
Abstract
Background:
To retrospectively assess the impact of prognostic nutritional index (PNI) on survival outcomes of patients with locoregionally advanced nasopharyngeal carcinoma (LA-NPC) treated with concurrent chemoradiotherapy (CCRT).
Methods:
This study incorporated 154 patients with LA-NPC who received exclusive cisplatinum-based CCRT. Receiver operating characteristic (ROC) curve analysis was utilized for accessibility of pretreatment PNI cutoffs influencing survival results. The primary end point was the interaction between the overall survival (OS) and PNI values, while cancer-specific survival (CSS) locoregional progression-free survival (LR-PFS), distant metastasis–free survival (DMFS), and PFS were the secondary end points.
Results:
A rounded PNI cutoff value of 51 was identified in ROC curve analyses to exhibit significant link with CSS, OS, DMFS, and PFS outcomes, but not LR-PFS. Patients grouping per PNI value (≥51 [N = 95] vs <51 [N = 49]) revealed that PNI < 51 group had significantly shorter median CSS (P < .001), OS (P < .001), DMFS (P < .001), and PFS (P < .001) times than the PNI ≥ 51 group, and the multivariate results confirmed the PNI < 51 as an independent predictor of poor outcomes for each end point (P < .05 for each). The unfavorable impact of the low PNI was also continued at 10-year time point with survival rates of 77.9% versus 42.4%, 73.6% versus 33.9%, 57.9% versus 27.1%, and 52.6% versus 23.7% for CSS, OS, DMFS, and PFS, respectively. Additionally, we found that PNI < 51 was significantly associated with higher rates of weight loss >5% over past 6 months (49.2% versus 11.6%; P = .002) compared to PNI < 51 group.
Conclusion:
Low pre-CCRT PNI levels were independently associated with significantly reduced CSS, OS, DMFS, and PFS outcomes in patients with LA-NPC treated with definitive CCRT.
Keywords
Introduction
Concurrent chemoradiotherapy (CCRT) is the current gold standard management option for patients presenting with locoregionally advanced nasopharyngeal carcinoma (LA-NPC). 1 Significant advances in diagnostic and staging tools and implementation of intensity-modulated radiotherapy (IMRT) to the treatment algorithm of LA-NPCs enhanced the locoregional tumor control rates. 2 -4 But consequently, distant metastasis (DM) turned into the leading failure pattern in such patients with over 20% DM rates. 4,5
Tumor (T) and node (N) components of the current tumor–node–metastasis (TNM) staging system represents for the current best quality level framework for treatment decision and outcome prediction of the patients with LA-NPC. However, this system accounts only for the local and regional tumor extent but disregards the considerable biological variations among the tumor- and host-related response factors. 6,7 Moreover, the remarkably distinct treatment outcomes observed between the patients with identical TNM stages, even after the same treatment conventions, render the predictive power of TNM framework flawed and underlines the pivotal significance of the identification of additional novel biological factors for more sophisticated prognostic stratification of patients with LA-NPC.
Growing evidence suggest that cancer-related malnutrition and inflammation enhance the local/regional tumor progression and widespread DM by altering the host immunity and tumor biology in unfavorable manners. 8 -11 The prognostic nutritional index (PNI), a combination of the serum albumin (Alb) concentration and total lymphocyte count (TLC) in peripheral blood, has been repeatedly shown to reliably reflect the magnitude of the systemic inflammation and the immunonutritional status of patients with many tumor types, including the pancreatic-, colorectal, gastric-, hepatocellular-, and lung cancers, malignant pleural mesothelioma, and glioblastoma multiforme. 12 -18 However, to date, very few studies have been reported to assess the prognostic and/or predictive value of PNI in patients with LA-NPC. 19 -23 In these studies, variable cutoffs those determined with various methodologies were utilized for discrimination of the outcomes usually with an end goal of 1 or 2 survival results. Hence, present retrospective study was designed to investigate the prognostic worth of pre-CCRT PNI values on the multiple survival end points of patients with LA-NPC and to determine the potential covariates which may correlate with PNI.
Methods
Study Population
The medical records of patients with LA-NPC treated with definitive CCRT by the Baskent University Medical Faculty Head and Neck Cancers Group between January 2007 and December 2015 were retrospectively reviewed. The eligibility criteria were histologically proven non-keratinizing (type 2) or undifferentiated (type 3) squamous cell carcinoma, age 18 to 80 years, Karnofsky Performance Score ≥70, clinical/radiological proof of T2-4N0-3M0 or T1-4N1-3M0 disease stage according to the TNM staging system (seventh edition), body mass index ≥20.0 kg/m2, no prior chemotherapy/RT history, at least 1 cycle of platinum-based chemotherapy administered during the CCRT course, available baseline fluorodeoxyglucose-positron emission computerized tomography (PET-CT) and chest CT scans, no evidence of brain metastasis on magnetic resonance imaging (MRI) scans obtained over past 1 month, available RT and chemotherapy charts, available complete data of baseline complete blood count and biochemistry tests, and available records of pretreatment and follow-up head and neck clinical examinations, MRI and PET-CT scans.
