
Abstract
Objective:
Recently, many commercial one-piece alloplastic materials are used in nasal dorsum augmentation and increased nasal tip projection, but there is no study about their effects with regard to size on nasal shape so far. The aim of this study is to evaluate the impact of oversized one-piece alloplastic implant on nasal tip projection.
Methods:
We categorized nasal tip drooping as primary (group 1: no rhinoplasty or trauma history) and secondary (group 2: previous history of augmentation rhinoplasty with one-piece alloplastic materials), and retrospectively compared the characteristics of primary and secondary nasal tip drooping on the basis of pre- and postoperative rhinological parameters (nasolabial angle [NLA], rotation angle, nasofrontal angle [NFA], and Goode ratio).
Results:
A total of 50 patients were enrolled and completely reviewed. The mean age was 27.46 years (ranging from 19 to 49 years) in group 1 and 31.33 years (ranging from 20 to 47 years) in group 2. The postoperative NLA and rotation angle were not statistically different between 2 groups, but the postoperative NFA and postoperative Goode ratio were statistically different between 2 groups by independent t test. When we further performed univariate and multivariate analysis, the postoperative Goode ratio was the only factor that was significantly different between the 2 groups.
Conclusion:
Insertion of one-piece alloplastic implants from nasal tip glabella to dome of nasal tip may induce secondary nasal tip drooping. The degree of recovery of nasal tip projection is different between 2 groups and may be obtained by a more delicate surgical techniques.
Introduction
Nasal tip drooping (decreased nasal tip projection, underprojected nasal tip) is one of the most importantly displeasing disharmonies to correct. 1 Nasal tip drooping occurs when nasal tip is more caudal than deemed ideal. Nasal tip drooping causes the nose to appear longer and imparts an aged facial appearance. 2 The causes of nasal tip drooping can be divided into 2 categories: intrinsic factors, such as long and vertically oriented lateral crura, with/without weak medial crura, and extrinsic factors such as excessive caudal anterior septum, with/without heavy nasal skin that pushes alar cartilages inferiorly. 1 Also, a poorly performed rhinoplasty may cause nasal tip drooping called as secondary nasal tip drooping. 3 Any surgical procedure that significantly weakens nasal tip supporting mechanisms has the potential to shift the normal nasal tip to a drooping position. Especially, since Koreans have attenuated lower lateral cartilages (LLCs), the strength to accentuate and support nasal tip projection is not enough. 4 In addition, when oversized alloplastic implants that are still widely used are inserted as a single piece into the dome area of nasal tip, the pressure exerted by the alloplastic implant can push the tip posteriorly and inferiorly (Figure 1). Therefore, an alloplastic implant may be another extrinsic factor that causes secondary nasal tip drooping.
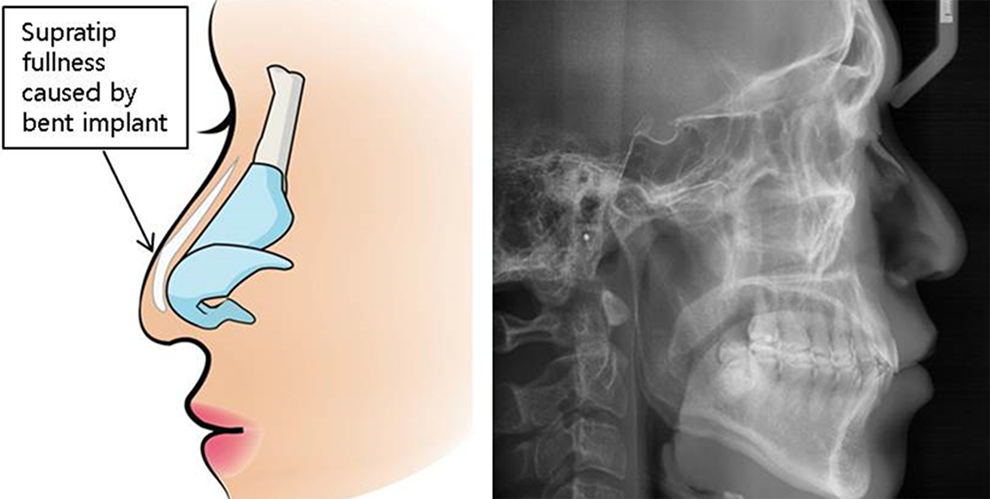
Secondary nasal tip drooping was caused by an oversized one-piece alloplastic implant in the dome area of nasal tip. The pressure exerted by the alloplastic implant can push and shift the nasal tip posteriorly and inferiorly.
