructive nature of these osteolytic lesions and the uneven involvement of both the inner and outer tables of the skull may result in the classic beveled or scalloped radiographic description. 2 “Button sequestrum” may be present, which is opacification of bone surrounded by a well-defined lucent area. 3 The most common sites of skull involvement are the petrous ridge and mastoid of the temporal bone. 3,4 Otologic manifestations include otorrhea resistant to medical treatment, preauricular mass, aural polyps, mastoid swelling, and/or hearing loss. 4,5
Computed tomography imaging of the skull classically reveals aggressive lytic osseous lesions with extensive destruction of bone, but without surrounding periosteal reaction or reactive sclerosis. 3,5 These radiologic findings are typically out of proportion to the clinical findings. Despite the extensive erosion present, involvement of the ossicles or inner ear is rare in eosinophilic granuloma. Ultimately, the radiologic appearance of the osseous lesions depends on the site of involvement and the phase of disease. 6
On MRI, these soft tissue masses commonly show a hyperintense signal on T2-weighted imaging and a hypo- or isointense signal on T1-weighted imaging. 2,4 There may be demonstration of surrounding soft tissue edema or inflammation around the lytic lesion. In cases of LCH involving the skull, MRI is helpful in demonstrating the extension of the lesion and any intracranial involvement for surgical planning if pursued.
The distinction between unifocal and multisystem LCH is important for prognosis and treatment; therefore, a skeletal survey is recommended in the workup in patients suspected to have LCH. Plain radiographs are best to assess the involvement of the skeleton. Definitive diagnosis is established by biopsy and immunohistochemical analysis. In conclusion, the diagnosis of temporal bone LCH should be considered in a pediatric patient with findings of predominant mastoid involvement, ill-defined bony destruction without periosteal reaction, and a soft tissue lesion on CT and/or MRI, and confirmed with histopathologic examination.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.