The retrospective study protocol was designed in accordance with the guidelines outlined in the Declaration of Helsinki and approved by the institutional Ethics Committee.
Concurrent Chemoradiotherapy
All patients received definitive CCRT with the RT and chemotherapy doses as reported previously. 24 In brief, the RT technique was 3-dimensional conformal RT (3D-CRT) between January 2007 to June 2011 and IMRT thereafter, administered in a daily fractionation basis: 5 days/week, for 7 weeks. Anti-emetic and nutritional support was provided as indicated. Prophylactic nasogastric tube or percutaneous endoscopic gastrostomy was not utilized, as our institutional treatment approach did not dictate their standard usage for such patients.
Prognostic Nutritional Index Measurements
PNI was calculated by utilizing the total blood count and biochemistry tests obtained on the first day of CCRT with using the Onodera’s original formula 25 : PNI = 10 × serum Alb (g/dL) + 0.005 × TLC (per mm3). As PNI reflects the nutritional and immune status of patients with cancer, patients on steroid treatment or with chronic or infectious diseases which may potentially alter the Alb and/or TLC levels were excluded from the analyses to avoid artificial alterations on outcomes.
Toxicity and Treatment Response Assessments
Acute toxicity was assessed weekly (or more frequently) during the CCRT, while patients were regularly examined every 3 months for the first 2 years, every 6 months between the 3 and 5 years, and annually (or more often) for subacute and chronic toxicities after the completion of CCRT. Each toxic event was scored according to the Common Terminology Criteria for Adverse Events v3 and reflected the worst grade ascertained.
Although the study design was retrospective, treatment response was assessed prospectively within the aforementioned visit intervals for chronic toxicity evaluations. All patients underwent detailed endoscopic examinations at each follow-up visit for evaluation of the index NPC and other head and neck regions in order to ascertain any local/regional recurrences and the emergence of second head and neck cancers. First imaging evaluations were obtained at the 90-days follow-up visit utilizing restaging PET-CT scans and scored according to the EORTC-1999 guidelines (the PET Response Criteria in Solid Tumors for patients evaluated after 2009). Positron emission computerized tomography scans were replaced by the head and neck CT and/or MRI whenever a complete metabolic response was ascertained. If indicated, restaging neck/abdominal ultrasonography or abdominal CT, chest CT, brain MRI, and bone scintigraphy were additionally utilized. Salvage interventions such as re-irradiation, systemic chemotherapy, neck dissection, or their combinations were offered to patients with confirmed local and/or regional relapses or distant metastases, as indicated.
Statistical Analysis
The primary objective was the association between pre-CCRT PNI values and overall survival (OS) defined as the interval between the first day of CCRT and death/last follow-up. Secondary objectives comprised the associations between pre-CCRT PNI values and cancer-specific survival (CSS), locoregional progression-free survival (LR-PFS), DM-free survival (DMFS), and PFS: the interval between the first day of CCRT and exclusive NPC-related deaths (for CSS), or progression/recurrence at the nasopharynx and/or ipsi-/contralateral neck or death/last follow-up (for LR-PFS), or any distant relapses or nonregional lymph nodes or death/last follow-up (for DMFS), or any disease progression or death/last follow-up (for PFS), respectively.
Receiver operating characteristic (ROC) curve analyses were utilized for testing the ability of pre-CCRT PNI levels to discriminate CSS, OS, LR-PFS, PFS, and DMFS. Means, medians, and ranges were used to describe continuous variables, while frequency distributions were used for categorical variables. The frequency distributions and their correlations among different groups were compared by χ2 tests, Student t tests, Pearson exact test, or Spearman correlations as appropriate. The interactions between the potential risk factors and CSS, OS, LR-PFS, PFS, and DMFS were assessed with Kaplan–Meier estimates and log-rank tests. Multivariate analyses incorporated only the factors exhibiting significance in univariate analyses and were tested by the Cox proportional hazards model. Although any 2-sided P values <.05 were considered significant for comparisons between any 2 groups, the noteworthiness of within-subgroup treatment influences was adjusted for multiplicity by utilizing Bonferroni corrections for comparisons between 3 or more subgroups in an effort to limit the chance-related false-positive discoveries.
Results
Present retrospective database search revealed 226 patients with NPC, but 72 of them were excluded from the analyses: for receiving upfront induction chemotherapy (N = 68) and lost to follow-up just after completion of CCRT (N = 4), respectively. Therefore, 154 patients were left eligible for this current analysis. Baseline patient and disease characteristics were as demonstrated in Table 1. In general, the CCRT scheme was relatively well tolerated with an overall grade 3 (N = 81; 52.6%) and 4 (N = 28; 18.2%) acute toxicity rate of 70.8% (N = 109). Only 2 (1.3%) treatment-related deaths due to intractable necrotic nodal-cutaneous fistula (n = 1) and tracheoesophageal fistula–related aspiration pneumonia (n = 1) were reported at respective 5th and 16th months of follow-up. During the CCRT, 112 (72.7%) patients received 3 courses of concurrent chemotherapy, and additionally, 81 (52.6%) were able to receive 1 (N = 18; 11.7%) or 2 (N = 63; 40.9%) adjuvant chemotherapy courses.