The aim of this study is to evaluate the impact of oversized one-piece alloplastic implant on nasal tip projection on the basis of the clinical characteristics of patients with secondary nasal tip drooping caused by a one-piece oversized alloplastic implant compared with primary nasal tip drooping.
Patients and Methods
Patients
Patients who underwent rhinoplasty at Unique Aesthetic Clinic to correct nasal tip drooping were evaluated. A total of 50 patients were enrolled from July 2013 to June 2014 and were divided into 2 groups: those who underwent rhinoplasty for correction of primary nasal tip drooping and those who underwent revision rhinoplasty for correction of secondary nasal tip drooping caused by an oversized silicone alloplastic implant. All patients in the latter group complained of nasal tip drooping that arose after previous rhinoplasty.
Anthropometric Measurements
Standard facial photographs, including the frontal, lateral, and basal views, were taken preoperatively and at 6 months after surgery. The standard reference points for structural characteristics were all marked using the standard facial photographs. 5 We measured the nasolabial angle (NLA) and the rotation angle to evaluate nasal tip rotation following a previous report. 6 The NLA was measured at the intercept of the line from the columellar point to the subnasale with the line from the subnasale to the labrale superioris. The rotation angle was measured at the intercept of the line from the tip to the columellar point with a line tangential to the columella. Also, we measured the nasofrontal angle (NFA) and the Goode ratio to evaluate nasal tip projection. The NFA was measured at the intercept of the line from the glabella to the pogonion with the line from the nasion to the nasal tip. The Goode ratio was calculated by dividing the distance between the alar point and the tip by the distance between the nasion and the tip. Data were analyzed with Graph Pad Prism 5 (GraphPad Software Inc, San Diego, California).
Surgical techniques for correction of nasal tip drooping
Group 1: Correction of primary nasal tip drooping
Rhinoplasty was performed via an external approach (transcolumellar and bilateral marginal incisions). After exposure of the caudal septum, bilateral septal mucoperichondrial flaps were raised. As a structural grafting material, additional autologous cartilage was harvested from the nasal septum. A 1-cm-wide L-strut was maintained along the dorsal and caudal septum to preserve the nasal tip and dorsal profile support. The surgical exposure provided by an external approach allowed direct assessment of the long and vertically oriented lateral crura of LLC. Conservative cephalic resection of lateral crura of LLC was performed to increase nasal tip rotation. An approximately 7-mm-width intact lateral crura of LLC was left to prevent alar collapse. The columellar strut was inserted between the bilateral medial crura of LLC and sutured in a classical manner to fix the strut (Figure 2).