Baseline Characteristics of 154 Patients With Locoregionally Advanced Nasopharyngeal Carcinoma.
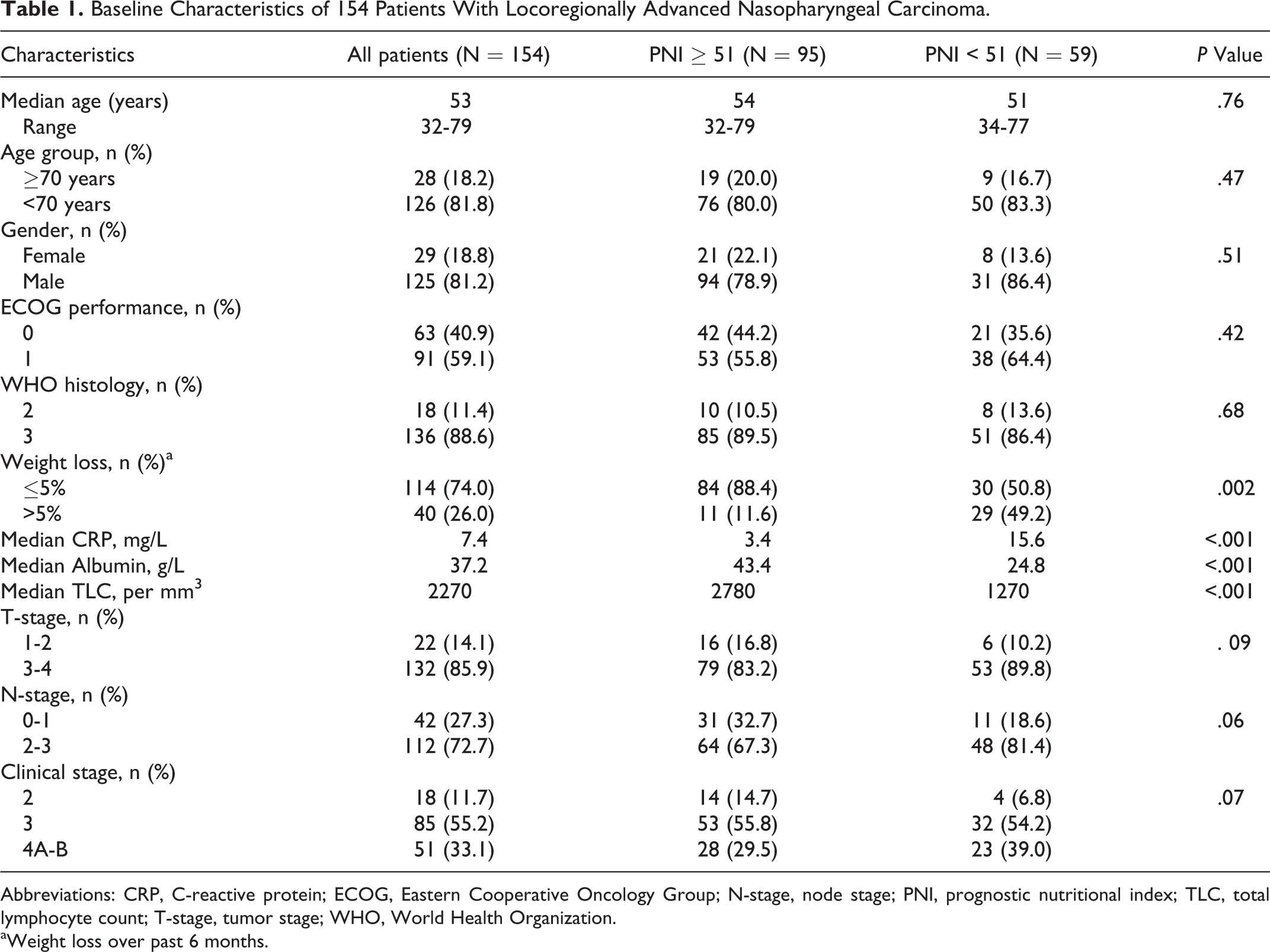
Abbreviations: CRP, C-reactive protein; ECOG, Eastern Cooperative Oncology Group; N-stage, node stage; PNI, prognostic nutritional index; TLC, total lymphocyte count; T-stage, tumor stage; WHO, World Health Organization.
aWeight loss over past 6 months.
At a median 60.3 months (range: 5.2-137.4) of the follow-up period, 115 (74.7%) patients were still alive with 86 (54.4%) of them being free of disease progression. The median CSS, OS, and LR-PFS times were not reached for the entire cohort, while the median DMFS and PFS times were 102.3 months (95% confidence interval [CI]: 79.1-125.5) and 96.4 months (95% CI: 75.7-120.1), separately. Respective 5- and 10-year survival rates were 81.1% and 74.7% for CSS, 72.6% and 65.3% for OS, 60.9% and 53.9% for LR-PFS, 67.6 and 49.4% for DMFS, and 53.8% and 45.1% for PFS. Actuarial 10-year locoregional control and distant relapse-free rates were 89.0% and 78.6%, respectively.