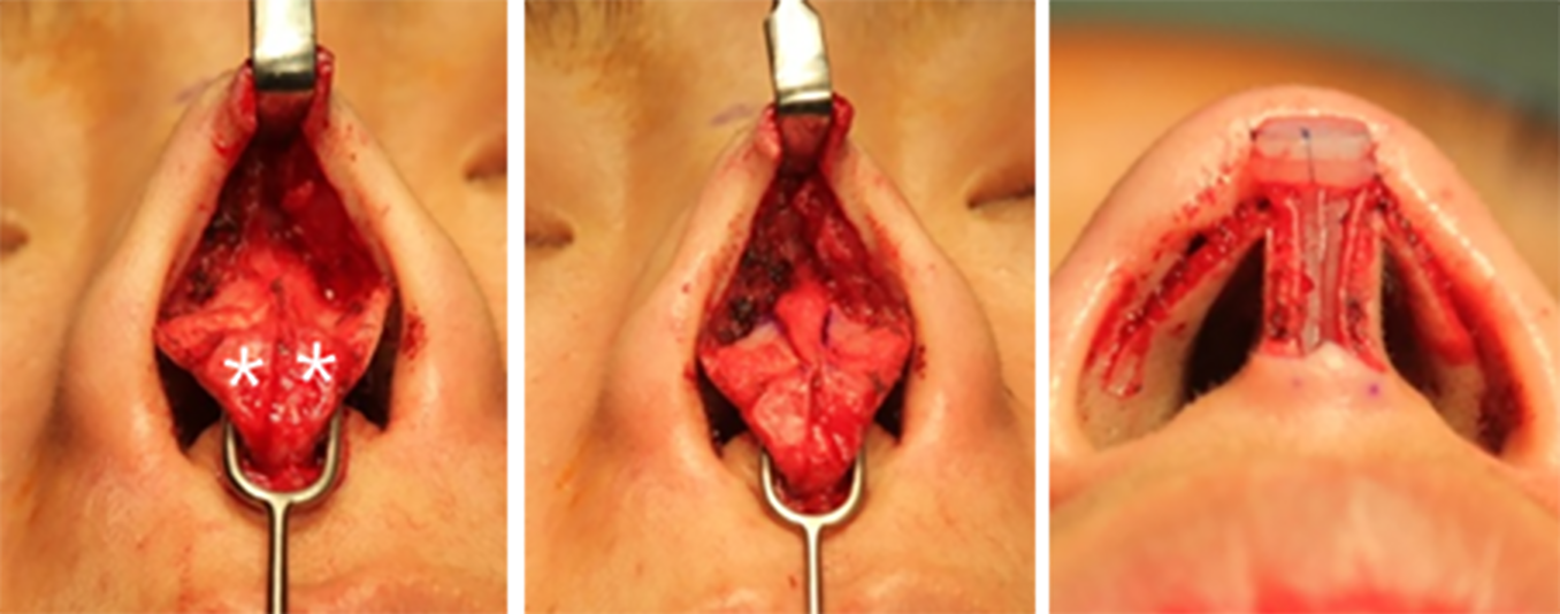
Operative technique of primary nasal tip drooping. The long and vertically rotated lateral crura was noted (asterisk). Conservative cephalic resection of lower lateral cartilage (LLC) was performed to increase nasal tip rotation. The columellar strut was inserted between 2 medial crura of LLC, and onlay grafts were placed and sutured on the dome.
Group 2: Correction of secondary nasal tip drooping caused by oversized one-piece alloplastic implant
Rhinoplasty was performed via an external approach (bilateral marginal incisions and transcolumellar incision: inverted V incision or using the previous operation scar). After exposure of the caudal septum, bilateral septal mucoperichondrial flaps were raised. As a structural grafting material, additional autologous cartilage was harvested from the remained nasal septum. A 1-cm-wide L-strut was maintained along the dorsal and caudal septum to preserve the nasal tip and dorsal profile support. The exposure provided by this approach allowed the direct assessment of the oversized alloplastic implant and LLC in their distorted position. The previously used alloplastic implant was removed. Lower lateral cartilages in all patients were buckled and twisted by the pressure caused by the alloplastic implant. After LLCs were released from the surrounding scar tissue, collapsed LLCs were realigned to achieve the normal structure. The columellar strut was inserted between the bilateral medial crura of LLC and sutured in a classical manner to fix the strut. The columellar strut helped to stabilize the weak medial crura and reinforce buckled medial crura. The exact size of the new pocket for proper alloplastic materials was created in the subperiosteal plane, and onlay grafts were placed on the dome and sutured (Figure 3).