The median PNI value for the whole study group was 50.6 (95% CI: 45.0-56.2). Receiver operating characteristic curve analyses identified the 50.9 (area under the curve [AUC]: 74.1%, sensitivity: 75.3%, specificity: 70.7%), 50.7 (AUC: 72.4%, sensitivity: 71.3%, specificity: 68.9%), 50.8 (AUC: 78.5%, sensitivity: 77.6%, specificity: 75.1%), and 51.2 (AUC: 72.7%, sensitivity: 73.1%, specificity: 71.3%) values as the cutoffs demonstrating significant association with the CSS, OS, DMFS, and PFS outcomes, respectively (Figure 1), while no particular discriminatory cutoff value was identifiable for LR-PFS. Because all 4 cutoffs were numerically very close, the study cohort was dichotomized into 2 groups at a rounded cutoff value of 51.0 for further analyses: group 1: PNI ≥ 51.0 and group 2: PNI < 51.0. Comparisons of the baseline demographics revealed that, although most factors were almost similarly distributed between the 2 PNI groups, baseline weight loss (WL) > 5% over past 6 months (49.2% vs 11.6%; P = .002) and the C-reactive protein measures were conversely higher (3.4 vs 15.6 mg/L; P < .001) in the PNI < 51.0 group, while the median measures of Alb (43.4 vs 24.8 g/L; P < .001) and total TLC (2780 vs 1270/mm3; P < .001) were significantly higher in the PNI ≥ 51.0 group (Table 1). As depicted in Figure 2 and Table 2, comparative survival analysis exhibited that the PNI ≥ 51.0 group had significantly longer median CSS (P < .001), OS (P < .001), DMFS (P < .001), and PFS (P < .001) durations than their PNI < 51.0 counterparts. Similarly, the respective 5- and 10-year survival rates were also superior in PNI ≥ 51.0 than the PNI < 51.0 group for each survival end point (Table 2).
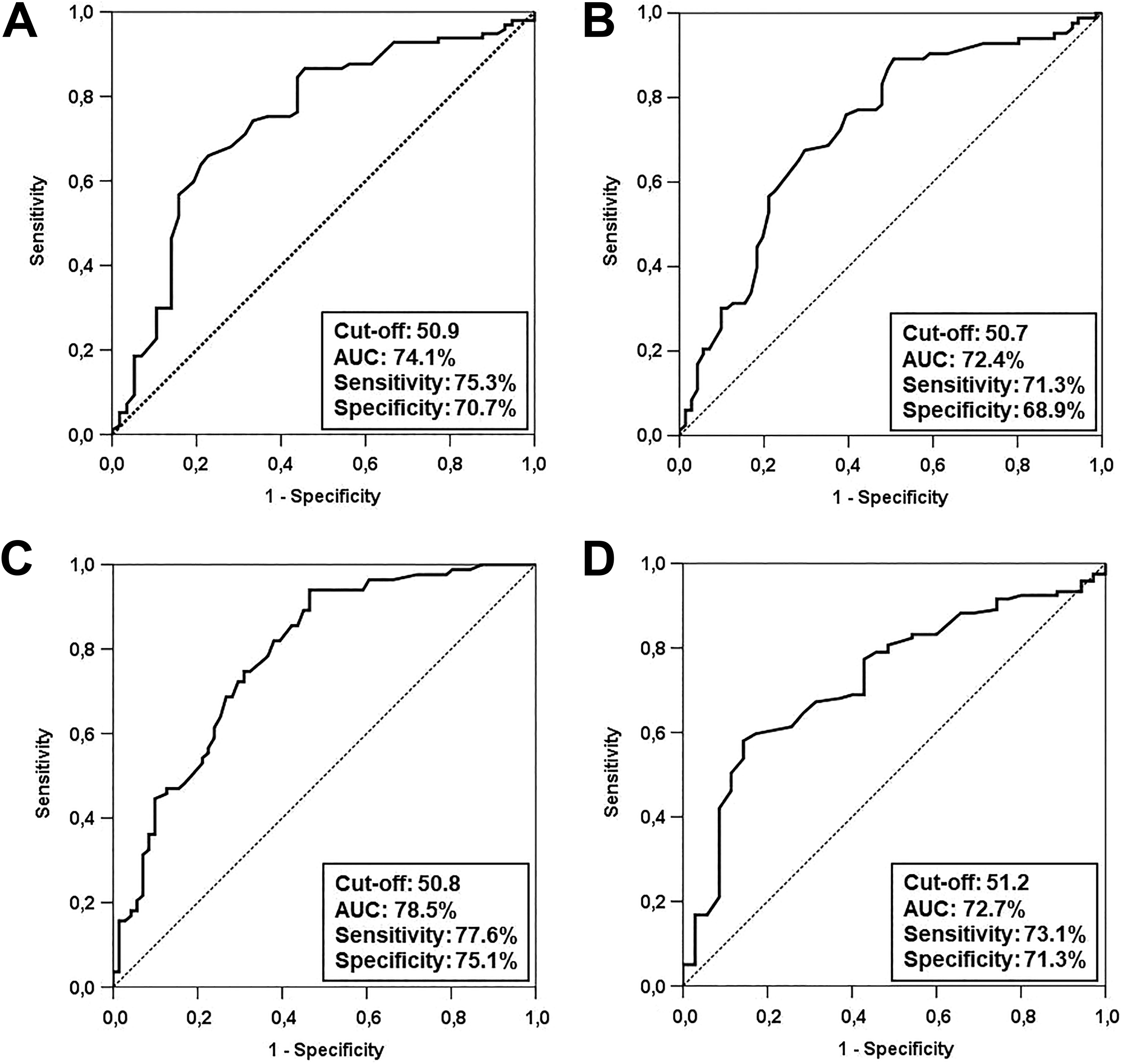
Outcomes of receiver operating characteristic curve analyses: (A) cancer-specific survival, (B) overall survival, (C) distant metastasis-free survival, (D) and progression-free survival.
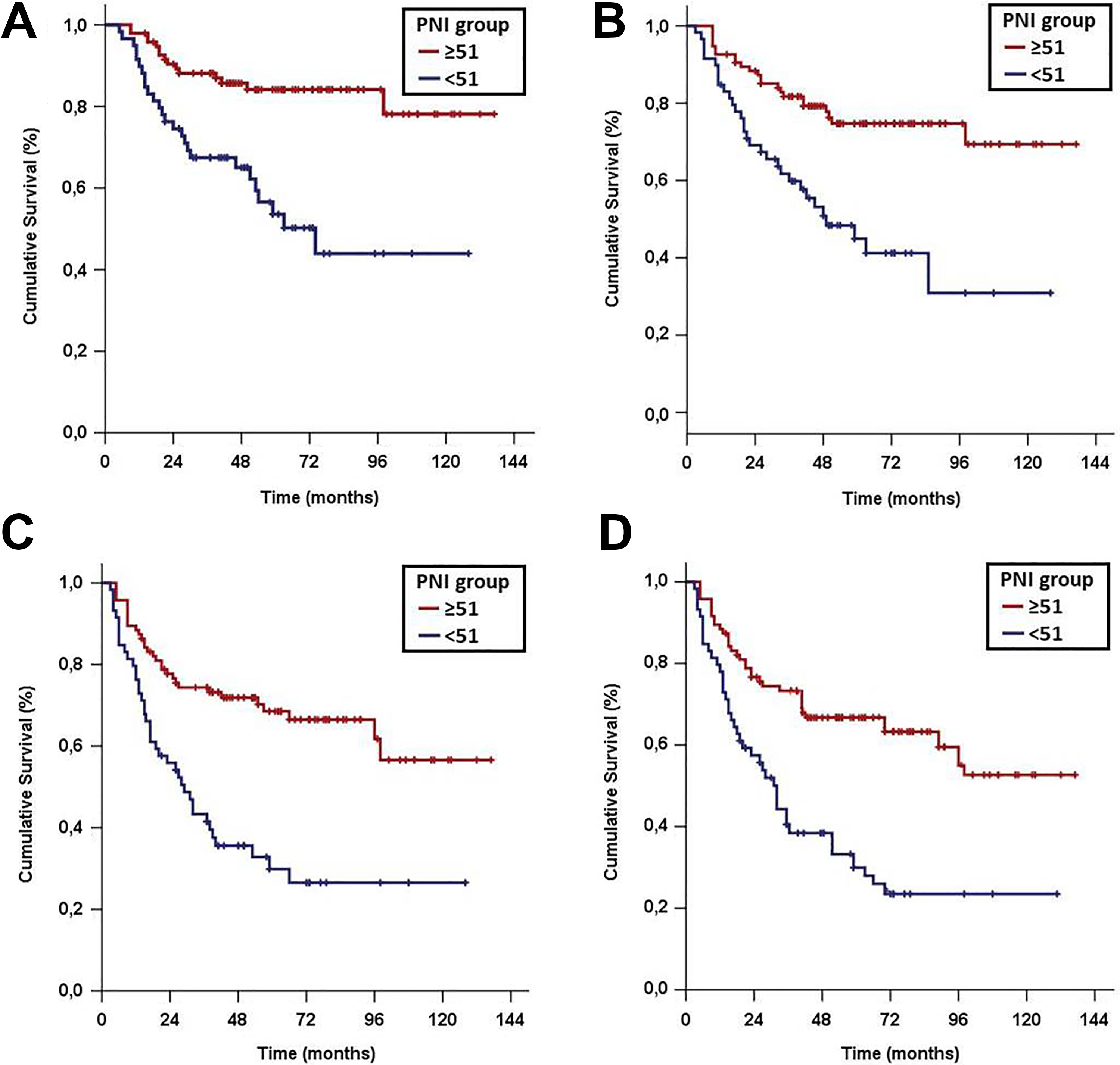
Survival results according to pretreatment PNI groups (red line: PNI ≥ 51 and dark blue line: PNI < 51): (A) cancer-specific survival, (B) overall survival, (C) distant metastasis-free survival, and (D) progression-free survival. PNI indicates prognostic nutritional.
Median and Long-Term Survival Outcomes According to PNI Groups.