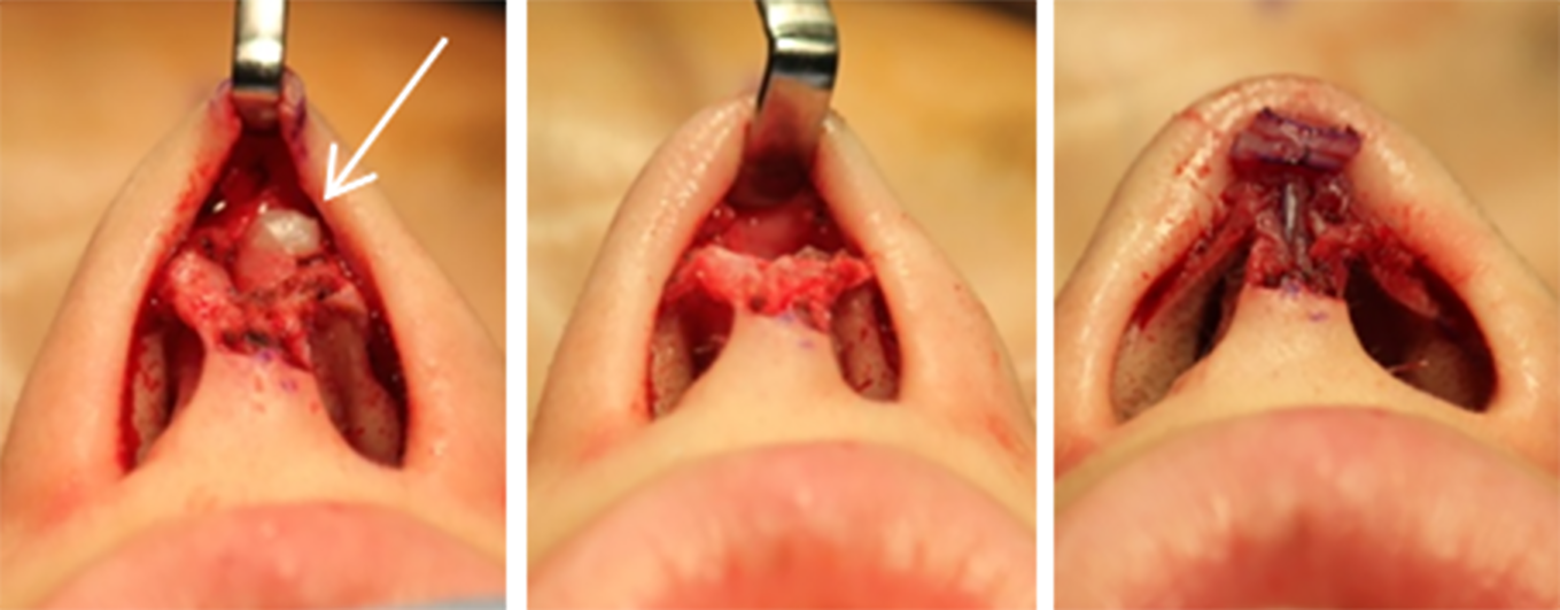
Operative technique of secondary nasal tip drooping. Buckled and twisted lower lateral cartilages (LLCs) were seen after removal of the alloplastic implant (arrow). The columellar strut was inserted between 2 medial crura of LLC, and onlay grafts were placed and sutured on the dome.
Results
The Comparison of Anthropometric Measurements Between Primary Nasal Tip Drooping and Secondary Nasal Tip Drooping
In group 1, 26 patients comprised, 18 women and 8 men. The ages of the patients ranged from 19 to 49 years, with a mean age of 27.46 (7.05) years. In group 2, the 24 patients comprised 22 women and 2 men. The ages of the patients ranged from 20 to 47 years, with a mean age of 31.33 (8.84) years. We compared the anthropometric measurements using rhinological parameters such as NLA, rotation angle, NFA, and Goode ratio between the 2 groups. The postoperative NFA and postoperative Goode ratio were statistically different between 2 groups by independent t test (Table 1). When we further performed univariate and multivariate analysis, the postoperative Goode ratio was the only factor that was significantly different between the 2 groups (Table 2).
Patients Characteristics.a
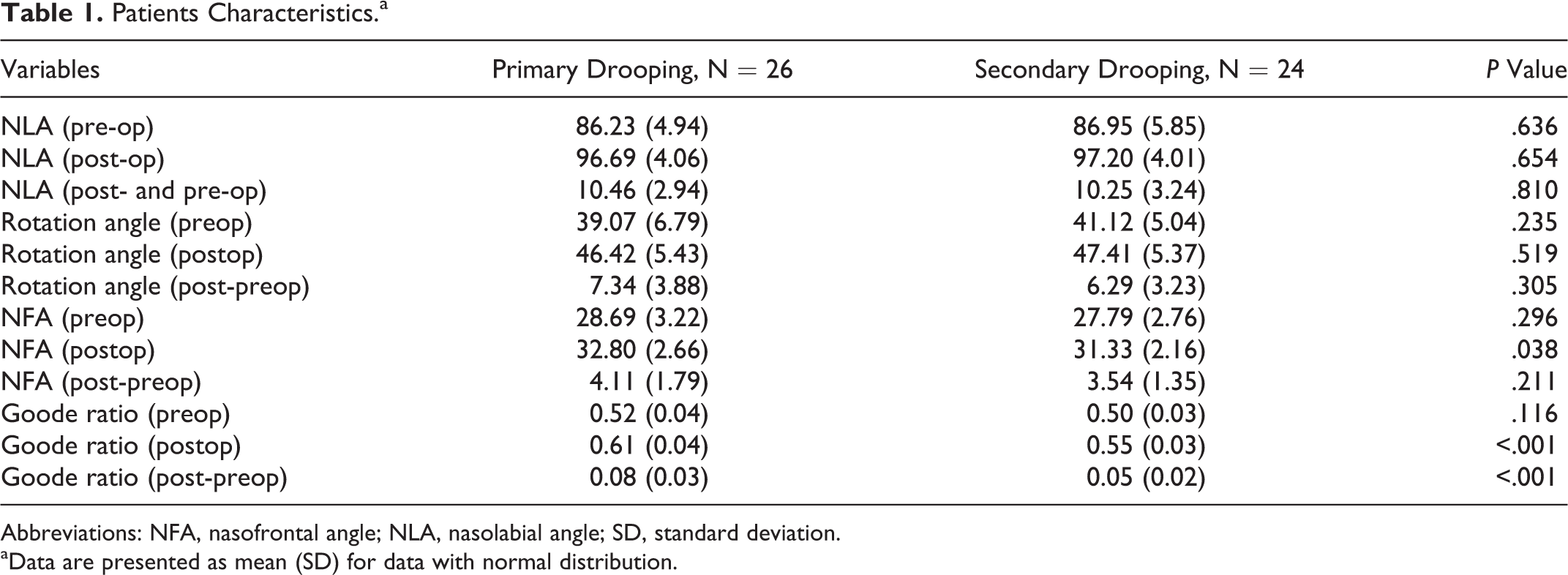
Abbreviations: NFA, nasofrontal angle; NLA, nasolabial angle; SD, standard deviation.
aData are presented as mean (SD) for data with normal distribution.