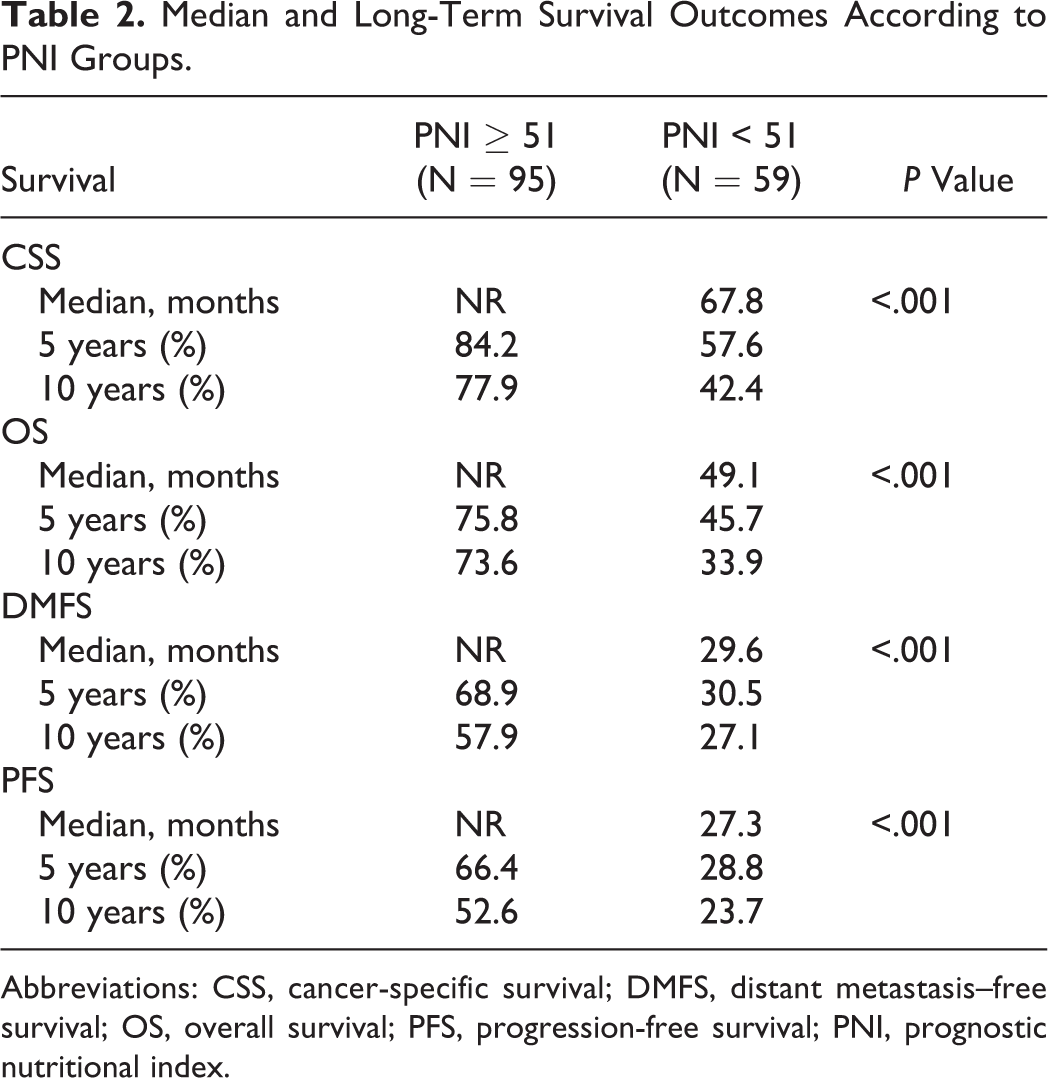
Abbreviations: CSS, cancer-specific survival; DMFS, distant metastasis–free survival; OS, overall survival; PFS, progression-free survival; PNI, prognostic nutritional index.
Outcomes of univariate analyses demonstrated that the lower T-stage (2-3 vs 4), lower N-stage (0-1 vs 2-3), lower TNM stage (4A/B vs 2-3), lower WL over past 6 months (≤5% vs >5%), and higher pretreatment PNI (≥51.0 vs <51.0) were related with significantly inferior CSS, OS, DMFS, and PFS outcomes (Table 3). Results of multivariate analyses restricted to the covariates exhibiting univariate significance revealed that each variable retained their independent significance for each survival end point (Table 3).
Outcomes of Uni- and Multivariate Analysis.