Univariate and Multivariate Regression Analysis.a
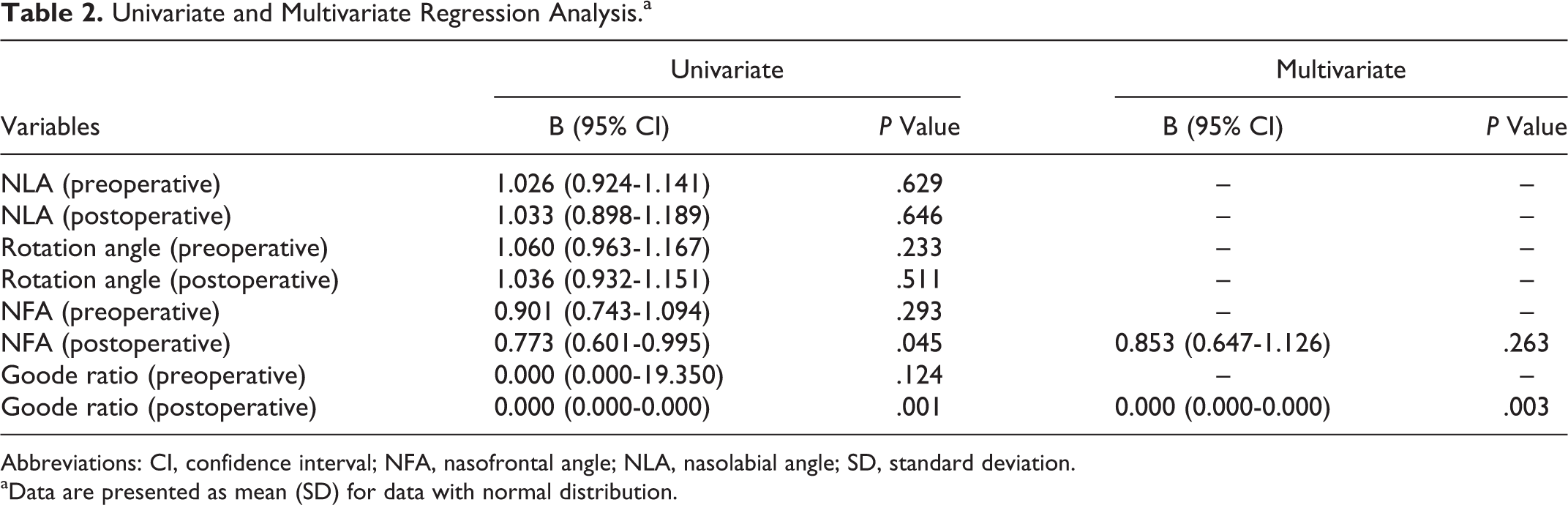
Abbreviations: CI, confidence interval; NFA, nasofrontal angle; NLA, nasolabial angle; SD, standard deviation.
aData are presented as mean (SD) for data with normal distribution.
Discussion
The typical Asian nose is characterized by a broad, flat dorsum with shallow, depressed origin at the nasion, deficient tip projection, thick lobular skin, a wide lobule, abundant subcutaneous fibro-fatty tissue, and a small osteocartilaginous framework. 7,8 So, during rhinoplasty, augmentation is more required rather than reduction. In general, Asian surgeons prefer readily available alloplastic implants such as silicone, Gore-Tex, Medpor, and hydroxyapatite, which are not associated with donor-site morbidity, offer ease of sculpting, and have smooth contours. 4,9,10
In our study, we reviewed 26 patients with primary nasal tip drooping and 24 patients with secondary nasal tip drooping caused by a previous rhinoplasty with oversized silicone one-piece implant. We compared the preoperative structural characteristics of patients with primary and secondary nasal tip drooping. Nasal tip rotation as evidenced by the NLA and rotation angle, and nasal tip projection as evidenced by the NFA and Goode ratio were evaluated. The differences in preoperative nasal tip rotation and nasal tip projection were not statistically significant. However, although the preoperative Goode ratio was not different between primary and secondary nasal tip drooping, we found that surgical outcomes were different between the 2 groups, which means that the degree of recovery of the nasal tip projection was different between primary and secondary nasal tip drooping. Although the mean values of both groups were in the normal range, the postoperative Goode ratio was higher in group 1. In other words, tip projection by correction surgery is more difficult to achieve in secondary rhinoplasty than in primary rhinoplasty. We think this result was caused by the destruction of the normal supporting structure of nasal tip projection and the scar formation in the surrounding tissue. So, additional surgical maneuvers should be performed to acquire enough nasal tip projection in patients with secondary tip nasal drooping.
Based on the above results, we suggest 2 important points about secondary nasal tip drooping. First, we found the placement of an oversized one-piece alloplastic implant from the glabella to the nasal tip could result in secondary nasal tip drooping. The increased tension along with the downward force of gravity by a one-piece alloplastic implant can push the dome of alar cartilages posteriorly and inferiorly. This means that one-piece alloplastic implants can function as another extrinsic factor and result in secondary nasal tip drooping. Our finding suggests that secondary nasal tip drooping should be considered another complication associated with alloplastic augmentation, especially in the case of augmented rhinoplasty with oversized one-piece implants.
Second, since anatomy of nasal tip and facial features vary widely between patients, there is no single surgical technique that can be routinely applied in all patients to correct nasal tip drooping. So, correction of nasal tip drooping varies according to the cause of the deformity, and an exact diagnosis of the underlying anatomical factors is important. 1,11 The static problems of alar cartilage and septal cartilage such as aggressive alar cartilage resection, too much layers of onlay grafts, interrupted strip techniques, and radical reduction of the anterior septal angle or the anterior nasal spine are typical interventions causing secondary nasal tip drooping. 12 Also, the elimination of dynamic pulling forces on the nasal tip by the underlying muscles may cause secondary nasal tip drooping. 12
We performed different operative techniques according to the cause of the nasal tip drooping. Primary nasal tip drooping originates from long and vertically oriented lateral crura. Therefore, we performed a conservative cephalic resection of LLC to increase the tip rotation and then used a columellar strut graft with onlay graft in order to support the medial crura and improve nasal tip projection. On the other hand, in patients with secondary nasal tip drooping, we removed the augmentation material and released the alar cartilages from the surrounding scar tissue. With the double-layered strut graft, we rotated the nasal tip cephalically with/without onlay grafts. Also, a 2-piece implant using silicone and cartilage was very effective in correcting nasal tip drooping on the basis of our experience. We suggest that primary and secondary nasal tip drooping should be distinguished and managed in distinct ways. However, although the cephalic resection of LLC is a well-known method of narrowing and rotating the nasal tip cephalically, we should keep in mind that the width and thickness of LLC are not quite sufficient for the cephalic resection of the lateral crura for cephalic rotation, due to the weak structural tip support of the small and thin LLCs in Asians. 13
Limitations
In our study, there are several limitations to the conclusions. First, in group 2, we didn’t consider the surgical procedures that significantly weaken nasal tip, besides alloplastic implant. It could act as a confounding variable. Second, it is difficult to determine the statistical significance of parametric statistics because the sample size is too small. Third, ideal anthropometric measurements of a nose differs between a man and a woman, but the number of men is too small (8 and 2 in group 1 and 2, respectively). Fourth, by methodology design, distinct surgical methods were used between 2 groups. So, 2 different outcomes were achieved among 2 different cohorts who were each treated differently with differing surgical treatment techniques.
Conclusion
We found that an oversized one-piece alloplastic implant from the glabella to the dome of nasal tip could induce secondary nasal tip drooping. The major strength of our study is that we compared pre- and postoperative structural characteristics between primary nasal tip drooping and secondary nasal tip drooping caused by an oversized one-piece alloplastic implant. Based on our results, we suggest that distinct methods for correction should be considered in primary and secondary nasal tip drooping.
Footnotes
Authors’ Note
This study was exempted from institutional review board (IRB) review by the public IRB of the Ministry of Health and Welfare, Republic of Korea (P01-201503-21-006). Informed consent was obtained from all individual participants included in the study. Hyun Jin Min is now affiliated with Department of Otorhinolaryngology-Head andNeck Surgery, Chung-Ang University College of Medicine, Dongjak-gu, Seoul, Korea.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP) (NRF-2017R1A1A1A05000760 to Hyun Jin Min).