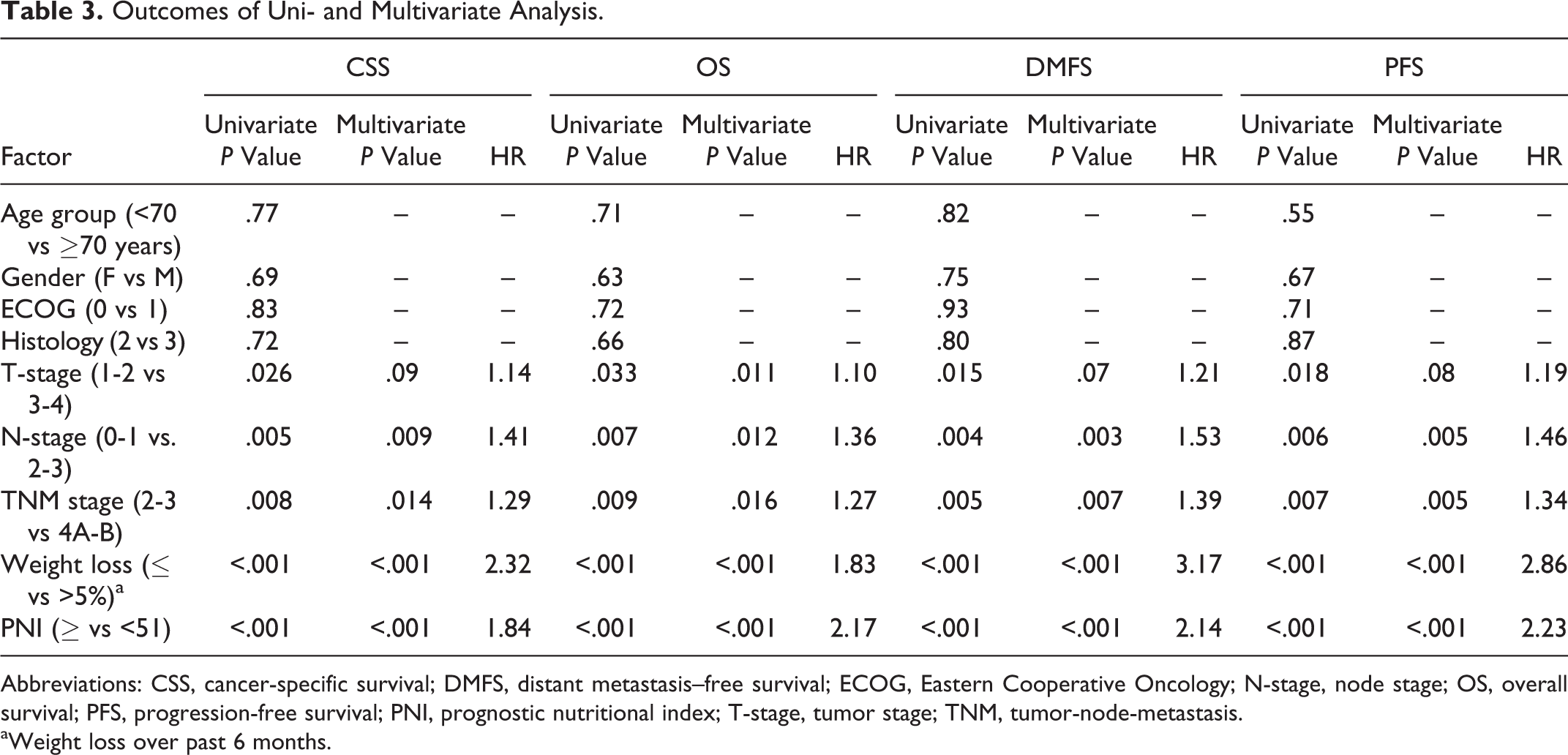
Abbreviations: CSS, cancer-specific survival; DMFS, distant metastasis–free survival; ECOG, Eastern Cooperative Oncology; N-stage, node stage; OS, overall survival; PFS, progression-free survival; PNI, prognostic nutritional index; T-stage, tumor stage; TNM, tumor-node-metastasis.
aWeight loss over past 6 months.
Discussion
Present retrospective cohort analysis investigated the prognostic value of pretreatment PNI on survival outcomes of 154 patients with LA-NPC treated with exclusive CCRT, and its results exhibited that PNI < 51 was strongly and independently associated with significantly inferior CSS, OS, DMFS, and PFS outcomes in this patients group. Besides confirming the prognostic utility of PNI in patients with LA-NPC undergoing exclusive CCRT, present results also discovered a significant correlation between PNI < 51 and WL > 5% over the past 6-month pre-CCRT period.
Besides the well-established genetic basis for cancer development, growing evidence has demonstrated that the systemic inflammation plays crucial roles in survival and proliferation of tumor cells, neoangiogenesis, resistance to apoptosis, escape from the immune system, metastasis to regional and distant sites, and resistance to therapies. 26,27 Therefore, overall, systemic inflammation supports the carcinogenesis, progression, and metastases steps in many solid and hematologic cancers. 28 Principally based on this basic evidence, recent studies focused on the prognostic value of several blood markers and their various combinations including the platelet to lymphocyte ratio, neutrophil to lymphocyte ratio, Glasgow prognostic score and its modified form, systemic immune-inflammation index, and PNI. 29 -35 Before its wide acceptance as an immunonutritional marker in many cancers including the NPC, the PNI was first utilized by Onodera et al in 1984 for prediction of postoperative complication risks in gastrointestinal cancers. 25 Although the low PNI values below various cutoffs have been almost consistently demonstrated to be strongly linked with poorer clinical outcomes in patients with NPC, yet most such studies were highly heterogeneous with regards to the disease stages and treatment modalities, and unfortunately focused on just 1 or 2 survival end points. Thus, the present study was designed to investigate the clinical utility of PNI in terms of CSS, OS, LR-PFS, DMFS, and PFS in a relatively more homogenous LA-NPC group treated with exclusive CCRT.
The first vital finding of our study was the exhibition of a strong relationship between the low PNI values and WL > 5% over the past 6 months. Acute phase reactants Alb and CRP are well-recognized factors to be associated with a hypercatabolic state and resultant WL in patients with cancer either in the pre-cachectic or cachectic periods. In consequence, both low Alb and high CRP levels were incorporated to the cachexia definition of Washington Consensus reported by Evans et al in 2008. 36 In our study, we observed significantly lower Alb and conversely higher CRP levels in the PNI < 51 group compared to its PNI ≥ 51 counterpart. Probably as a consequence of this observation, meeting the major diagnostic criteria of Delphi Consensus’ cancer cachexia definition (WL > 5% over the past 6 months in the absence of simple starvation), the rate of WL > 5% over the past 6 months was significantly higher in the PNI < 51 group (49.2% vs 11.6% for PNI ≥ 51; P = .002). 37 Previously, McMillan et al noted that the CRP and Alb concentrations were inversely correlated in many tumor types, that any increase in CRP was almost always accompanied with decreased Alb concentrations, as observed in our study. 38 Hence, the demonstration of a significant connection between the WL > 5% over the past 6 months pre-CCRT period and low PNI values appears to be mainly associated with low Alb levels, which is the common factor shared by increased WL and decreased PNI status on the basis of a same chronic systemic inflammatory condition.
In this research, besides the other well-recognized traditional prognostic factors including the higher T- and N- and TNM-stage, and WL > 5% over past pre-CCRT 6 months, the results of multivariate analysis revealed that pre-CCRT PNI < 51 was strongly and independently associated with significantly inferior CSS, OS, DMFS, and PFS, but not LR-PFS. This finding accords well with the previous NPC studies proposing the low PNI levels (range: 49-55) as a predictor of poor prognosis with regard to the systemic disease control and survival end points. 19 -23 Although our results appear to confirm these studies, yet we additionally demonstrated a notable prognostic worth for PNI in the prediction of the CSS outcomes alike with the recent study by Miao et al. 20 The actuarial 89% locoregional tumor control rate at 10-year observed in our study and nearly 90% in other studies all together underline the critical importance of evaluation of CSS as a primary end point in patients with LA-NPC, as such cases achieve long-term locoregional control rates particularly with the use IMRT as a component of CCRT. Therefore, such analysis may prove valuable in-through evaluation of the exact value of novel prognostic markers in these patients populations by the elimination of the deaths related with the other causes rather than the index LA-NPC, which may account for as much as 40% of all deaths. 39
Our current investigation has certain limitations. First, the present results represent the outcomes of a retrospective, single-institutional relatively small cohort analysis which might be biased by some unpredictable factors common to such studies. Therefore, our results might have been influenced in any way because of unavoidable unequal distributions of unidentified clinicopathological factors among the eligible patients. Second, although the measures of Alb and TLC may demonstrate significant variations during the course of treatment, yet we restricted our investigation just to the baseline PNI and did not evaluate the PNI kinetics during or after the CCRT, which might also have notable impacts on outcomes. Supporting this rational anticipation, in a small-scale recent study of 70 NPCs, Cho et al investigated whether the minimum absolute lymphocyte count (ALC) during RT/CCRT could predict clinical outcomes and demonstrated that the minimum ALC with a cutoff 245 cells/μL had significant influences on outcomes. 40 The 5-year CSS and PFS for patients with minimum ALC ≥ 245 versus <245 were 88.1% versus 60.8% (P = .004) and 71.2% versus 35.2% (P = .004). Furthermore, all of the 10 patients with minimum ALC <120 experienced disease progression. Thus, PNI kinetics deserves to be further studied in future PNI investigations. And third, the current outcomes are relevant only for a select patients with LA-NPC group presenting with ECOG 0-1 and pretreatment BMI ≥ 20 kg/m2 who underwent the same CCRT protocol except for the time-dependent changes in RT techniques. Hence, our results ought to be interpreted with caution and should not be accepted as authoritative to all LA-NPC populations until the outcomes of prospectively designed larger scale PNI studies become available.
Conclusions
The outcomes of current retrospective research confirmed the usefulness pretreatment PNI in the stratification of patients with LA-NPC into 2 groups with distinctive CSS, OS, DMFS, and PFS following definitive CCRT. Therefore, the immunonutritional biomarker PNI with its easy to calculate, reproducible, and inexpensive test characteristics may supplement the standard TNM classification in further prognostic stratification of radically treated patients with LA-NPC.
Footnotes
Authors’ Note
Erkan Topkan and Ugur Selek contributed to conception and design. Nur Y. Ekici, Yurday Ozdemir, Ali Ayberk Besen, Huseyin Mertsoylu, and Ahmet Sezer contributed to collection and assembly of data. Erkan Topkan, Ugur Selek, Yurday Ozdemir, Ali Ayberk Besen, Ahmet Sezer, and Huseyin Mertsoylu contributed to data analysis and interpretation. Erkan Topkan and Ugur Selek contributed to manuscript writing. All authors contributed in Final approval of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.